Week 14: Substance-Related Disorders
Introduction to Substance-Related Disorders
Substance use disorders are significant national health problems.
In 2021, there were 29.5 million people in the United States aged 12 and older with an alcohol use disorder.
Alcohol-Related Statistics:
Over 140,000 alcohol-related deaths annually.
Alcohol-related death is the fourth leading preventable cause of death in the U.S.
Withdrawal can also be life-threatening.
Be able to identify intoxication (breath, slurred speech, unsteady gait), and recognize the signs of withdrawal, such as tremors, anxiety, and seizures, which highlight the importance of early intervention and treatment.
31% of driving fatalities are alcohol-related.
Global impact: 5.1% of the global burden of disease and injury is due to alcohol use.
Impact on children and families: 8.7 million children live with a parent who has a substance use disorder.
Opioid Crisis and CDC Recommendations
The opioid crisis in the U.S. results in 300 deaths daily from opioid overdoses and affects all demographics.
CDC Recommendations:
Educate on the potency of illicitly manufactured fentanyl.
Address the unintentional consequences of polysubstance use.
Promote the lifesaving use of naloxone to reverse opioid overdose.
Reduce stigma surrounding recovery and treatment options.
Role of Naloxone:
200% increase in naloxone dispensing since 2018.
Naloxone has saved thousands of lives and encourages legislative support for its availability.
Can be given intranasal, IV, or IM.
Potency of Illicitly Manufactured Fentanyl
Fentanyl is a highly potent synthetic opioid that is often mixed with other substances, increasing the risk of overdose.
Challenges with Fentanyl:
Difficult to detect in substances.
Small amounts can be lethal.
Awareness and Education:
Public education about the dangers of fentanyl is critical.
Training for first responders is essential for handling fentanyl-related incidents.
Importance of Reducing Stigma Around Recovery and Treatment
Stigma as a barrier: Fear of judgment prevents individuals from seeking help.
Strategies to reduce stigma:
Public education campaigns.
Promoting positive stories of recovery.
Benefits of reducing stigma:
Encourages more individuals to seek treatment and ultimately improves public health outcomes.
Role of the American Medical Association (AMA) in the Opioid Crisis
AMA's Perspective: The crisis may have been initiated by the overprescription of opioid analgesics.
Recent Trends:
Decrease in prescription opioid use.
Rise in heroin and illicit synthetic opioid use.
AMA Recommendations:
Support for naloxone use and availability.
Policy initiatives aimed at comprehensively addressing the opioid crisis.
Types of Substance Misuse
Substance use includes terms for both misuse and dependence, encompassing various substances, both legal (e.g., alcohol, prescription medications) and illegal.
Polysubstance use refers to the misuse of more than one substance.
Definitions:
Misuse: Inconsistent with medical/social norms, leads to negative consequences; problems in social, vocational, or legal areas.
Simply means incorrect use, but not necessarily dependent on it.
Dependence: Encompasses addiction, tolerance, withdrawal, and unsuccessful attempts to quit.
This is a psychological need for a substance.
Misuse and dependence are often viewed as clinically similar.
Symptoms and Effects of Substance Use
Intoxication: The use of a substance resulting in maladaptive behavior.
Withdrawal Syndrome: Negative psychological and physical reactions when substance use decreases or halts. Some symptoms can be life-threatening.
Detoxification (Detox): The process of safely withdrawing from a substance.
Substance-Induced Disorders: Includes psychosis and mood disorders.
Onset and Clinical Course of Alcohol Use Disorder
Research heavily focuses on alcohol due to its legality and prevalence.
Prognosis: Initially unclear, as studies often involve individuals seeking treatment.
Initial Intoxication: Typically begins during adolescence (ages 12-14), with minor issues appearing in late teens and severe problems emerging between mid-20s and mid-30s (due to easier access as people age).
Common Issues: Relationship breakups, arrests, withdrawal symptoms, health problems, work/school interference, blackouts, and tolerance development.
Blackout: Functioning without conscious awareness or memory (risk of harm to self, others, or abuse).
Tolerance: Needing more alcohol for the same effect; tolerance breaks occur where small amounts induce intoxication.
Later Course and Relapse in Alcohol Use Disorder
Later Stages: Often characterized by periods of abstinence or controlled drinking that follow crises.
Temporary control can lead to increased intake and further issues; relapse rates can range from 40% to 80% because this is a chronic disorder.
Nearly half relapse within a year post-treatment, with success linked to abstinence goals, motivation, and relapse prevention strategies.
Spontaneous Remission: Some individuals achieve recovery without formal treatment, often triggered by crises or commitments to loved ones.
Types of Drugs and Their Classification
CNS Depressants: Include alcohol, cannabis, sedatives, and hypnotics.
Intended Effects: Decreased anxiety, sedation, drowsiness.
CNS Stimulants: Increased energy and euphoria, less clinical use due to high potential for misuse.
Common examples include amphetamines and cocaine (these are club/designer drugs when mixed with other drugs).
Cannabis: Changing legal status, with varying intended effects such as euphoria and pain management.
THC: associated with “high” or euphoric sensation.
CBD: does not have the same psychoactive effects, and stays in the body longer.
Excessive use can lead to long-term psychosis.
Hallucinogens: Distort perception and can lead to symptoms similar to psychosis.
Preferred treatment for intoxication: talking to the person, reassurance.
If danger to self and others, give haloperidol or benzodiazepines.
Inhalants: Commonly found in everyday products, intended for euphoria but leading to significant health risks.
Causes anoxia (damage to the brain), bronchospasms, and peripheral nerve injury.
Coping Strategies and Relapse Prevention
Discuss events leading to substance use in a nonjudgmental manner to identify patterns and triggers.
Positive Coping Strategies: Building stress management techniques like physical exercise, verbal expression, journaling, and meditation.
Manage Unstructured Time: Excessive free time can lead to substance use; planning purposeful activities can mitigate risks.
Social Skills Enhancement: Teaching and demonstrating appropriate social skills can improve self-esteem and reduce isolation.
Related Disorders
Gambling Disorder: Non-substance-related diagnosis with behaviors such as spending beyond means and inability to refrain from gambling.
Caffeine and Tobacco/Nicotine: Classified in the DSM-5 as not mental health problems per se, but potential dependencies.
Caffeine can mimic an amphetamine, given that it is a stimulant.
Substance-Induced Disorders: Symptoms such as substance-induced anxiety, psychosis, and mood disorders that may dissipate once the substance is eliminated.
Etiology of Substance-Related Disorders
Factors contributing to substance-related disorders include:
Biological and Genetic Factors: Genetic predispositions and neurochemical influences contributing to the risk of alcohol use disorder.
Psychological Factors: Family dynamics and coping mechanisms related to parental behavior can impact children's substance use risk.
Social and Environmental Factors: Cultural influences, laws, availability, and socio-economic status significantly affect substance use trends.
Cultural Considerations
Cultural attitudes toward substance use vary:
Islam prohibits alcohol, while wine is integral to Jewish culture/Catholisism.
The flushing reaction is linked to genes for alcohol metabolism, such as seen in people of Asian ancestry.
Native American tribes may use peyote in ceremonies, and alcohol use statistics show significant outcomes among Native Americans.
Treatment Approaches
Treatment post-detoxification is generally consistent across substances and should be tailored to the client's needs. Key elements include:
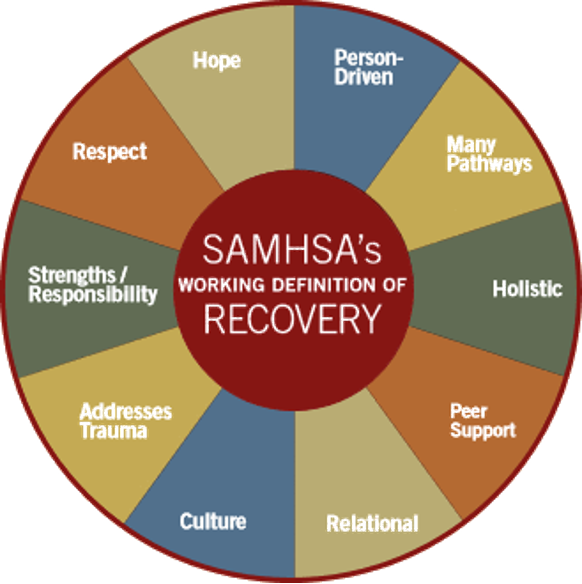
The Recovery Model: Focus on strengths (not weaknesses), community involvement, health, and purpose.
Support Services: Integrated programs addressing both substance use disorders and any co-occurring mental health issues.
Expected Findings in Substance Use Disorders
Screening Techniques: Open-ended questions to gather data about usage patterns, history, and withdrawal symptoms.
Focus on adverse effects, withdrawal, and how that affected their life.
Recognizing Cues: Observing physical and behavioral indicators of substance use.
Alcohol: Intoxication and Overdose
Intoxication Symptoms: Slurred speech, lack of coordination, impaired judgment, blackouts, and can interfere with memory.
Overdose Symptoms: Include vomiting, unconsciousness, and respiratory depression, potentially leading to cardiovascular shock and death.
Treatment for Overdose: May involve gastric lavage (pumping someone’s stomach) or dialysis and supportive care.
Alcohol: Withdrawal and Detoxification
Withdrawal Symptoms: Onset occurs 4 to 12 hours after cessation, including tremors, sweating, elevated HR and BP (non-compensating), insomnia, and anxiety.
If untreated, symptoms can progress to delirium tremens (DTs) and seizures.
Treatment varies based on severity (home vs. hospitalization).
Pharmacologic Treatment for Substance-Use Disorders
Primary Goals: Ensure safe withdrawal and prevent relapse.
Opioid Treatment: Utilization of clonidine for withdrawal, methadone for dependence, and naloxone for overdose.
Withdrawal is very uncomfortable, especially since opioids are a pain reliever and often lead to increased sensitivity to pain during the withdrawal process.
Alcohol Withdrawal Management: Benzodiazepines are commonly used for managing symptoms. Disulfiram is implemented for aversion therapy.
Disulfiram (Antabuse): An oral medication that inhibits the enzyme acetaldehyde dehydrogenase, causing unpleasant reactions when alcohol is consumed, thereby deterring the individual from drinking.
Side effects: fatigue, drowsiness, and gastrointestinal disturbances such as nausea and vomiting.
Dual Diagnosis in Substance Use Disorders
Co-occurrence of substance use with psychiatric conditions requires simultaneous treatment strategies to address all issues effectively.
Integrated treatment programs are essential for this demographic, highlighting stable housing, social support, and meaningful activities.
Community-Based Care
Treatment Settings: Can include outpatient facilities, recovery programs, and community resources.
Continuous follow-up services and ongoing support for clients and families significantly enhance recovery success.
Teaching Coping Strategies and Social Skills
Encouraging expressive outlets and developing social skills through practice in supportive settings can bolster self-esteem and reduce relapse risk.
Prevention Programs and Education
Community awareness and educational programs focused on alcohol misuse, particularly among youth and vulnerable populations.
Encouragement for lifestyle choices, including support for abstinence and healthy social interactions.
Factors Influencing Outcomes in Alcohol Use Disorder
Early onset, prolonged substance use, and comorbid mental illnesses negatively impact recovery outcomes. Regular contact with clients and validation of feelings aid in treatment adherence.
Conclusion and Review Strategies
Approach substance use disorders with understanding, empathy, and structured treatment plans that emphasize community support and continuous learning. Regular evaluations of progress and barriers ensure effective care and improved health outcomes.