Prostate Cancer
LEARNING OBJECTIVES
Describe the structure and functions of the prostate gland
Define the risk factors for prostate cancer.
Identify the clinical picture, staging, diagnosis and treatment of prostate cancer.
Describe the value of PSA as a screening test for prostate cancer
Prostate Anatomy
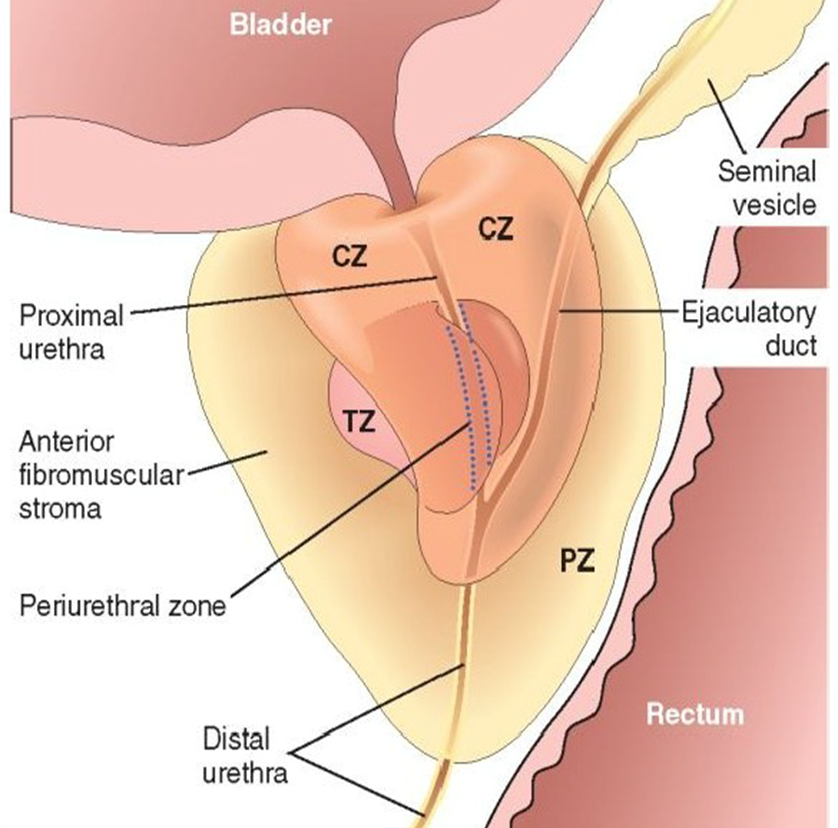
Retroperitoneal organ, encircling the neck of the bladder and urethra.
20g
Devoid of distinct capsule.
4 distinct zones
Central zone (CZ)
Peripheral zone (PZ) - most tumors here
Transitional zone (TZ) - most hyperplasia here
Periurethral zone.
Prostate Histology
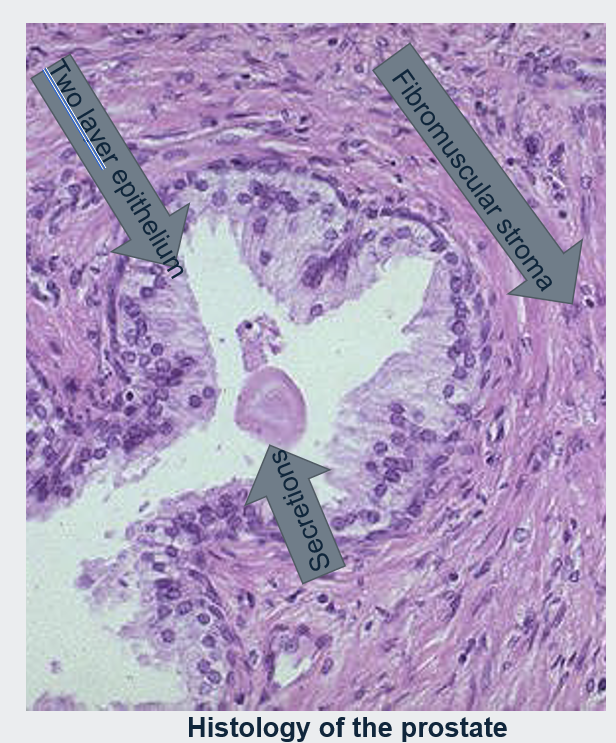
Histologically the prostate is composed of glands lined by two layers of cells.
A basal layer of low cuboidal epithelium covered by a layer of columnar secretory cells.
In many areas there are small papillary infoldings of the epithelium.
These glands are separated by abundant fibromuscular stroma.
Testicular androgens control the growth and survival of prostatic cells.
Prostate Functions
Accessory sex gland.
Function → Secrete prostate fluid
Contents: PSA, prostaglandins, fructose, Zinc, Citrate.
Muscles of the prostate gland also help propel seminal fluid into the urethra during ejaculation.
PSA → Liquefying semen that has thickened after ejaculation. This thinning action allows sperm to swim more freely.
Prostate Cancer
Age: men over 50
Ethnicity: African Caribbean men
Family History (1st degree relative)
High dietary fat and obesity
Vitamin D or E deficiency.
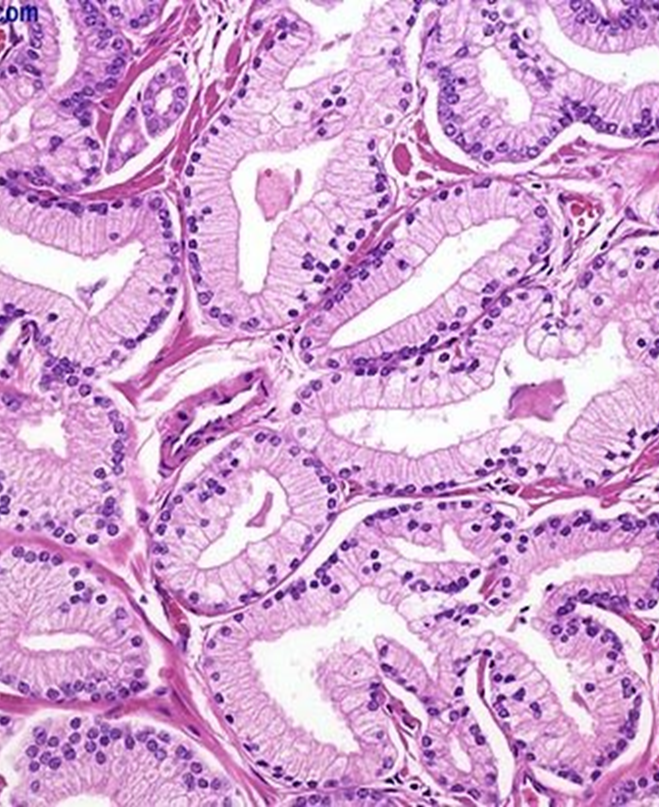
Pathology
Most common form is adenocarcinoma (glandular prostate cancer).
Lined by a single uniform layer of cuboidal or low columnar epithelium.
The outer basal cell layer typical of benign glands is absent.
Cancer glands are more crowded and characteristically lack branching and papillary infoldings.
Prostate Cancer: Presentation
EARLY STAGE USUALLY ASYMPTOMATIC
Most cases detected by serum PSA screening.
Palpable nodule or firmness on DRA (digital rectal examination).
ADVANCED STAGES
Urinary retention/renal failure.
Bone pain
Anemia
Weight loss, fatigue.
Spinal cord compression.
Diagnosis of prostate cancer
PSA → prostate specific antigen
DRA → Digital rectal exam
Asymmetrical, hard and nodular enlargement with loss of median sulcus.
Transrectal ultrasound alone/CT scan/MRI not sensitive enough to make the diagnosis.
Prostate cancer treatment considerations
Patients age
Co-morbid health conditions
Tumor grade
Often a patient choice
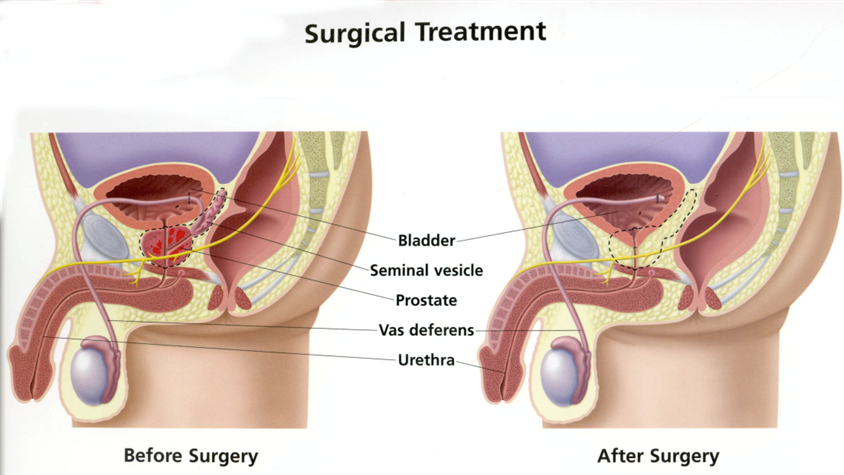
Early stage cancer
Prostatectomy
Radiotherapy
Radioactive Seeds (brachytherapy)
Advanced Prostate Cancer
Androgen deprivation
Antiandrogens
Supportive therapies
Analgesics
Steroids
Vitamin D/Calcium
Chemotherapy
Brachytherapy
Tiny radioactive seeds are put into the prostate.
Each seed is the size and shape of a grain of rice.
Seeds stay in the prostate forever and give a steady dose of radiation over a few months.
Radiation damages prostate cells and stops them multiplying and growing.
Cancer cells cannot recover and die.
Healthy cells can repair themselves easily.
Prostate Screening
PSA as a test
4.0ng/ml is upper limit of normal
More than 10ng/ml → likely cance
4 - 10ng/ml → gray area.
Low specificity (false +ve) and sensitivity (false -ve)
Limited value for screening - need DRE, transrectal sonography, needle biopsy.
Useful to monitor disease - after treatment increasing levels indicate recurrence/metastasis.
What can increase PSA levels?
Prostate Cancer
BPH - benign prostatic hyperplasia
Age - PSA goes up with age.
Prostatitis - infection of the prostate gland
Ejaculation
PSA increased for a short time
Men are asked to abstain from ejaculation for 2 days before testing.