Nuclear Receptors
Nuclear Receptors: Ligand-Regulated Transcription Factors:
Nuclear receptors (NRs) are intracellular ligand-activated transcription factors.
They regulate gene expression in response to lipophilic signalling molecules such as:
Steroid hormones (e.g., oestrogens, glucocorticoids)
Thyroid hormones
Retinoids and vitamin D metabolites
They are essential regulators of development, metabolism, reproduction, and homeostasis.
Cellular Localisation:
In contrast to membrane-bound receptors (e.g., ion channels and G protein-coupled receptors), nuclear receptors are located within the cytoplasm or nucleus.
Their ligands are hydrophobic, enabling passive diffusion through the plasma membrane.
General Mechanism of Action:
Ligand Entry:
Lipophilic ligand diffuses across the plasma membrane.
Ligand Binding:
Ligand binds to its cognate nuclear receptor, inducing a conformational change.
Dimerisation:
The receptor forms a homodimer or heterodimer, enhancing DNA-binding affinity.
Nuclear Translocation:
The receptor–ligand complex translocates to the nucleus if initially cytoplasmic.
DNA Binding:
The complex binds to specific DNA sequences termed Hormone Response Elements (HREs) within the promoter region of target genes.
Transcriptional Regulation:
Coactivator proteins (e.g., SRC-1, CBP/p300) promote transcription.
Corepressor proteins (e.g., NCoR, SMRT) inhibit transcription.
The resultant outcome (gene activation or repression) depends on the cellular context and cofactor availability.
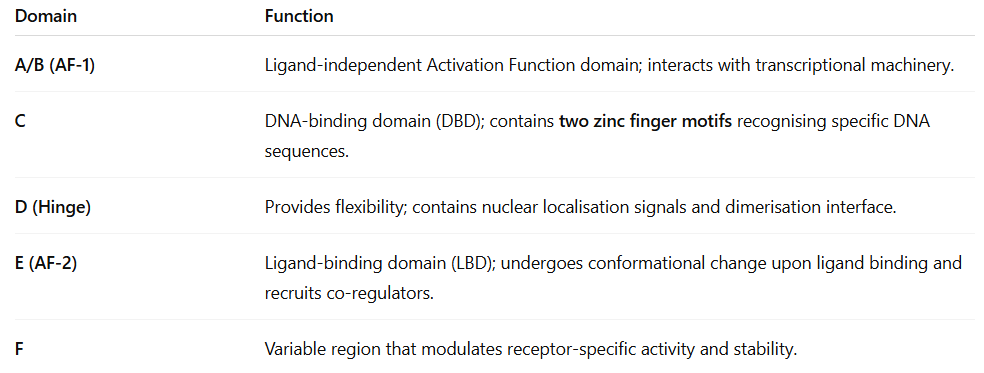
Structural Organisation of Nuclear Receptors:
Each receptor is a single polypeptide chain comprising several conserved domains:
The Oestrogen Receptor (ER):
Ligand and Subtypes:
Primary ligand: 17β-oestradiol (E2).
Receptor subtypes:
ERα: Predominantly expressed in reproductive tissues (e.g., uterus, breast).
ERβ: Found in bone, brain, and cardiovascular tissues.
Subtype expression contributes to tissue-specific pharmacological responses.
— — — — —
Mechanism of Action:
Oestradiol diffuses through the plasma membrane due to its lipophilic nature.
It binds to the oestrogen receptor in the cytoplasm or nucleus.
Ligand binding induces receptor dimerisation.
The receptor–ligand complex binds to Oestrogen Response Elements (EREs) within target gene promoters.
Recruitment of coactivators stimulates transcription of oestrogen-responsive genes, while corepressors suppress transcription.
— — — — —
Physiological Roles of Oestrogen:
Regulation of female secondary sexual characteristics (e.g., breast development, fat distribution).
Maintenance of the menstrual cycle and fertility.
Promotion of bone growth and maintenance.
In males, contributes to spermatogenesis and sperm maturation.
— — — — —
Clinical Relevance:
Many breast cancers are oestrogen receptor-positive (ER⁺) and depend on oestrogen signalling for proliferation.
Selective Oestrogen Receptor Modulators (SERMs) (e.g., tamoxifen) exhibit tissue-specific agonist/antagonist activity:
Antagonist in breast tissue → inhibits tumour growth.
Agonist in bone → preserves bone mineral density.
The tissue specificity arises from differing patterns of coactivator and corepressor expression in various cell types.
The Glucocorticoid Receptor (GR):
Ligands and Function:
Endogenous ligand: Cortisol.
Synthetic analogues: Dexamethasone, beclomethasone, prednisolone.
Primary functions:
Regulation of metabolic homeostasis.
Mediation of anti-inflammatory and immunosuppressive effects.
— — — — —
Mechanism of Action:
Glucocorticoid diffuses across the plasma membrane.
Binds to cytoplasmic GR complexed with heat shock proteins (HSP90, HSP70).
Ligand binding displaces HSPs and induces receptor dimerisation.
The activated receptor translocates into the nucleus.
GR binds to specific Glucocorticoid Response Elements (GREs) in DNA.
Regulates transcription through:
Transactivation: Upregulation of anti-inflammatory genes (e.g., Annexin-1, IL-10).
Transrepression: Inhibition of pro-inflammatory genes (e.g., IL-1β, TNF-α, COX-2).
— — — — —
Physiological and Pharmacological Effects:
Anti-inflammatory and immunosuppressive:
Inhibit cytokine and chemokine production.
Decrease vascular permeability.
Suppress leukocyte migration.
Clinical applications:
Treatment of asthma, rheumatoid arthritis, dermatitis, inflammatory bowel disease, and allergic reactions.
Adverse effects (with chronic use):
Hypertension, mood alterations, hyperglycaemia, weight gain, and osteoporosis.