Week 2 - Anaerobic Exercise
What builds up in muscle?
ammonia
PCr
Lactic acid
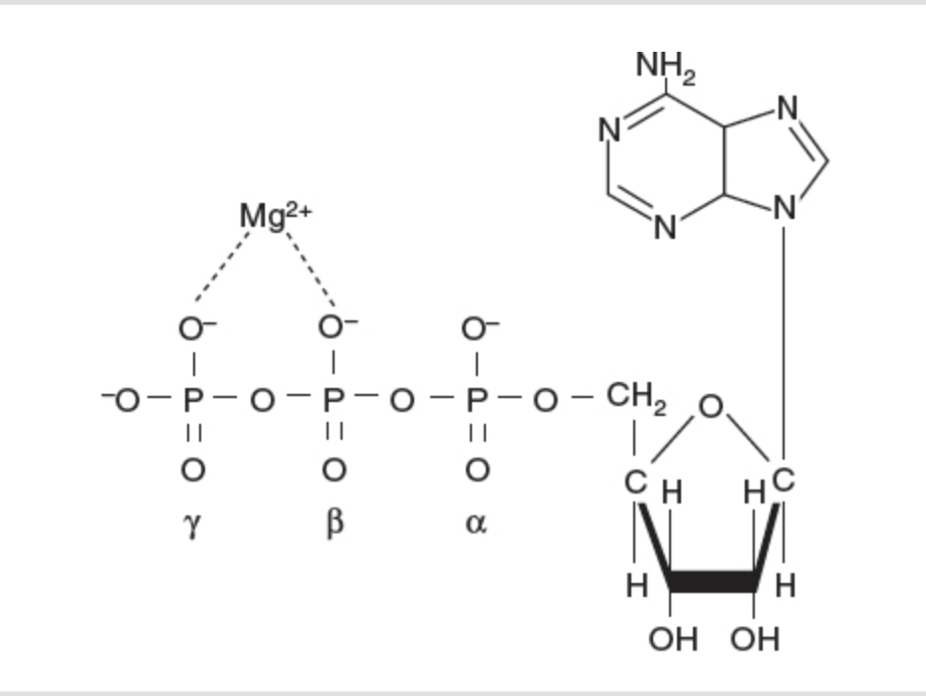
ATP: unstable due to crowded negative charges = phosphoanhydride bonds
nucleotide
adenine + ribose + three phosphate groups
universal energy currency
biosynthesis
transport
movement
ATP is unstable due to negative charges, alpha, beta and gama (1st, 2nd, and 3rd of the triphosphate) the breakdown of those bonds release energy.
essentially = sugar, base and 2 phosphates w an extra part
in cells ATPs functional form is energy ATP 2, has a binding to magnesium, its function is inherently linked to it.
Chemcially accurate drawing of ATP
Cleaving off the phosphate, hydrolysis via ATPase separates a phosphate to release energy; a triphosphate turns into a diphosphate by cleaving off that one inorganic phosphate
lysis = breaking down
hydro = water
hydrolysis = breaking a bond by adding water
ADP +Pi is more stable that ATP, change in free energy is less that 0 meaning the reaction is downhill, driving something forward. This can then be used in another step
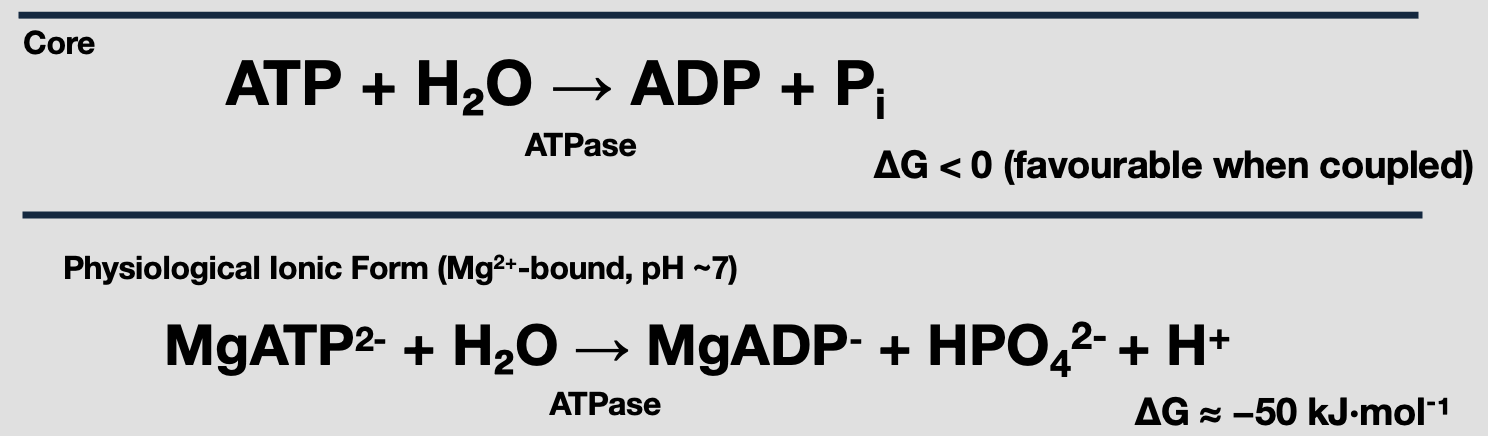
Hydrolysis of ATP, releasing energy and changing the free energy.
extra step = adds in magnesium and ionic charges *nor required to know
ATP synthesis:
phosphagen system = anaerobic
anaerobic glycolysis = anaerobic
aerobic glycolysis
Anaerobic - without air
Required for everyday life - Anaerobic energy production
Involves the breakdown of:
glucose /glycogen
PCr
Rapid ATP w/out oxygen
where do PCr and glycogen get broken down?
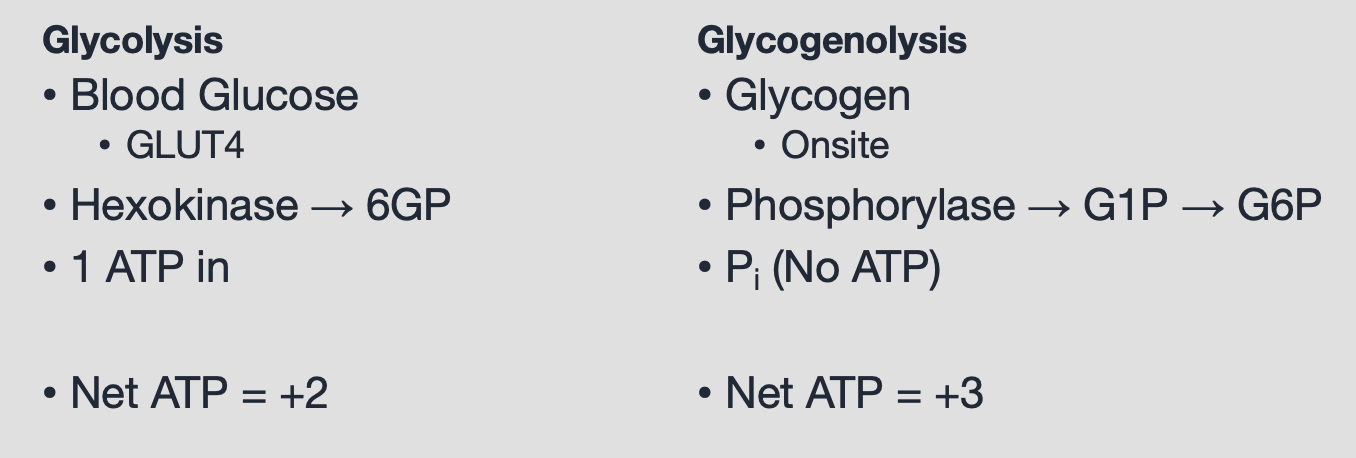
glycolysis = purpose of glycolysis is to phosphorylate ADP, to add a phosphate to ADP
glycolysis w/ glucose
glycogenolysis w/ glycogen
key points in the chain:
glycolysis is when you start w glucose, not glycogen.
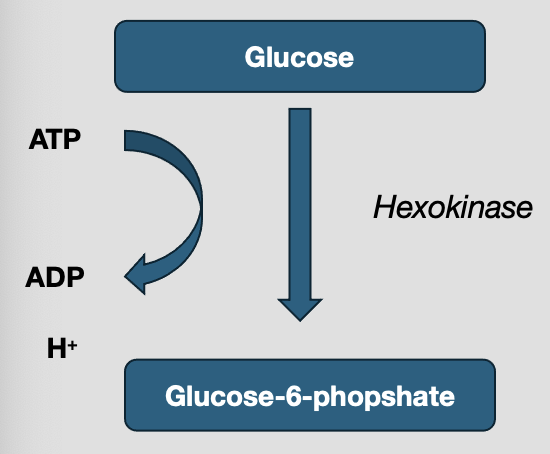
Glycolysis Step 1:
Phosphorylate glucose at C-6 (add a phosphate)
energy investment of 1 ATP
traps guel
G6P cant leave via glucose transporters (glut)
hexokinase inhibited by G6P—> hexokinase turns glucose into glucose-6-phosphate. The glucose comes from the blood, self regulatory step is put in place to not use all of our blood glucose
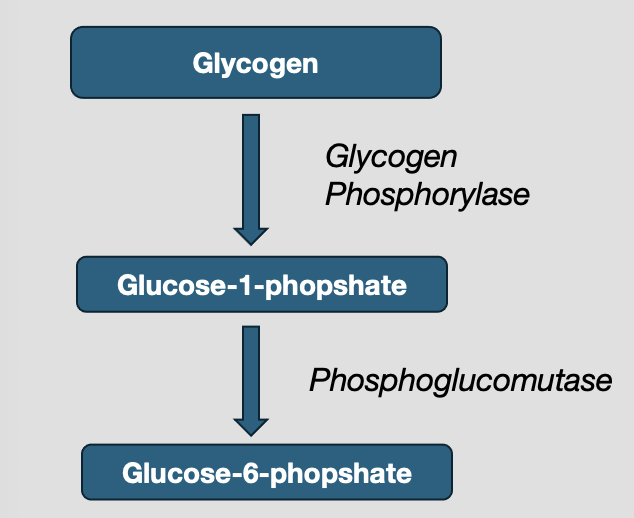
if glycogen is considered, extra steps must take place
glycogen phosphorylase (enzyme) releases G1P
phosphoglucomutase —> G6P
energy investment = 0 ATP —> uses inorganic phosphate instead of using ATP, blood glucose will cost 1 energy investment this doesn’t
Step 3 of glycolysis:
rate limiting step, once this occurs it must follow through
phosphorylate F-P at C-1
energy investment of 1 ATP
committed, rate-limiting step
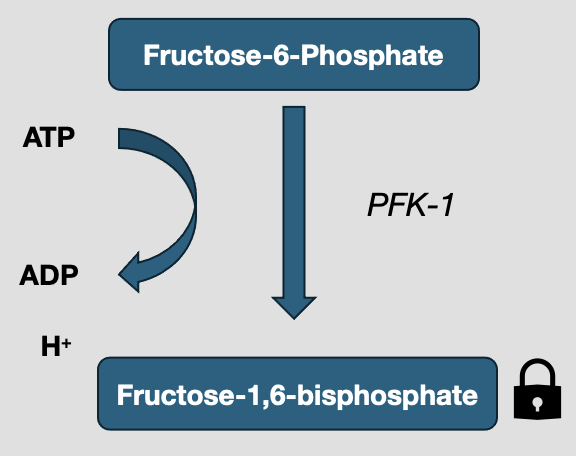
PFK activates
AMP/ADP, F-2, 6-BP, when there is low energy
PFK inhibited
ATP, Citrate, H+, when there is high energy or too much ATP
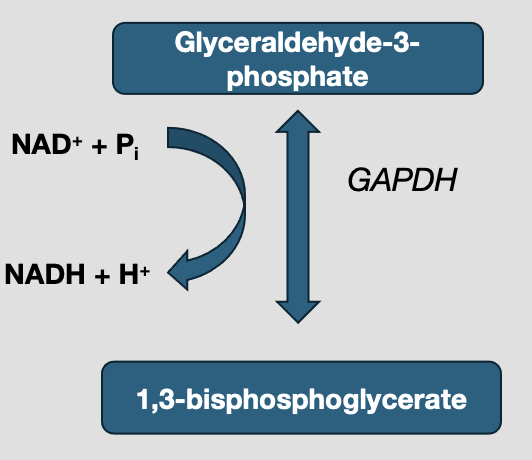
Step 6 of glycolysis: hydrogen is what changes the pH of a muscle
only oxidation step in glycolysis
there is a loss of electrons
glyceraldehyde - 3 - phosphate dehydrogenase
ADds pi without ATP
flux depends on cytocolic
LDH regenerates NAD+ when O2 limited
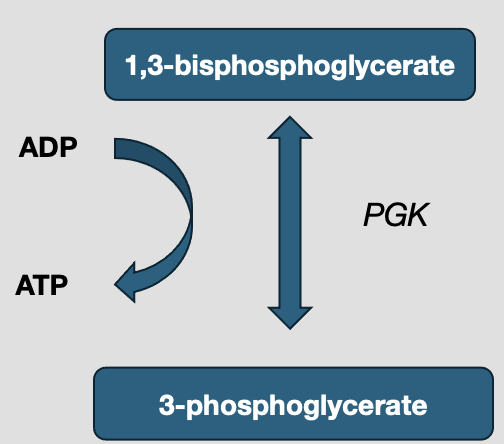
Step 7:
substrate level phosphorylation
+2 ATP per glucose
reversible and depends on step 6
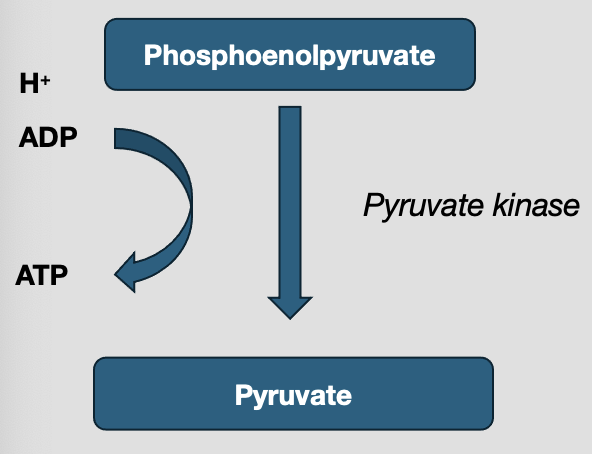
Step 10:
subtrate level phosphorylation
+2 ATP per glucose
irrevesible
Activated by F-1, 6BP
requires Mg2+ and K+
pyruvate in anaerobic conditions will be converted into lactate
Phosphocreatine
fastest ATP buffer, rapid synthesis ATP via creatine kinase
cytosol
finite capacity
if there is more ADP, thats going to drive the reaction
PCr pool —> can be improved, for example when taking creatine as a supplement
each kg is storing 5mmol of ATP and 15 mmol of PCr
studies show that inhibited creatine kinase is essential to facilitate muscle contraction and the use of PCr. Long term adaptations when blocking phosphagen system (ATP-PCr); make anaerobic pathways more efficient, make more mitochondria to increase aerobic respiration.
how we are studying anaerobic metabolism:
percutaneous needle biopsy: it shows you the change in muscle, great for measuring pre and post cycling for example, fiber type and activation, phosphorylation and muscle adaptation. quite invasive and does not show full transition
magnetic resonance spectroscopy: measures rest, exercise and recovery as well as measuring PCr, ATP and Pi. Allows us to watch change over time.
square brackets means concentration of
ramp test; gets harder over time, as it increases, PCr concentration decreases slowly, PCr does not go to 0 at the end of exercise, never going to reach 0 due to systems being in a state of flux
step test: PCr is maintained
oxygen uptake and use mirrors the pathway
Importance of ATP - Pcr
fastest ATP buffer —> supports the first seconds of high intesntiy work
stabalises ADP and preserves change in free energy, helps maintain force
buys time until glycolysis and xoidative phosphorylation reach steady flux
direction set by ADP.ATP concentration, pH, Mg and Pi
recovery is aerobic; PCr resynthesis rate reflects mitochondiral capacity; training shortens
creatine can improve availability of PCr/Cr pool
Summary:
Phosphocreatine (PCr) System – Key Points
Role:
Acts as the fastest ATP buffer in muscle.
Provides immediate ATP resynthesis during the first seconds of high-intensity work.
Stabilizes ADP concentration and maintains free energy for contraction.
Reaction:
Creatine kinase catalyzes:
PCr + ADP ⇌ ATP + CrDirection depends on [ADP]/[ATP], pH, Mg²⁺, and Pi levels.
Capacity & Adaptation:
Small storage pool: ~5 mmol ATP and ~15 mmol PCr per kg of muscle.
PCr supply is finite but can be improved by creatine supplementation, which increases the PCr/Cr pool.
PCr does not fully deplete during exercise; system stays in flux.
Function in Exercise:
Buys time until glycolysis and oxidative phosphorylation reach steady state.
Supports force output at the start of intense efforts.
Recovery of PCr is aerobic → rate of resynthesis reflects mitochondrial capacity. Training enhances this recovery rate.
Research Tools:
Muscle biopsy: invasive, provides detailed biochemical info.
Magnetic resonance spectroscopy (MRS): non-invasive, measures ATP, PCr, Pi in real time during exercise/recovery.
Ramp tests vs. step tests: PCr falls progressively during ramp tests; remains steady in step tests at submaximal levels.
✅ Main Takeaway:
The PCr system is the body’s rapid-response ATP supplier, crucial for short bursts of high-intensity effort. It doesn’t last long but stabilizes energy balance and bridges the gap until slower pathways (glycolysis, oxidative phosphorylation) can contribute. Its recovery depends on aerobic metabolism, and both training and creatine supplementation can expand or speed up PCr availability.