N3 musculoskeletal.docx
It seems you haven't provided the book and chapter details. Please share the specific book and chapter you'd like me to summarize, and I'll be happy to help!
Pediatric Musculoskeletal disorders
Terms to Know
Trendelenburg Gait
Osteotomy- cutting of and removal of bone to improve bone function.
Arthrotomy- cutting into a joint to expose its interior
Hematogenously- involving, spread by, or arising in the blood.
Variations in Pediatrics
Immature musculoskeletal system
Rapid muscle growth (clumsiness)
Bones are more flexible and more porous
Males- testosterone release causes growth spurts and bulkier muscles
Females- laxer ligaments from female hormones
Shape of spine develops over time
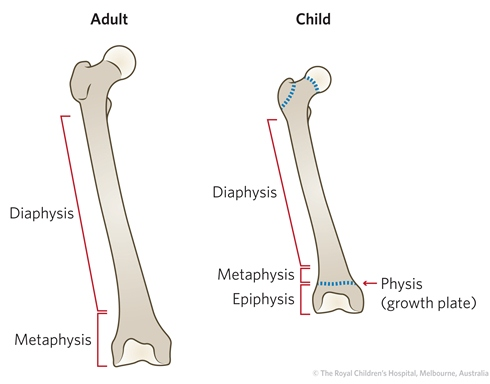
Epiphyseal region is vulnerable and weak. Fusing and maturing occurs in adolescence.
Quicker bone healing
Rich nutrient and blood supply
Increased remodeling- breaking down and forming new bone
Legs have a bowed appearance- in utero positioning. Resolves in 2-3 years with weight bearing.
Feet- in-toeing and flat. Also resolves with walking.
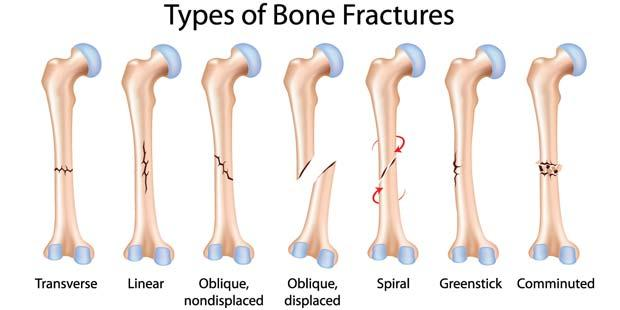
Fractures
When a bone is subjected to more energy than it can absorb
Forearm & wrist most common
Greenstick & buckle account for half
Childhood fractures are most frequently from accidental trauma.
Child < 2 yo with fractures & any child with spiral, rib, or humerus fractures should be evaluated for child abuse &/or underlying disorder.
Growth plate is most vulnerable portion of bone
Majority will heal with splinting alone
Casting is performed more for comfort and increased activity
Reduction (realigning) before casting will be needed with displaced fractures
More severe fractures may require traction, surgical reduction, &/or fixation
Swelling may occur initially after splinting. Delay casting until swelling subsides.
Do not attempt to straighten or manipulate
Inspect for bruising, erythema, swelling, deformity, limp, inability to bear weight. Palpate for point tenderness. Assess neurovascular status.
Immobilize injured limb above & below injury in most comfortable position with splint
Cold therapy to reduce swelling for first 48 hrs
Elevate injured extremity above level of heart
Frequent neurovascular checks
Assess pain using appropriate pain scale
Crutch walking teaching as needed
Encourage age appropriate protective equipment, such as wrist guards & shin guards
Casting
Immobilizes a bone that has been injured or a diseased joint, holds a bone in reduction when a fracture has occurred, and prevents/corrects deformities.
Plaster or fiberglass- drying time varies. Be careful to not make indentions during drying time!!
Gore-Tex lining available to make waterproof
FREQUENT neurovascular checks
Compartment syndrome- pressure builds up causing decreased blood flow, preventing nourishment and oxygen from reaching nerves and muscles causing tissue death.
Compartment Syndrome “5 P’s”
Monitor for
Increased pain
Decreased or absence of pulse/prolonged capillary refill (>3 seconds)
Cyanosis or pale color/coolness of the skin
Numbness or tingling (paresthesia)
Decreased or no movement (paralysis)
Increased edema
Home Cast Care
Ice/elevation for pain or swelling in first 24-48 hrs
Wiggle fingers or toes hourly
For itching
NEVER insert anything into the cast
Blow COOL air on hair dryer’s lowest setting
NO lotions or powders
Cover with plastic to protect from wetness
Assess skin integrity
Contact HCP if foul smell or drainage, T > 101.5°F (38.5°C), skin irritation or breakdown, “burning” under cast, if cast gets wet, split, cracked, or softened, or for s/sx of compartment syndrome.
After Cast Care
May be frightened by loudness of cast saw
New skin may be tender—avoid scratching & excessive rubbing
Soak in warm water & wash daily with soap
Apply moisturizing lotion
Encourage gradual increase of ROM
Sprains & Strains
Twisting or turning motion of affected body part
Tendons & ligaments stretch excessively & may tear
Any joint (most common ankle & knee)
RICE (rest, ice, compression, elevation)
Inspect for edema, bruising, inability to bear weight.
Assess neurovascular status.
May need crutches
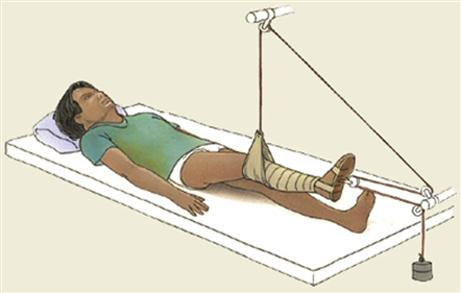
Traction
Application of weights and pulleys to provide pulling force on an extremity or body part for:
reducing dislocations
realigning injured extremities
immobilizing fractures
correcting deformities
Not used as often in practice
Ensure ropes move freely & weights do not touch floor. Constant and even traction should be maintained.
Serial x-rays to monitor progress
Skin Traction (short periods of time)
Noninvasive
Apply weights via ropes to bandage or foam boot
Apply traction over intact skin only
Skeletal Traction (long periods of time)
Invasive/when more pulling force is needed
Apply weights via ropes attached to skeletal pins
Protect exposed ends of pins to avoid injury
Types of Skin Traction
Bryant—used for femur fractures, DDH in child < 3 yrs, or a shortened limb. Supine with buttocks slightly elevated & clear of bed. Assess bandages & skin every shift. Ensure ankles and heels are free from pressure.
Russell—femur fracture, hip or knee injuries/contractures. Ensure heel is free of bed & use foot support to prevent foot drop, assess for skin breakdown from sling
Types of Skeletal Traction
Dunlop—humerus fracture. Provide pin site care, neurovascular checks, wiggle fingers periodically.
90-90—femur fracture reduction when skin traction inadequate, pin in distal femur. Provide pin site care, may need restraints, neurovascular checks.
Crutchfield tongs— management of cervical or thoracic fractures. Assess tongs q. 8 hours, log roll, pin site care, neurovascular checks.
Fixation
Surgical reduction (open reduction) of complicated fracture or skeletal deformity with an internal or external pin(s) or device used to immobilize bone while it heals
Routine neurovascular & skin assessment essential
Pins inserted into bone & place child at risk for infection
External—Pin Site Care daily as prescribed
National Association of Orthopedic Nurses (NAON) published minimal guidelines
Perform pin care weekly or prn after first 48-72 hrs
Chlorhexidine 2 mg/mL is solution of choice.
Teach child and family pin site care & s/s of infection to report
Internal—no additional care
Bryant Russell Dunlop 90-90 Crutchfield




Congenital & Developmental Disorders
Pectus Excavatum/Carinatum
Pectus excavatum—funnel shaped chest, sinks inward at the xiphoid process
Progresses with growth
May require surgery if cardiac or pulmonary compression occurs- SOB, exercise intolerance, chest pain in older children
Pectus carinatum—protuberance of chest wall, pigeon chest
Extent for both can be determined by xray, CT, MRI
Limb Deficiencies
Absence of a limb or portion of it, or the deformity of a limb
Occurs during fetal development
Mostly attributed to amniotic bands
Provide activities EARLY to improve child’s function & activities that the child can participate in
PT/OT- early intervention to meet developmental milestones
May need prosthesis
Polydactyly/Syndactyly
Polydactyly—extra digits
Assess for presence of bone
May require surgery to remove the extra digit or simply tying off with suture (necrosis)
Syndactyly—webbed digits
No treatment necessary
May have surgery (more complex) for cosmetic reasons
Both can be inherited & associated with other genetic disorders
Metatarsus Adductus -curve foot
Medial deviation of forefoot
One of most common foot deformities of childhood
Degree of flexibility is important & determines treatment
If flexible past neutral position, then observe
If flexible only to neutral position, stretching exercises may be beneficial
If rigid, serial casting (before 8 months of age)
Surgery in severe cases (rare)
Congenital Clubfoot
Complex deformity of the ankle and foot in which the hindfoot and forefoot are rotated inward with and arched midfoot while the foot is pointed downward
Rigid and cannot be manipulated into a neutral position
Etiology unknown-
genetic/environmental factors
TX
Goal of treatment is functional foot
Treatment starts as soon after birth as possible
Weekly manipulation with serial casting initially, then q2wk
May require corrective shoes or bracing
Severe may require surgery—foot immobilized with cast for up to 12 wks post-op, then ankle-foot splints or corrective shoes for years
Teach cast care as previously discussed & use of braces or splints as necessary
Osteogenesis Imperfecta (OI)
Inherited connective tissue disorder that results in fragile bone (fractures), small, weak muscles, & joint hypermobility causing instability of joints (lax joints).
Lacks bruising/swelling
“brittle bone disease”
Multiple classifications ranging mild to severe
DX: Collagen biopsy (skin punch), genetic testing to determine severity (50% Type 1-mildest), xray
Handle child carefully!
Common findings
Blue sclera (purple, blue, or gray tint that does not resolve after first few weeks of life.)
Short stature
Early hearing loss
Discolored teeth
Joint hypermobility
Acute & chronic pain
Scoliosis
Respiratory complications(from immobility)
Gross motor developmental delays
OI Treatment
Biphosphonate (increases bone mineral density)
Increased calcium and Vitamin D in their diet
PT/OT
Splints/braces
Surgical insertion of rods into long bones
Exercise- walking, swimming, water therapy
Developmental Dysplasia of the Hip (DDH)
Abnormalities of the hip joint including dislocation and subluxation
Femoral head has abnormal relationship with acetabulum
Unilateral or bilateral
May cause avascular necrosis of femoral head, loss of ROM, recurrent instability, femoral nerve palsy, leg length discrepancy, early osteoarthritis.
Goal is to maintain hip joint in proper place so that femoral head & acetabulum can develop properly
Treatment varies based on age & severity
Diagnosing DDH
Asymmetrical gluteal &/or thigh folds lying prone
Limb-length discrepancy- shortening of affected femur
Trendelenburg gait in older child
Limited hip abduction with passive ROM
Positive Barlow and Ortolani test- palpable “clunk”
Galeazzi sign- discrepancy of knee height when both knees
TX For DDH:
Pavlik Harness for DDH
Up to 6 mo of age may be treated with Pavlik harness—maintains hip flexion & abduction
Must be worn continuously at first & applied properly, then off for short periods (23 of 24 hours/day)
Parents are instructed to not adjust the harness
Assess for skin breakdown (long socks & undershirt recommended to prevent rubbing)
Usually worn for 3 months
Hand wash, air dry
Other options for DDH
For children 6 mo old or those who do not improve with Pavlik harness- traction may be used (Bryant)
Surgical reduction & casting followed by bracing or orthotic use may also be necessary
Spica cast for 12 wk
Abduction brace
Physical Therapy-
Strength and flexibility
Tibia Vara (Blount Disease)
An exaggerated “bowing” of the legs
Etiology unknown
Occurs more frequently in child who walks early
Obesity is risk factor
Bracing & surgery should start before age 4 yrs
Compliance is most significant barrier to successful tx
Brace must be continued for months to years & worn 23 hrs/day
Long-leg bent knee or spica cast after surgery
Torticollis- “twisted neck”
Painless muscular condition in infants or children
Observe for wryneck (tilting head to one side)
Congenital form may be related to in utero positioning
Preferential turning of head to one side when supine or prone can lead to tightness of sternocleidomastoid muscle
TX
Passive stretching exercises and tummy time
PT & a tubular orthosis collar may be used
Pharmacological treatment-
Baclofen (muscle relaxant)
Injection of botulinum toxin (Botox) can provide temporary relief—need to be repeated q3mo
Plagiocephaly
Flat spot on baby’s head/asymmetrical head shape
Management- wearing a helmet for 23 hours a day for 3-6 months, encouraging tummy time
Acquired Disorders
Rickets
Softening or weakening of bones as result of nutritional deficiency from inadequate Ca or vitamin D consumption or limited exposure to sunlight (preventable)
Can also occur if body cannot regulate Ca and Phos (such as in chronic renal dz and malabsorption GI disorders—CF, Chrons, & prematurity)
Look for: dental deformities, bowlegs, bone pain, hx of fractures, low serum Ca, Vitamin D, and Phos levels
Treatment is Ca, Phos, & possibly vitamin D supplements
Slipped Capital Femoral Epiphysis (SCFE)
Femoral head dislocates (slips) through the epiphyseal (growth) plate
Etiology unknown
Promptly refer to orthopedic surgeon
Can result in chondrolysis (cartilage necrosis), avascular necrosis of femoral head, shortening of the affected leg, thigh atrophy, and osteoarthritis.
May present with
(acute or chronic) groin, thigh, or knee pain,
inability to bear weight
a limp or Trendelenburg gait
decreased ROM
affected leg may be shorter
X-ray for diagnosis
Once diagnosed, strict bed rest & activity restriction (No ROM movements)
May need Russell traction before surgery (pins or screws to hold the femoral head in place)
Monitor neurovascular status
Teach crutche walking (PT), weight bearing after 1 week, pin removal later.
Severe cases may need osteotomy
Legg-Calve-Perthes Disease
Self-limiting condition involving avascular necrosis (cutting off blood supply) of femoral head
MRI for diagnosis
Interruption of blood supply to femoral head results in bone death, loss of spherical shape, and swelling of the soft tissues.
New blood vessels develop and revascularization takes 6-12 months
Femoral head reforms over 1-2 years
Legg-Calve-Perthes Disease
Characterized by:
Starts as a painless limp (intermittent over period of months) resulting in…
Mild hip pain or referred knee or hip pain
Pain aggravated by exercise
Trendelenburg gait/joint dysfunction
Limited abduction of hip (ROM)
Muscle spasms
Wasting/atrophy of thigh/buttock muscles
Treatment includes anti-inflammatory medications to decrease muscle spasms around hip joint & relieve pain. May take 18 months to 4 years to fully recover. (no preventative measures)
Activity limitations may be prescribed (crutch teaching)
Bracing, casting, or traction. Serial x-rays.
Surgery is rare—osteotomy may be performed
Osteomyelitis
Bacterial infection of bone & soft tissue surrounding bone (long bones most common)
Staphylococcus aureus is most common infecting organism – bacteria enters the bloodstream and invades the bone. (hematogenously)
X-ray/bone scan to confirm diagnosis. Blood cultures to identify organism. Elevated WBC.
Pain, refusal to walk/guarding, fever, swelling, warmth, tenderness
Bed rest, pain management, antipyretics, 4-6 wk course of antibiotics (IV then po), possible debridement
Septic Arthritis
Bacterial invasion of joint space (most often hip or knee)
Usually obtained hematogenously through direct puncture from injections, venipuncture, wound infection, surgery, or injury
Sepsis of hip joint may cause avascular necrosis of femoral head
Considered MEDICAL EMERGENCY because destruction of joint cartilage may occur within few days
Joint aspiration (responsible organism) or arthrotomy, IV antibiotics, then possibly PO antibiotics at home
Note recent respiratory infection or otitis media, skin or soft tissue infections, traumatic puncture wounds, or femoral venipuncture
S/S: Ill appearance, sudden onset of fever, moderate-severe pain, usually maintains joint in flexion & will not allow leg to be straightened. Will not bear weight.
Pain management with acetaminophen or ibuprofen usually sufficient, but may need morphine or codeine
Crutches, wheelchair, PT
Scoliosis
Lateral curvature of spine that exceeds 10 degrees
Congenital, associated with disorders, or arises spontaneously (idiopathic)
Idiopathic occurs more during adolescence & is the most common type
Children are screened at each healthy visit until bones mature
With progression & changes of the shape of the thoracic cage, cardiac & pulmonary compromise may occur
Treatment based on age, expected future growth, & severity of curvature
Commonly will not report back pain- just mild discomfort
Asymmetry in hips or shoulders is noted by family or during scoliosis screening.
25-40 degree curvature, bracing may be sufficient
Watch closely for skin breakdown
> 45 degrees curvature, surgical approach used
Rod placement, bone grafting, or spinal fusion
Post-op -> ICU
use log-roll technique to turn to avoid flexion of back
Indwelling urinary catheter, incision care, PCA, IV antibiotics, may need blood transfusion
Ambulate slowly when ordered to avoid orthostatic hypotension. Passive ROM exercises.
Home Health/PT/OT- can return to school in 4-6 weeks
Overuse Syndromes
Group of disorders that result form repeated force applied to normal tissue
Develop over weeks to months
No identifiable injury
Pain associated with an activity & worsens with participation in the activity
Initially apply ice when pain is severe.
Anti-inflammatory medications (NSAIDs- ibuprofen) may be helpful
Encourage to limit exercise & participate in different activity
Resolves over few weeks then can resume activity
Osgood-Schlatter disease—partial pulling/tearing of the ossification center of the tibial tubercle
Most commonly affects adolescent boys during period of rapid growth
Often dismissed as “growing pains”
May take 12-24 mo to resolve
Encourage stretching before activities & conditioning before season begins
Resolves on its own once the child’s bones stop growing
Radial Head Subluxation (Nursemaid’s Elbow)
Occurs when pulling motion on the arm causes annular ligament surrounding radial head to stretch or tear, therefore displacing the radial head
Ligament becomes entrapped within the joint
Child will hold arm slightly flexed at side or across abdomen & refuse to move it
Neurovascular status is normal, no edema or bruising, & no obvious discomfort if arm is still
After reduction, child will experience less pain almost immediately (video)