In-Depth Notes on Amnesia and Memory Impairment
Impairments of Memory and Learning: Amnesia
Aims of the Lecture
To describe and discuss the following aspects of amnesia:
Characteristics: definition, causes, brain lesions, behavioral symptoms
Theoretical interpretation and implications for memory theories
Definition of Amnesia
Generalized memory loss affecting the ability to store or retrieve information.This condition can be classified into different types, including anterograde amnesia, where new memories cannot be formed, and retrograde amnesia, which disrupts the retrieval of pre-existing memories.
Types of Amnesia
Retrograde Amnesia:
Characterized by a deficit in retrieval of information acquired prior to the onset.
Typically affects short-term memories spanning from a few hours to days before the trauma.
Anterograde Amnesia:
Involves deficits in encoding, storage, and learning new information post-trauma.
This may resolve after a few days or weeks, or may persist permanently depending on severity.
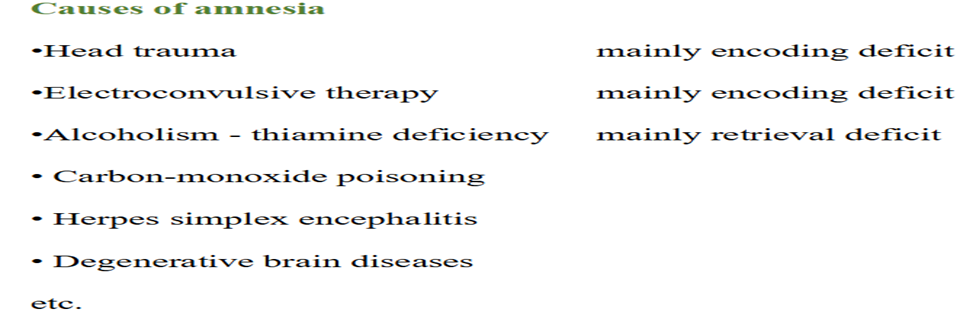
Causes of Amnesia
Generally results from brain injury.
Neuroanatomical Correlates of Amnesia
Diencephalon (Thalamus):
Functions as a relay station for sensory information.
Thalamus sits in brain subcortical structure and is crucial for attention, consciousness, and regulatory functions associated with memory processing.
Disruption can lead to amnesia.
Hippocampus:
A horseshoe-shaped region vital for memory retrieval and navigation.
Plays a significant role in memory consolidation and retrieval. Damage to the hippocampus can result in both anterograde and retrograde amnesia, impacting a person's ability to form new memories and recall past experiences.
Behavioral Symptoms of Amnesia
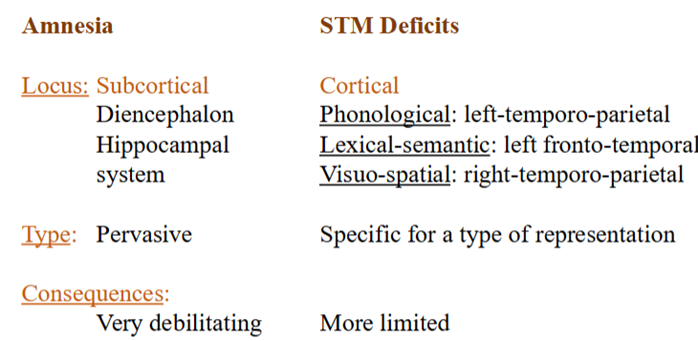
Non-specific representation relative to cortical impairments.
Involves the storage of information unlike short-term memory deficits, which deal with immediate conscious awareness.
Amnesia linked to subcortical lesions, while short-term memory deficits correspond to cortical lesions.
Consequences of short-term memory loss are less extensive compared to subcortical amnesia.
Case Study: Patient H.M.
Surgical removal of medial temporal lobes, including partial hippocampus and amygdala.
Experienced severe anterograde amnesia and some retrograde amnesia for events before surgery.
Normal thought process but difficulty with:
Episodic memory and semantic memory (e.g., could not remember faces, facts, or routes).
Notable preservation of:
Normal digit span.
Learning of new skills (mirror drawing, puzzles).
Is any ltm function spared In amnesia
Skill learning
Patients retain ability to learn motor skills without conscious memory of prior learning.
Example: Mirror drawing, where patients improve performance without recalling practice sessions.
Tower of Hanoi- transfer towers to last peg following rules- trial and error- amnesia patients do this but they wouldn’t know they’ve done it before
Priming involves faster responses to previously presented items, indicating some retained memory.
Theoretical Interpretations of Amnesia
Explicit vs. Implicit Memory:
Explicit Memory: Conscious events and declarative memory (facts based on conscious attention).
Implicit Memory: Unconscious learning, not available for verbal report (skills and procedures).
Evidence shows:
Amnesia primarily affects explicit memory while implicit memory (procedural skills, priming) can remain intact.
Selective impairment for explicit tasks (recall/recognition) but preservation in tasks not requiring explicit memory (fragment completion).
Evidence of Memory Functioning in Amnesia
Amnesics typically poor at explicit recall (memory for events) but can perform well in implicit tasks (e.g., word completion).
Memory for factual information often presents difficulties, especially in more complex contexts.
Declarative vs. Procedural Memory
Declarative Memory includes:
Episodic Memory: Memories of personally experienced events and their temporal relations.
Semantic Memory: Memory for facts devoid of personal context.
Procedural Memory: Skills and habits like riding a bike; often intact in amnesic patients.
Problem with declarative memory and involves storing specific facts which you need to pay specif attention to
Psychogenic Amnesia
Caused by severe psychological trauma, often linked to attempts to escape an overwhelming experience.
Opposite of neurogenic amnesia: patients can form new memories but lack recollection of personal history.
Summary of Understanding Amnesia
Comprehend differences between neurogenic vs. psychogenic amnesia.
Identify causes and neuroanatomical bases of amnesia.
Assess skills and functions impaired or spared in amnesic conditions.
Discuss theoretical frameworks regarding patterns of memory function in amnesic individuals.
What is impaired in amnesia?
Declarative memory with spared procedural memory or Explicit memory with spared implicit memory
We have seen that
• Memory for facts is always impaired when tested explicitly;
• SOME memory for facts is spared when tested implicitly (a form of priming?);
• BUT memory for complex facts and association is always impaired even if
tested implicitly;
• Procedural memory is always spared
A solution?
Amnesics have difficulty with declarative memory which is explicit and can be learned in one go. Complex facts and association among facts can be only be learned explicitly;
Amnesics have no problem with procedural memory and are able to show priming for simple units of information
Episodic vs. Semantic Memory
(e.g., Tulving, 1989)
Two components of declarative memory:
Episodic memory (sometimes called source memory) is: ‛The capacity for acquisition and retention of knowledge about personally experienced events and their temporal relations ... the ability to mentally travel back in time ‛ (Tulving, 1984).
Semantic memory in contrast is memory for de-contextualized facts
Hypothesis: Within declarative memory, amnesia affects episodic memory onlyand leaves semantic memory unaffected. Amnesics can learn facts, but ‛de-contextualized’ facts.
Evidence:
There are patients who suffer a selective loss of autobiographical information. E.g., KC (Tulving et. al., 1988; Tulving, 1989)
- Severe closed-head injury;
- Lesions in the left fronto-parietal and right parietal-occipital regions;
- Did not remember any personally experienced event;
- Typical amnesic pattern, but:
- Preserved general knowledge of history, geography, politics, music, etc.
Problems:
- KC shows some preserved autobiographical knowledge. Tulving claims it is acquired ‛semantic autobiographical knowledge’.
How do we distinguish true autobiographical knowledge from acquired autobiographical knowledge ?
- There are patients who show a selective impairment of episodic memory, but who are not amnesics (Janowsky, Shimamura & Squire, 1987).
More likely interpretation:
- Source or episodic memory is a subset of declarative memory mediated by the frontal lobes.
- An impairment of episodic memory may or may not occur together
with generalized amnesia depending on locus of damage. An episodic
impairment, therefore, does not account for the rest of the amnesic
pattern.
Agatha likely suffered from psychogenic amnesia
Psychogenic amnesia is not an invention but a real syndrome:
• Caused by psychological trauma but may be trigged by a brain damage;
• Common in soldiers during war;
• Caused by severe psychological distress
You want to block out your whole past; so you forget everything that concerns you, but especially your identity.
Cases in the movies where the hero/heroine is trying to reconstruct their past resemble more cases of psychogenic amnesia than neurogenic amnesia:
They do not suffer from anterograde
amnesia: can remember new information, but cannot remember any retrograde information. The opposite of what happens in neurogenic