Histo - Female reproductive system
 Functions:
Functions:
Production of female gametes; ova, by oogenesis.
Hormone production.
Reception of male gametes; spermatozoa.
Provision of suitable environment for the fertilization.
Provision of an environment for development of fetus.
Expulsion of developed fetus to external environment.
Nutrition of newborn.
Oogenesis:
The development of ova. The ova are released by the process of ovulation in a cyclic manner. Which suspended during pregnancy.
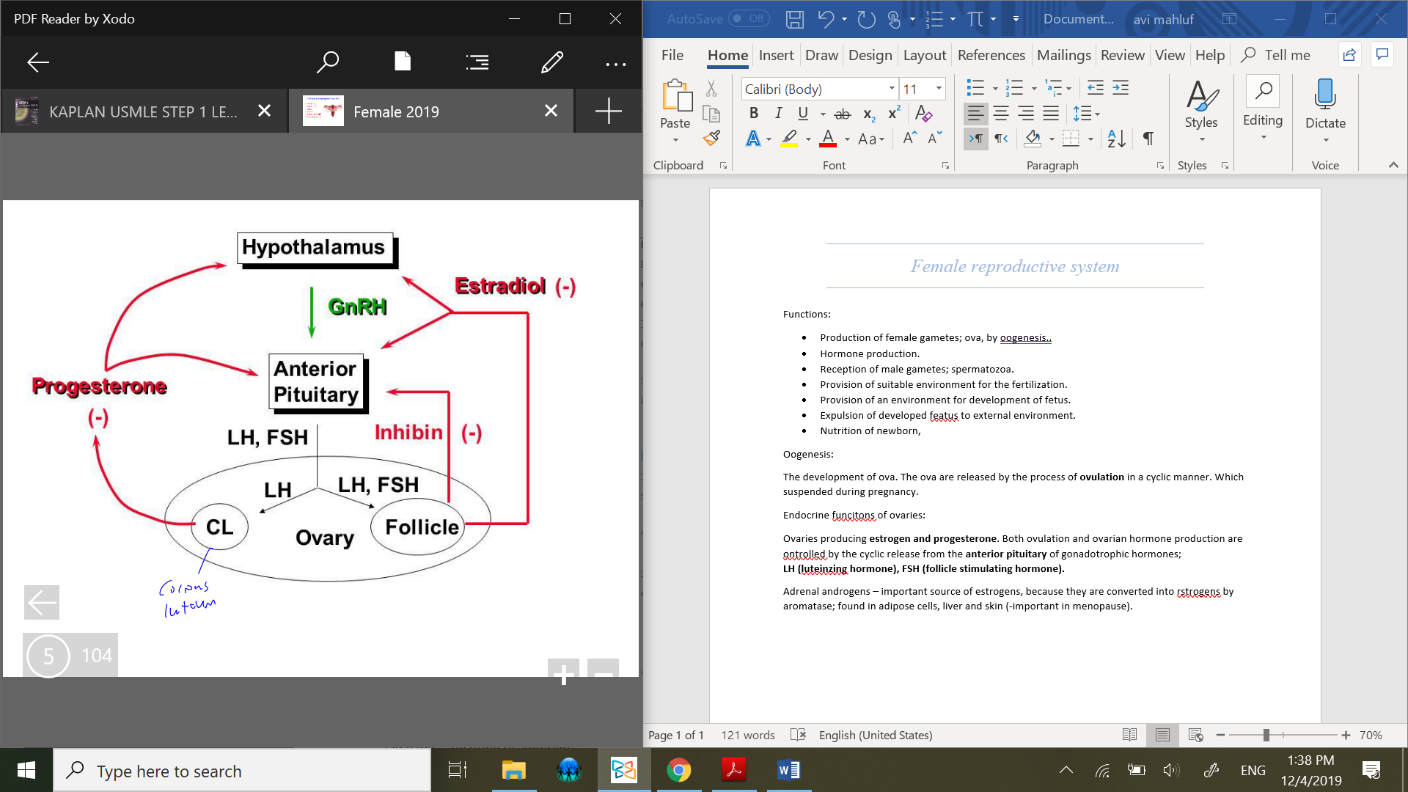
Endocrine functions of ovaries:
Ovaries producing estrogen and progesterone. Both ovulation and ovarian hormone production are controlled by the cyclic release from the anterior pituitary of gonadotrophic hormones;
LH (luteinizing hormone), FSH (follicle stimulating hormone).
Adrenal androgens – important source of estrogens, because they are converted into estrogens by aromatase; found in adipose cells, liver and skin (-important in menopause).
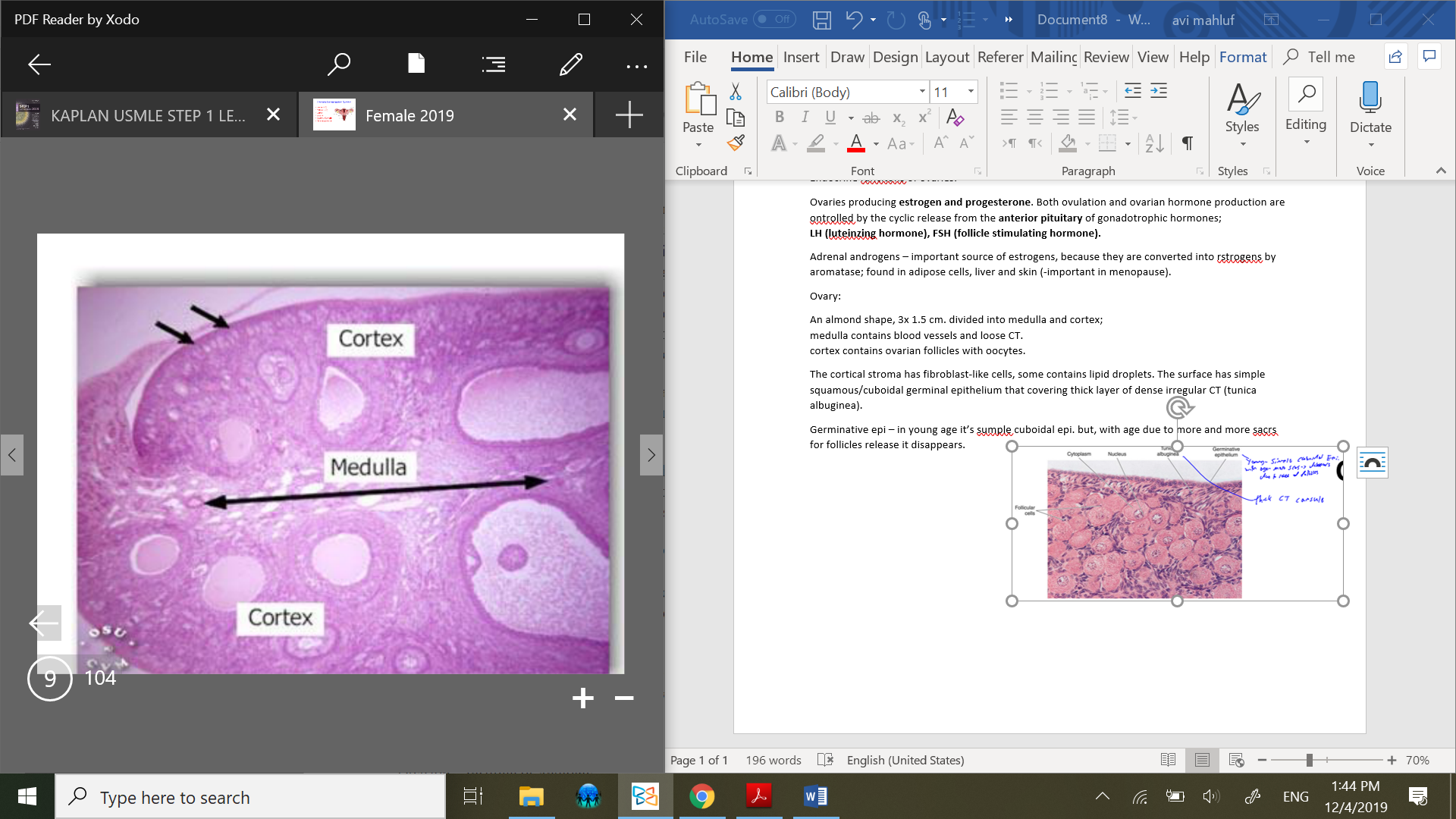
Ovary:
An almond shape, 3x 1.5 cm. divided into medulla and cortex;
medulla contains blood vessels and loose CT.
cortex contains ovarian follicles with oocytes.
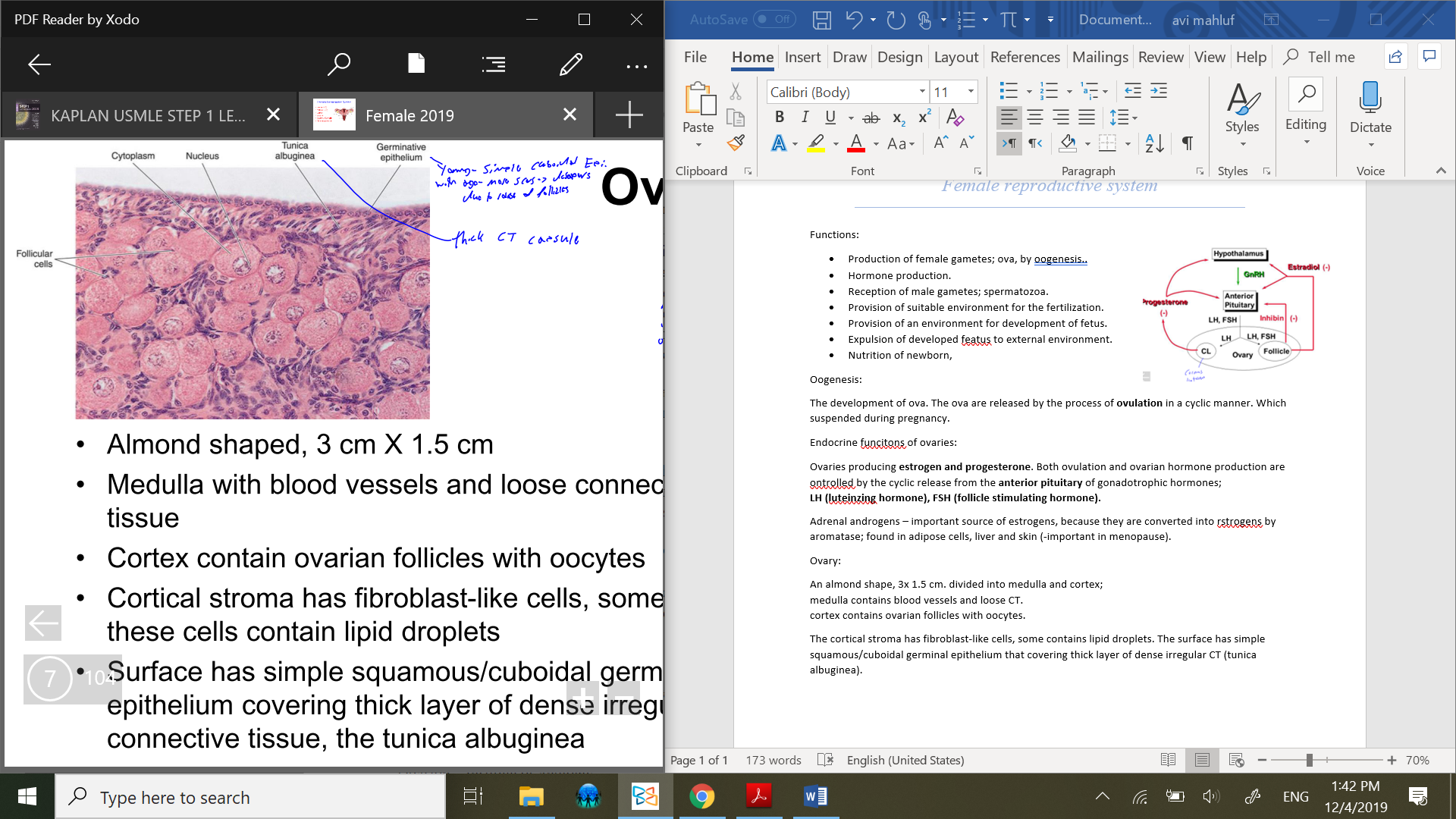
The cortical stroma has fibroblast-like cells, some contains lipid droplets. The surface has simple squamous/cuboidal germinal epithelium that covering thick layer of dense irregular CT (tunica albuginea).
Germinative epi – in young age it’s simple cuboidal epi. but, with age due to more and more scars due to follicles release, it disappears.
 Ovarian follicels:
Ovarian follicels:
Found in cortex of ovary. Between stromal cells, there are located oocytes that surrounded by one or more layers of follicular cells.
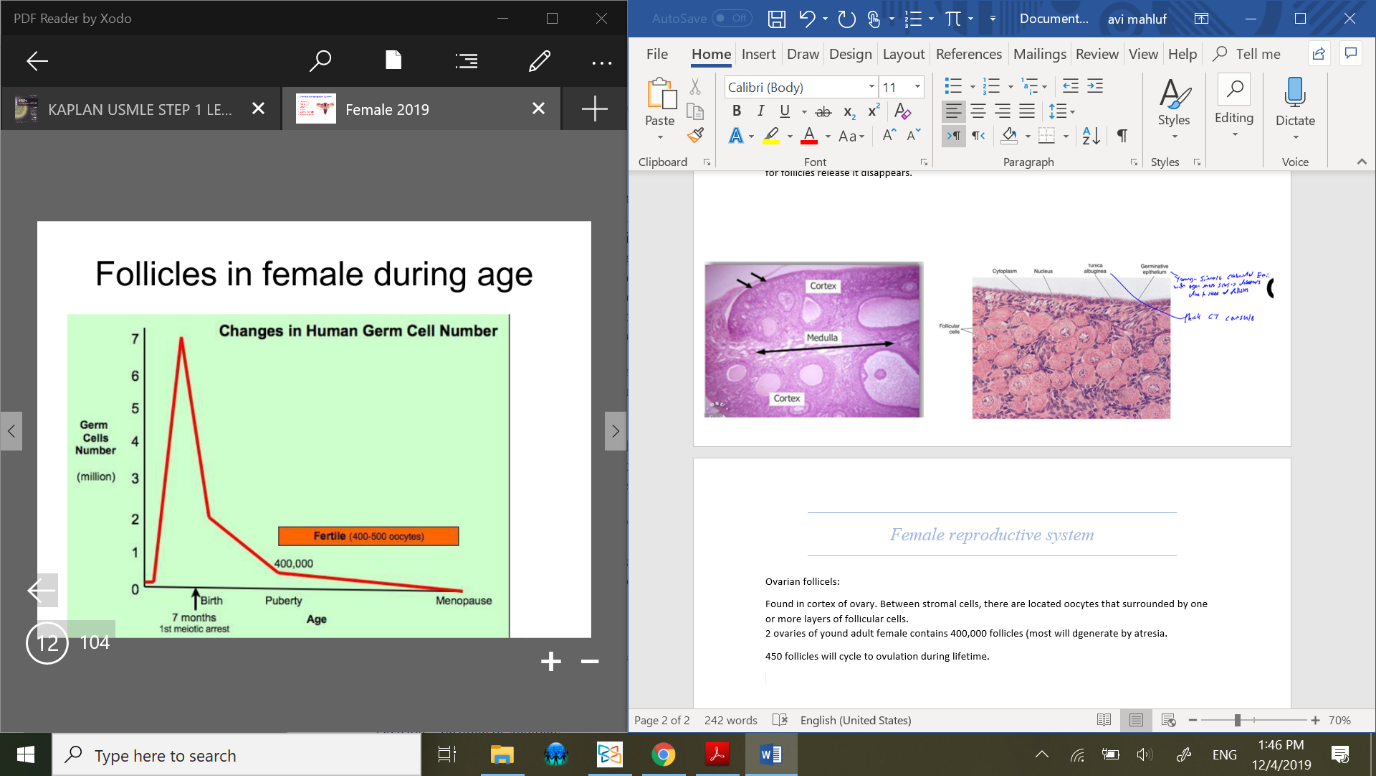
2 ovaries of young adult female contains 400,000 follicles (most will dgenerate by atresia).
the biggest num of follicles is at birth (7 million). 450 follicles will cycle to ovulation during lifetime.
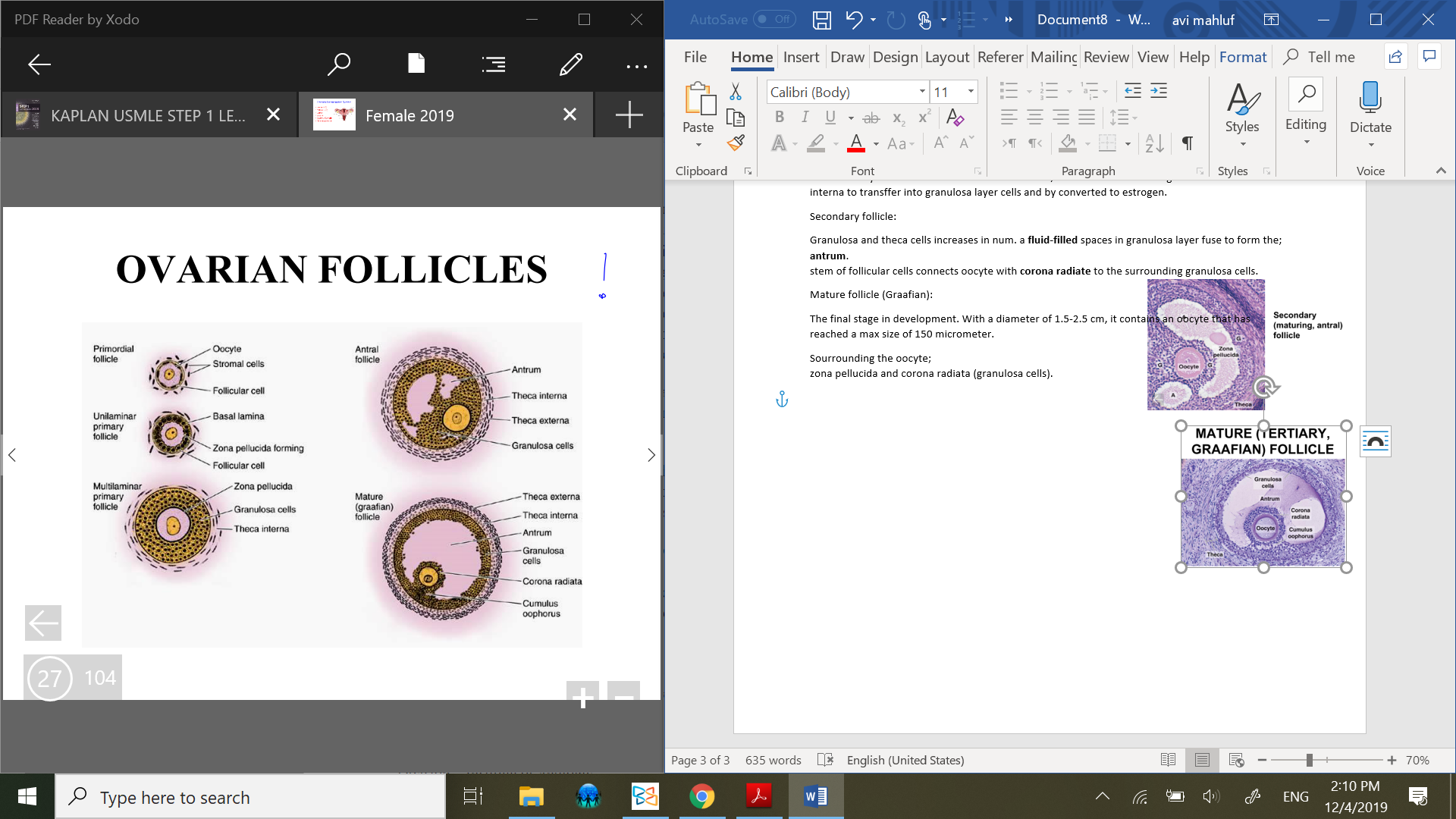
Types of ovarian follicles:
Primordial follicle:
Primary oocyte with one layer of flattened follicular cells. The oocyte in primordial follicle is in arrested beginning of 1st meiotic division, diplotene stage (1st meiotic division is completed just before ovulation).
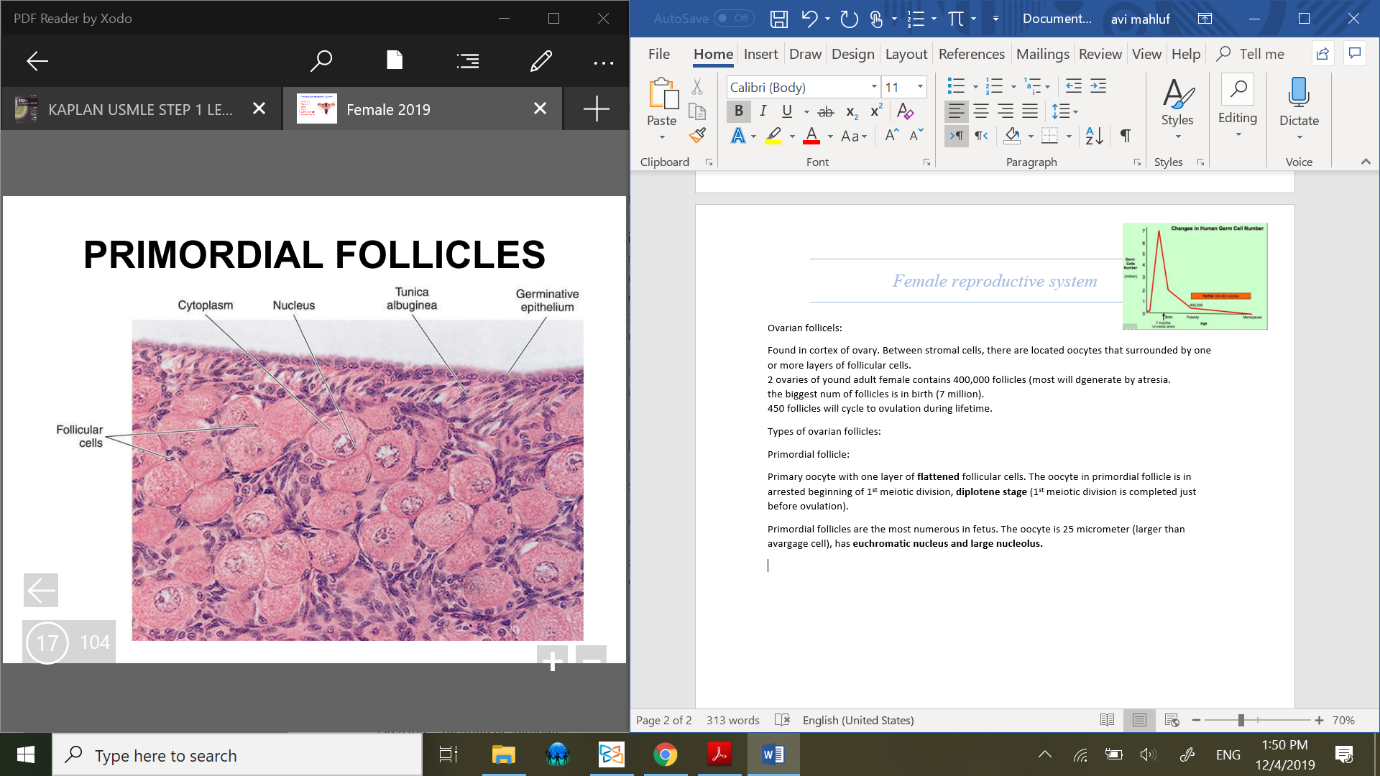 Primordial follicles are the most numerous in fetus. The oocyte is 25 micrometer (larger than avargage cell), has euchromatic nucleus and large nucleolus. With basment membrane.
Primordial follicles are the most numerous in fetus. The oocyte is 25 micrometer (larger than avargage cell), has euchromatic nucleus and large nucleolus. With basment membrane.
Growing follicles:
By FSH at the beginning of every ovarian cycle, 5-15 primordial follicles begin
to grow and only one reaches maturation.
Oocyte diameter increases to 150 micrometers, nucleus enlarges, organelles
increase in num.
Forming;
Unilaminar primary follicle – has one layer of cuboidal follicular cells (primary follicle).
Multilaminar primary follicle – has several layers of follicular (granulosa) cells.
Layers surrounded follicle:
Wall – granulosa cells, theca interna, theca externa.
Zona pellucida – proteoglycans and glycoproteins, forms outside the oocyte membrane, thick basal lamina.
Granulosa layer – Follicular cells differntiate into granulosa cells.
Theca interna – stromal cells forming the inner layer of theca foliculi surrounding the developing follicle.
it’s vascularized and responded to LH, also theca internal synthesizing and secreting androgens, which processes into estrogen in granulosa cells.Theca externa – stromal cells forming the outer layer of theca foliculi which surrounding developing follicle.
consisting of CT, smooth muscle and collagen fibers.
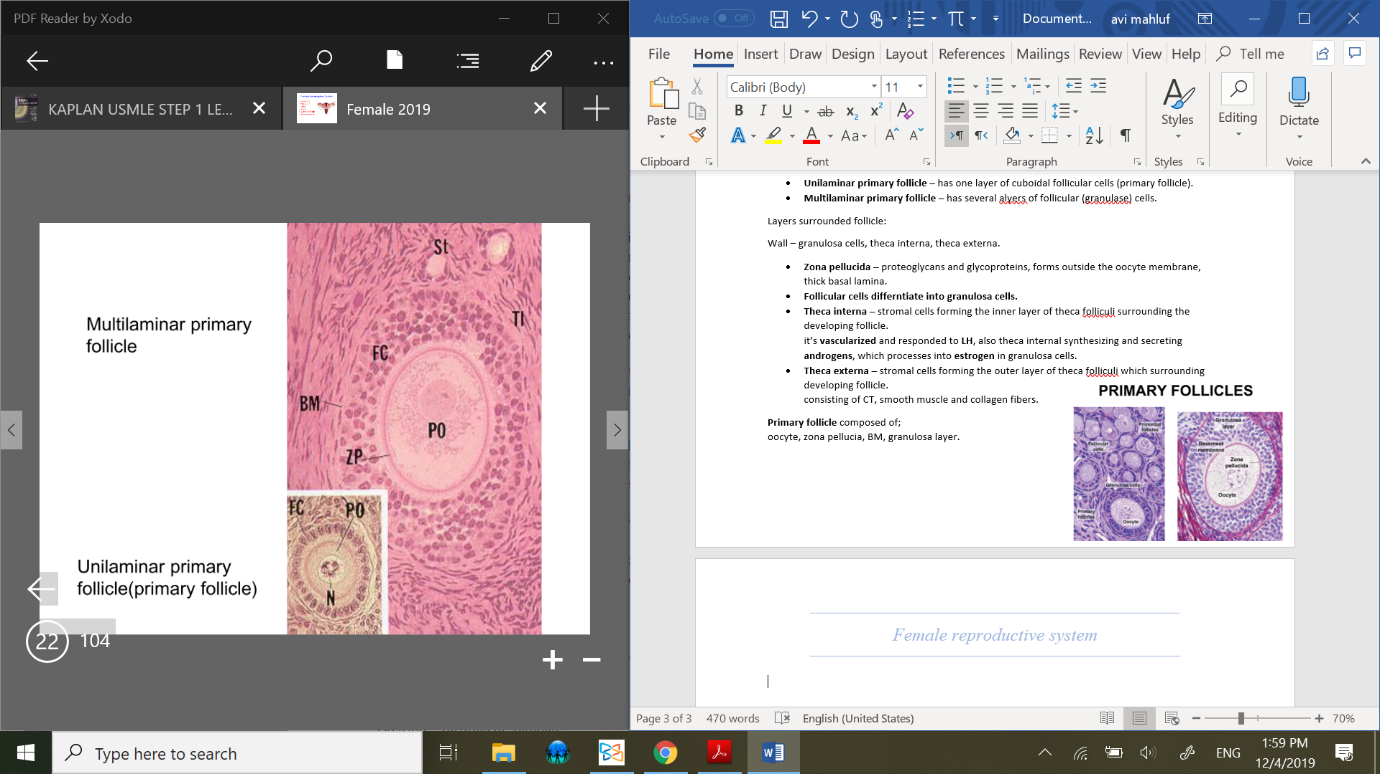
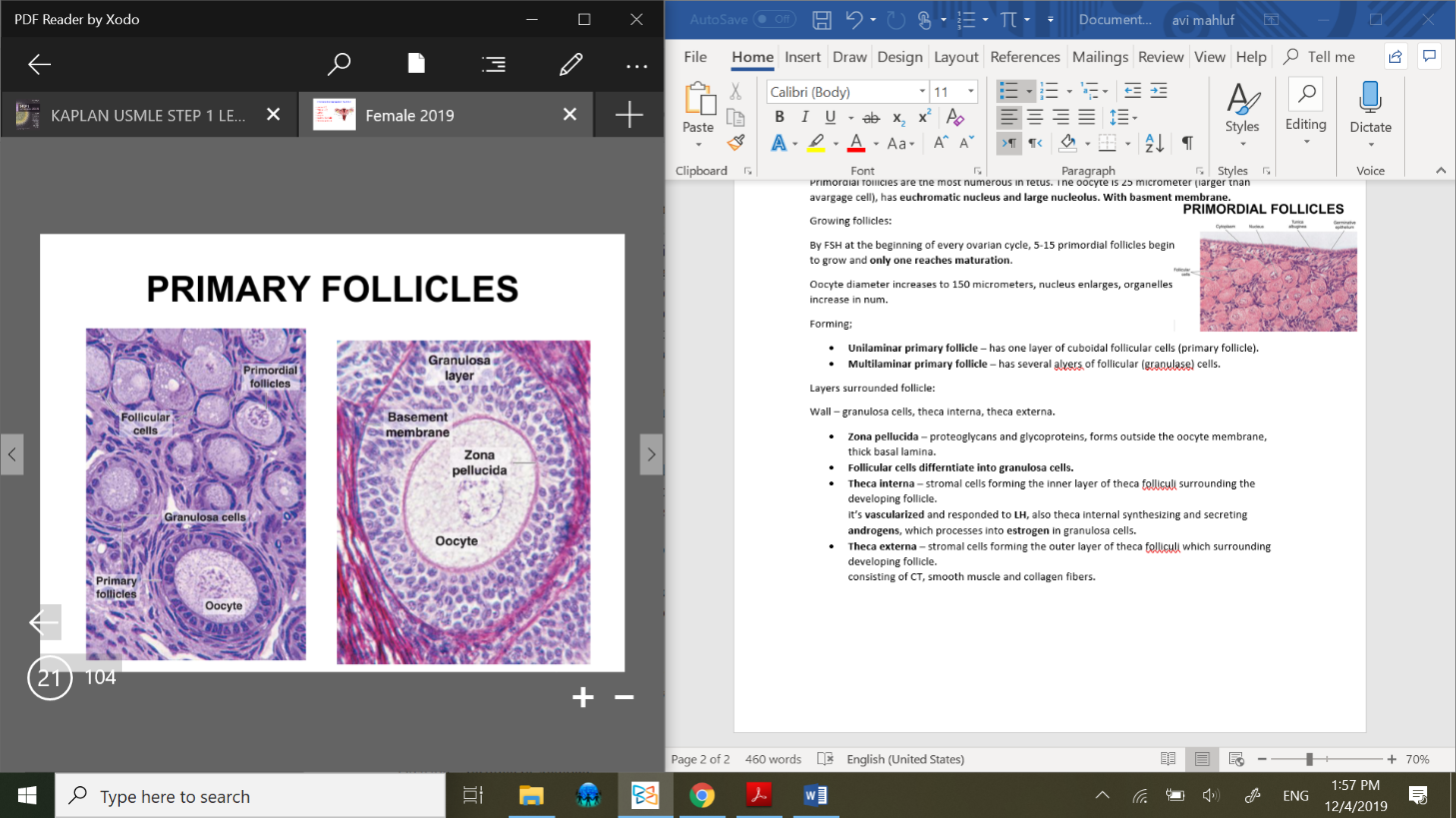
Primary follicle composed of;
oocyte, zona pellucia, BM, granulosa layer.
Theca interna:
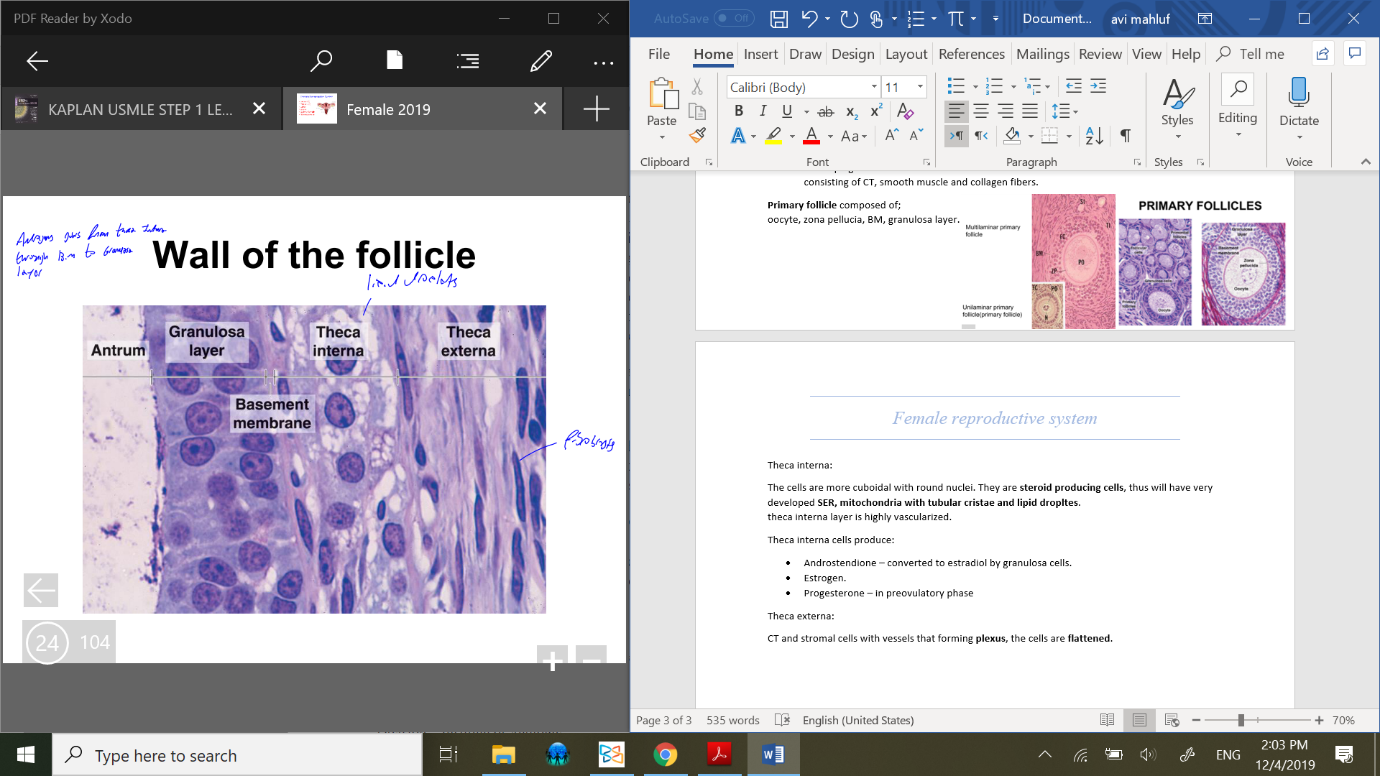 The cells are more cuboidal with round nuclei. They are steroid producing cells, thus will have very developed SER, mitochondria with tubular cristae and lipid dropltes.
The cells are more cuboidal with round nuclei. They are steroid producing cells, thus will have very developed SER, mitochondria with tubular cristae and lipid dropltes.
theca interna layer is highly vascularized.
Theca interna cells produce:
Androstendione – converted to estradiol by granulosa cells.
Estrogen.
Progesterone – in preovulatory phase
Theca externa:
CT and stromal cells with vessels that forming plexus, the cells are flattened.
Granulosa layer and theca interna have sahred BM, which allows the androgens secreted from theca interna to transffer into granulosa layer cells and to be converted to estrogen.
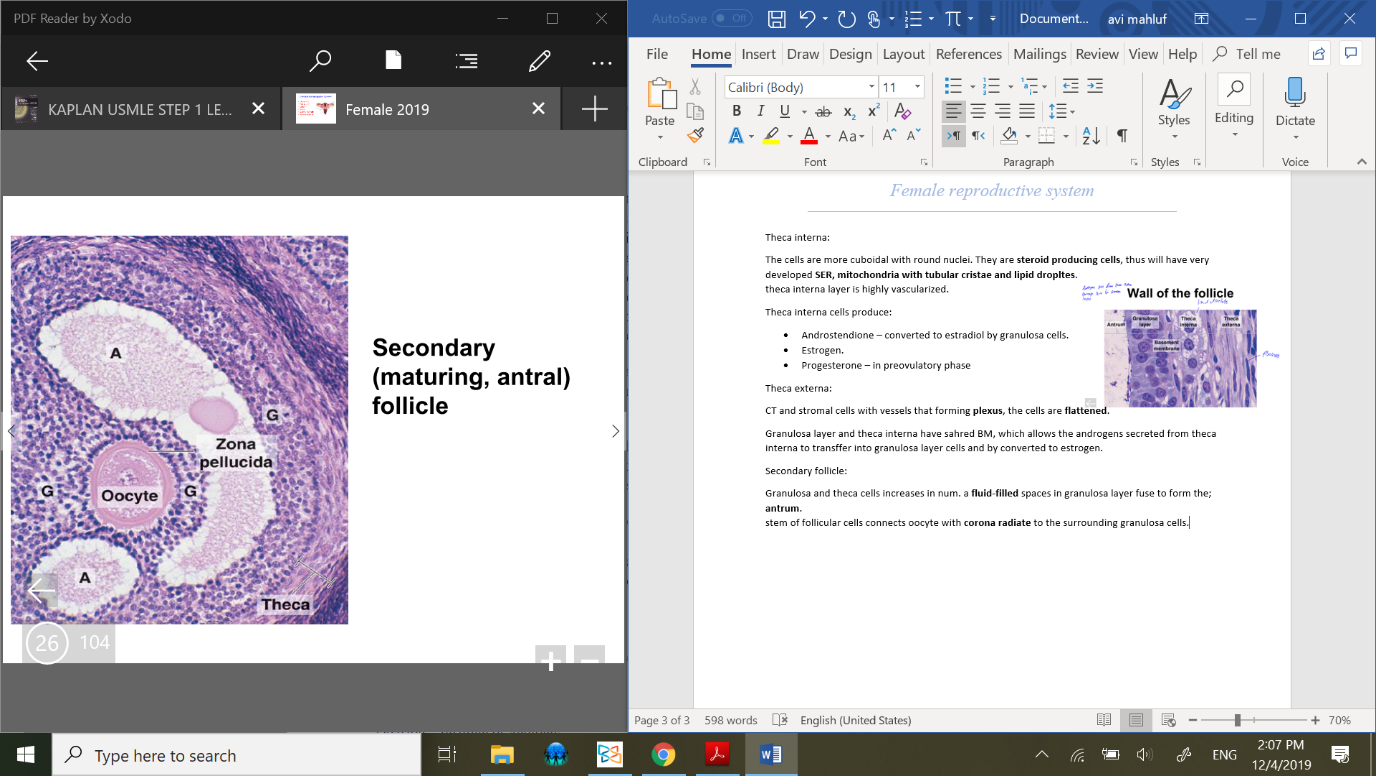
Secondary follicle:
Granulosa and theca cells increases in num. a fluid-filled spaces in granulosa layer fuse to form the;
antrum.
stem of follicular cells connects oocyte with corona radiate to the surrounding granulosa cells.
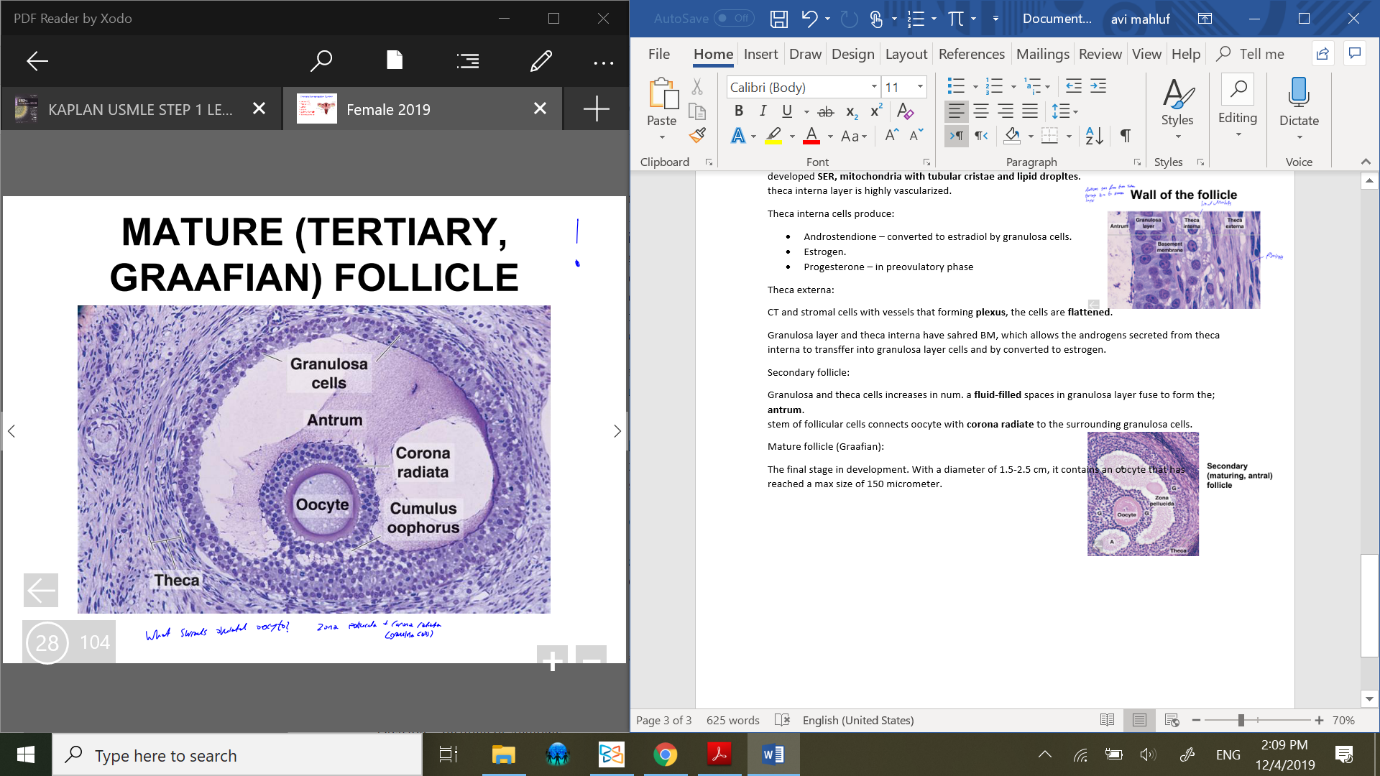
Mature follicle (Graafian):
The final stage in development. With a diameter of 1.5-2.5 cm, it contains an oocyte that has reached a max size of 150 micrometer.
Surrounding the oocyte;
zona pellucida and corona radiata (granulosa cells).
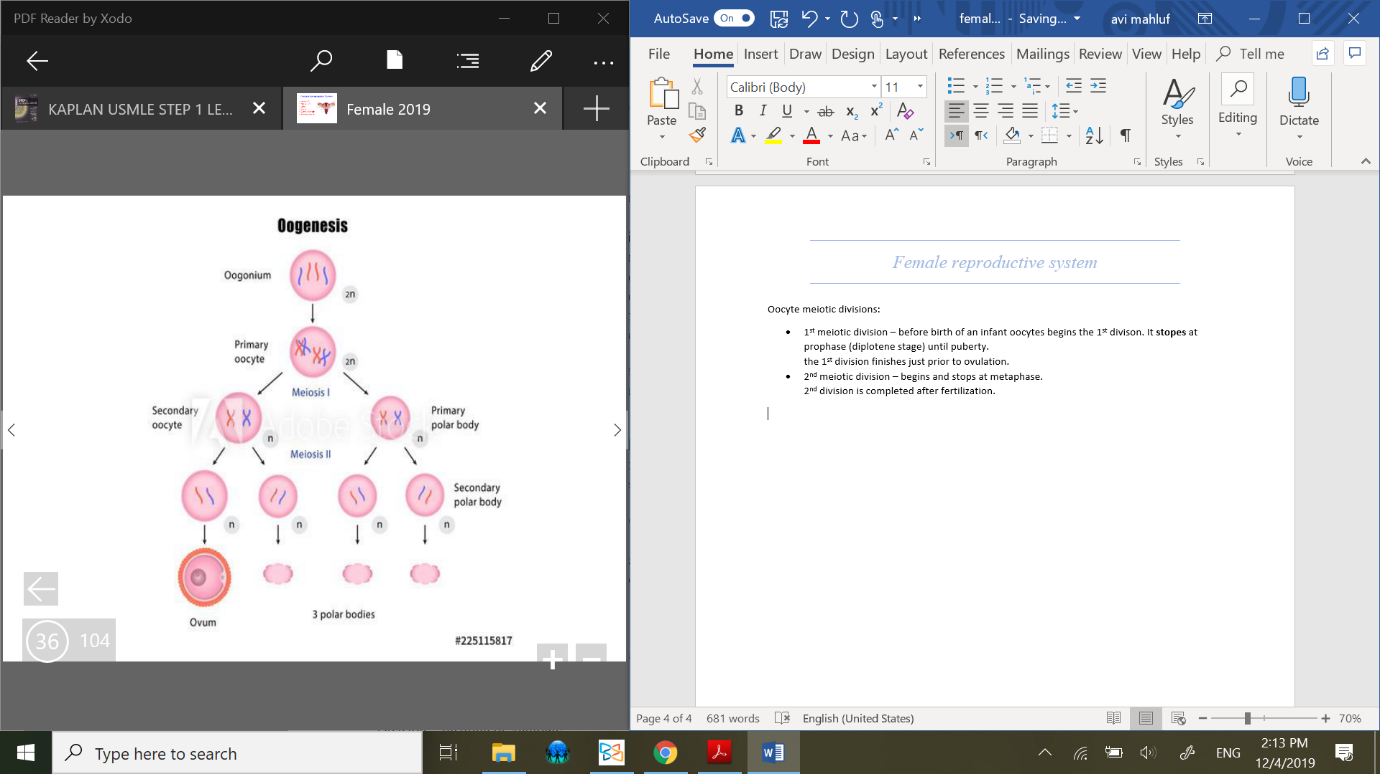 Oocyte meiotic divisions:
Oocyte meiotic divisions:
1st meiotic division – before birth of an infant oocytes begins the 1st divison.
It stopes at prophase (diplotene stage) until puberty.
the 1st division finishes just prior to ovulation.2nd meiotic division – begins and stops at metaphase.
2nd division is completed after fertilization.
Ovulation:
Perifollicular CT broken by proteases, a fluid pressure increse until the follicle ruptures and the ovum separates from the follicle wall.
The ovum is drawn into open end of the oviduct (fallopian tube) and remains viable for 24 hr after ovulation.
the fertilization occurs in fallopian tubes.
Follicular atresia:
Degeneration of follicle that can occur at any stage. Phagocytes take up the dead oocyte freagments and follicular cells.
Common just after birth due to loss of maternal hormones, puberty and pregnancy.
The follicules died via apoptosis autolysis. And replaced by stromal cells (CT).
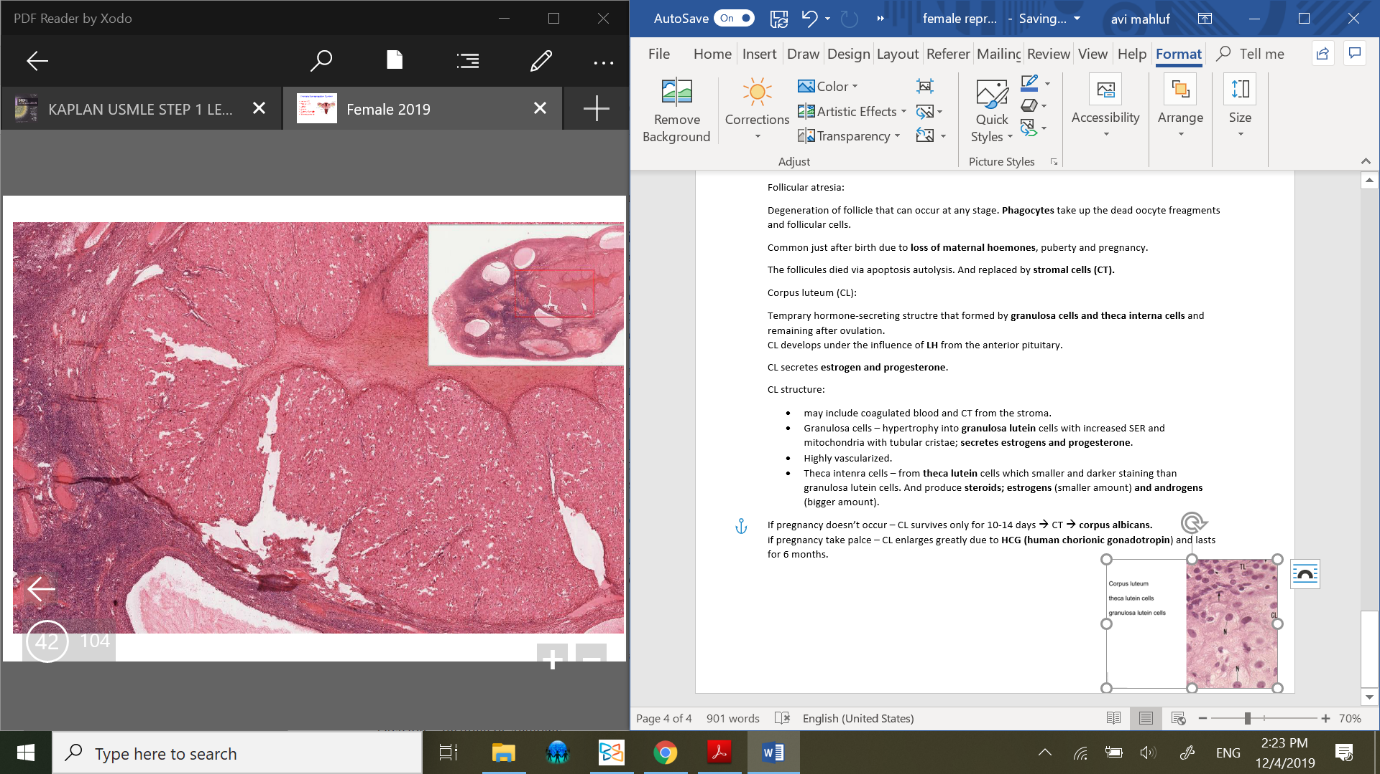
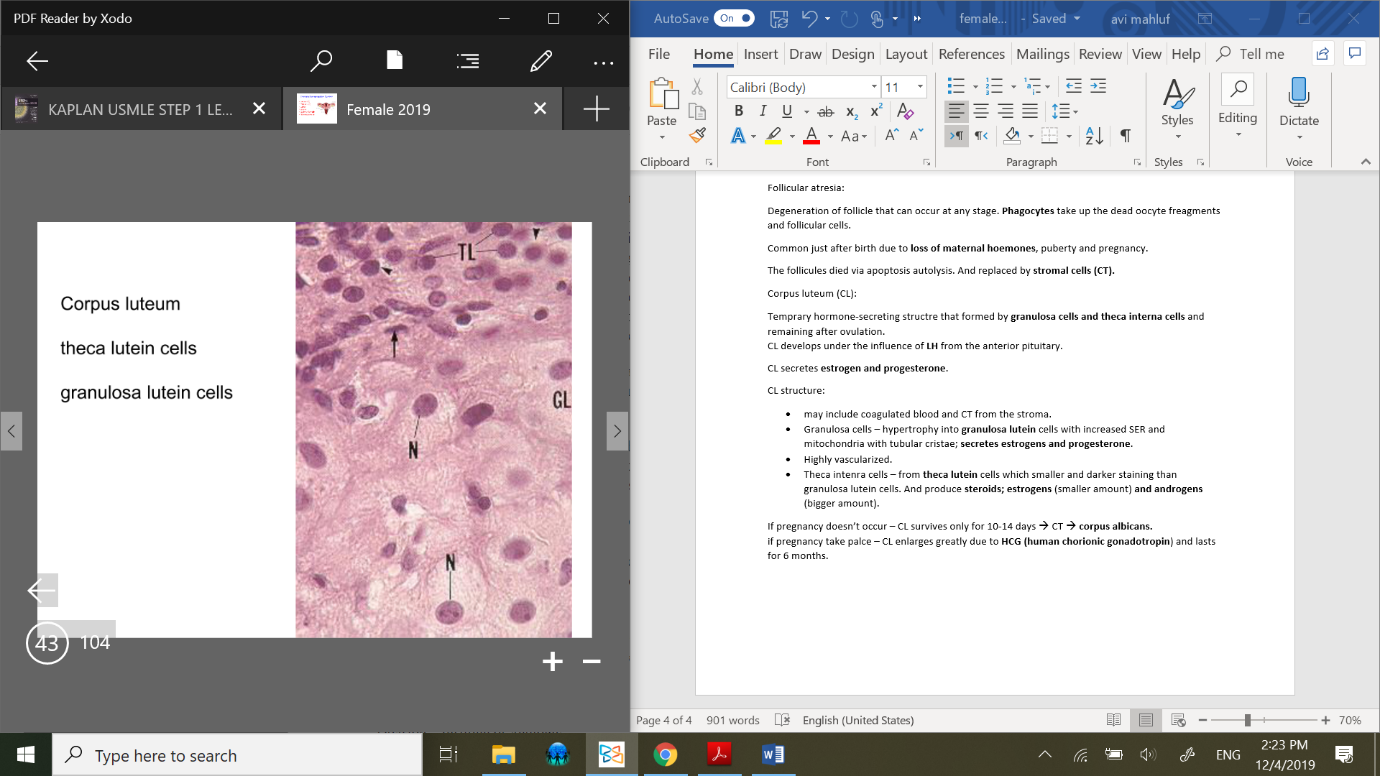
Corpus luteum (CL):
Temprary hormone-secreting structure that formed by granulosa cells and theca interna cells and remaining after ovulation.
CL develops under the influence of LH from the anterior pituitary.
CL secretes estrogen and progesterone.
CL structure:
may include coagulated blood and CT from the stroma.
Granulosa cells – hypertrophy into granulosa lutein cells with increased SER and mitochondria with tubular cristae; secretes estrogens and progesterone.
Highly vascularized.
Theca intenra cells – form theca lutein cells which smaller and darker staining than granulosa lutein cells. And produce steroids; estrogens (smaller amount) and androgens (bigger amount).
 If pregnancy doesn’t occur – CL survives only for 10-14 days 🡪 CT 🡪 corpus albicans.
If pregnancy doesn’t occur – CL survives only for 10-14 days 🡪 CT 🡪 corpus albicans.
if pregnancy take palce – CL enlarges greatly due to HCG (human chorionic gonadotropin) and lasts for 6 months.
Corpus albicans:
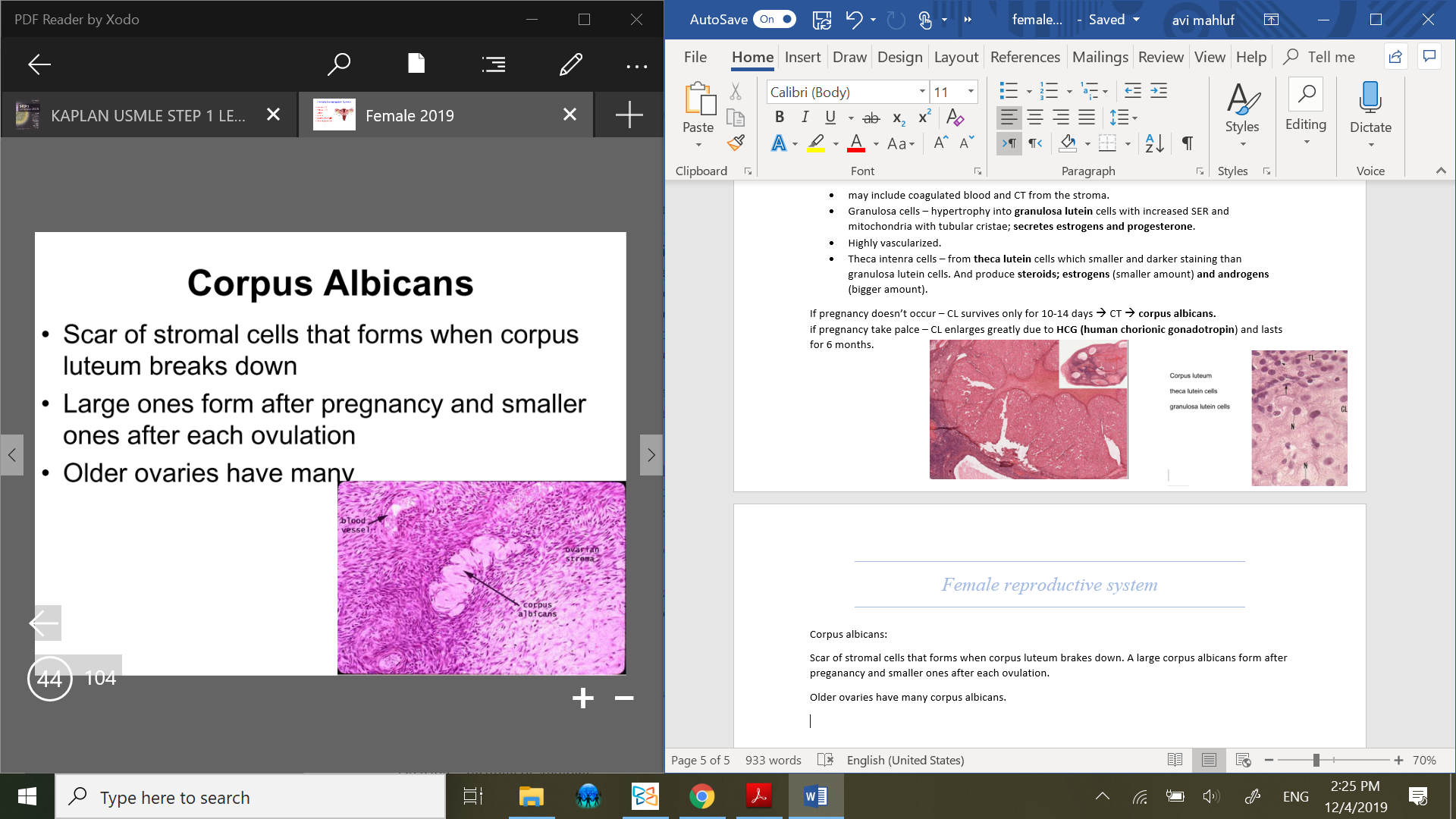 Scar of stromal cells that forms when corpus luteum brakes down. A large corpus albicans form after preganancy and smaller ones after each ovulation.
Scar of stromal cells that forms when corpus luteum brakes down. A large corpus albicans form after preganancy and smaller ones after each ovulation.
Older ovaries have many corpus albicans.
Oviduct:
A muscular tube of 12 cm. the upper end opens into peritoneal cavity near the ovary, where the lower end passes through the uterus wall.
4 segements of oviduct:
Intramural part – in uterine wall.
Isthmus – adjacent to uterine wall.
Ampulla – dilated part.
Infundibulum – funnel shaped part near ovary with fimbriae.
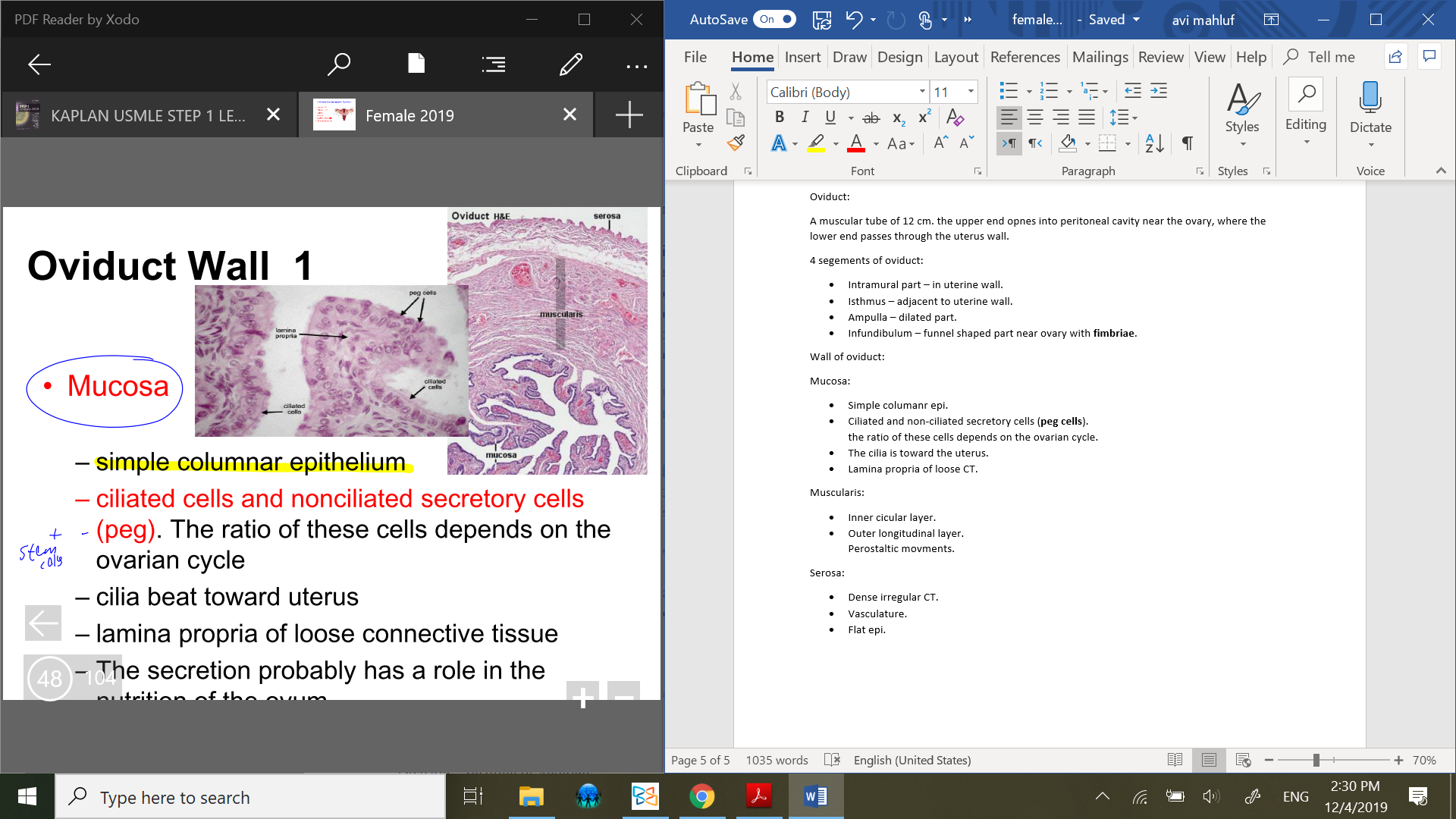
Wall of oviduct:
Mucosa:
Simple columanr epi.
Ciliated and non-ciliated secretory cells (peg cells).
the ratio of these cells depends on the ovarian cycle.The cilia is toward the uterus.
Lamina propria of loose CT.
Muscularis:
Inner cicular layer.
Outer longitudinal layer.
Perostaltic movments.
Serosa:
Dense irregular CT.
Vasculature.
Flat epi.
 Uterus:
Uterus:
7 cm long in non-pregnant state. Composed of; endometrium, myometrium and perimetrium.
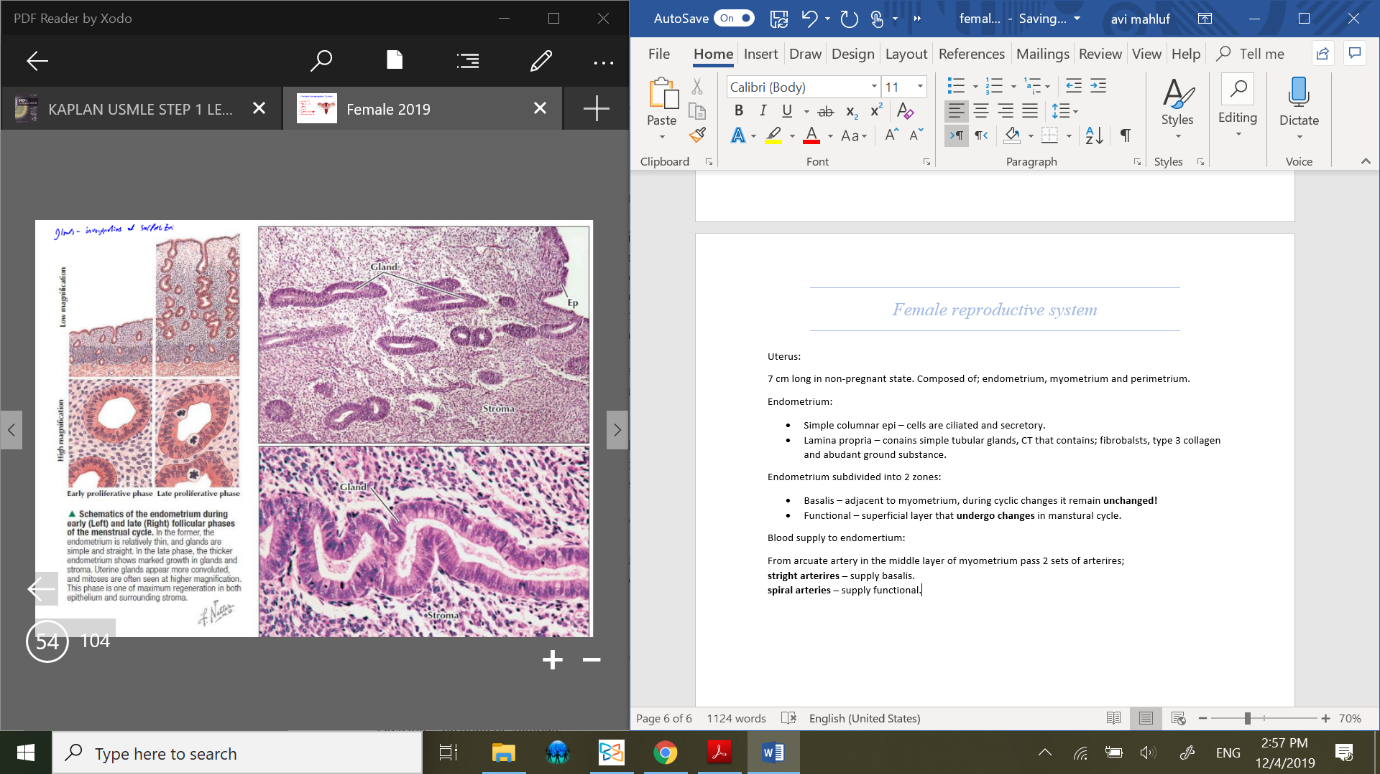
Endometrium:
Simple columnar epi – cells are ciliated and secretory.
Lamina propria – conains simple tubular glands, CT that contains; fibrobalsts, type 3 collagen and abudant ground substance.
glands – invegination of surface epi.
Endometrium subdivided into 2 zones:
Basalis – adjacent to myometrium, during cyclic changes it remain unchanged!
Functional – superficial layer that undergo changes in manstural cycle.
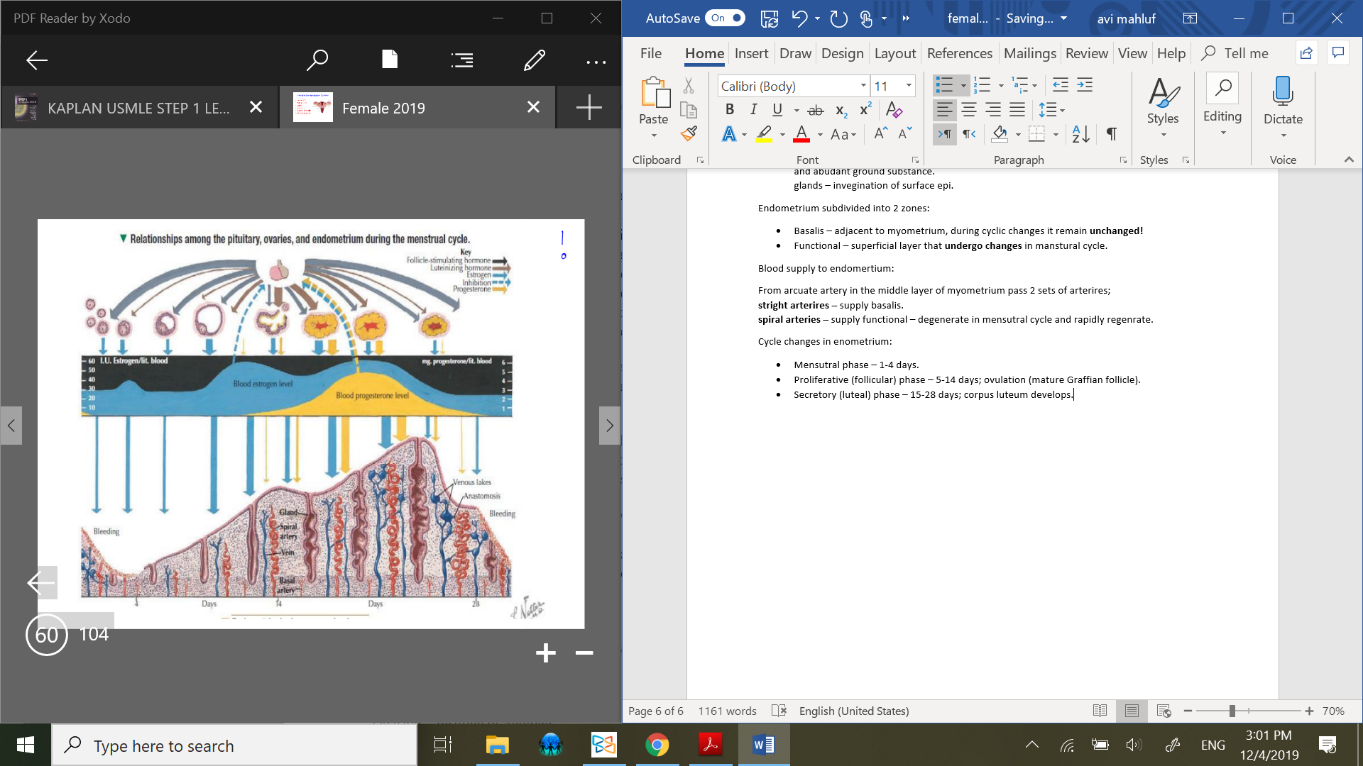
Blood supply to endomertium:
From arcuate artery in the middle layer of myometrium pass 2 sets of arterires;
stright arterires – supply basalis.
spiral arteries – supply functional – degenerate in mensutral cycle and rapidly regenerate.
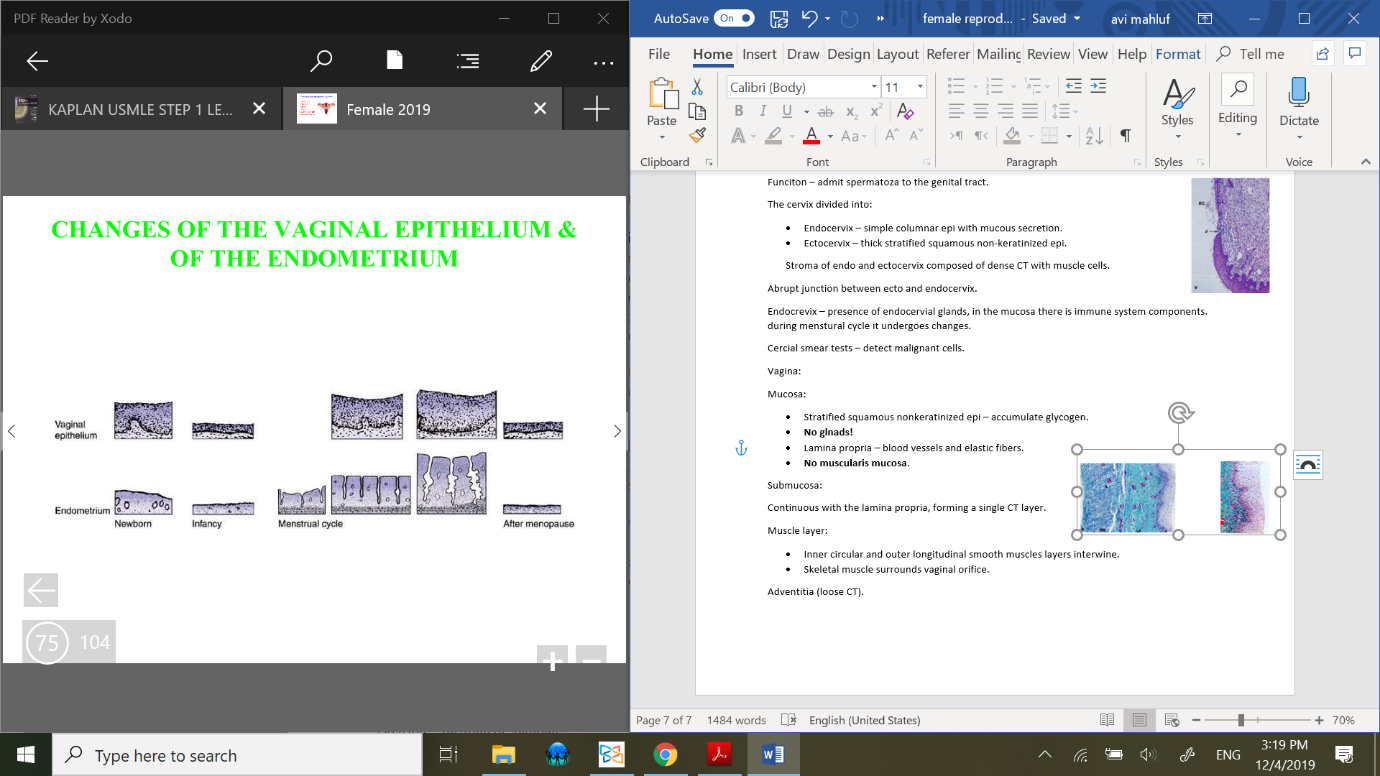
Cycle changes in enometrium:
Mensutral phase – 1-4 days.
Proliferative (follicular) phase – 5-14 days; ovulation (mature Graffian follicle).
Secretory (luteal) phase – 15-28 days; corpus luteum develops.
Menstrural cycle:
menstrual phase (1-4 days):
the 1st day of mensturation is 1st day of menstrual cycle.
in the absence of implantation degenrates CL and diminishes secretion of estrogen and progesteron.
results in constriction of spiral arterires and ischemia of functional layer of endometrium.
The ischemia leads to necorsis and degeneration of all stratum functionalis which shed; menses.
The menses composed of; blood, necrotic epi and stroma. Apoptotic endometrial cells.
Proliferative (follicular) phase (5-14 days):
Endometrial stroma proliferates and becomes thicker. The tubular glnads elongate and begins to secrete.
the thickinening of endometrium is from 0.5 mm to 2-3 mm.
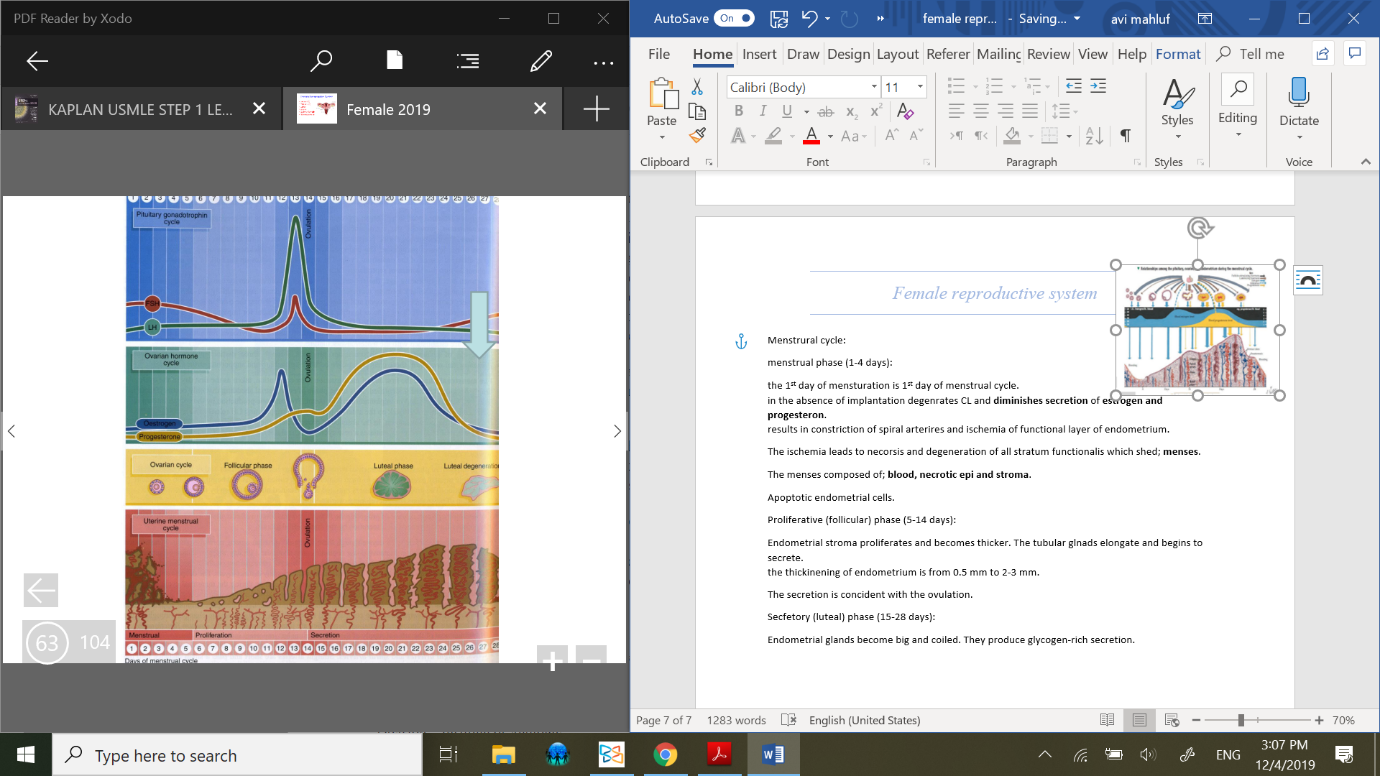 The secretion is concident with the ovulation.
The secretion is concident with the ovulation.
Secretory (luteal) phase (15-28 days):
 Endometrial glands become big and coiled. They produce glycogen-rich secretion.
Endometrial glands become big and coiled. They produce glycogen-rich secretion.
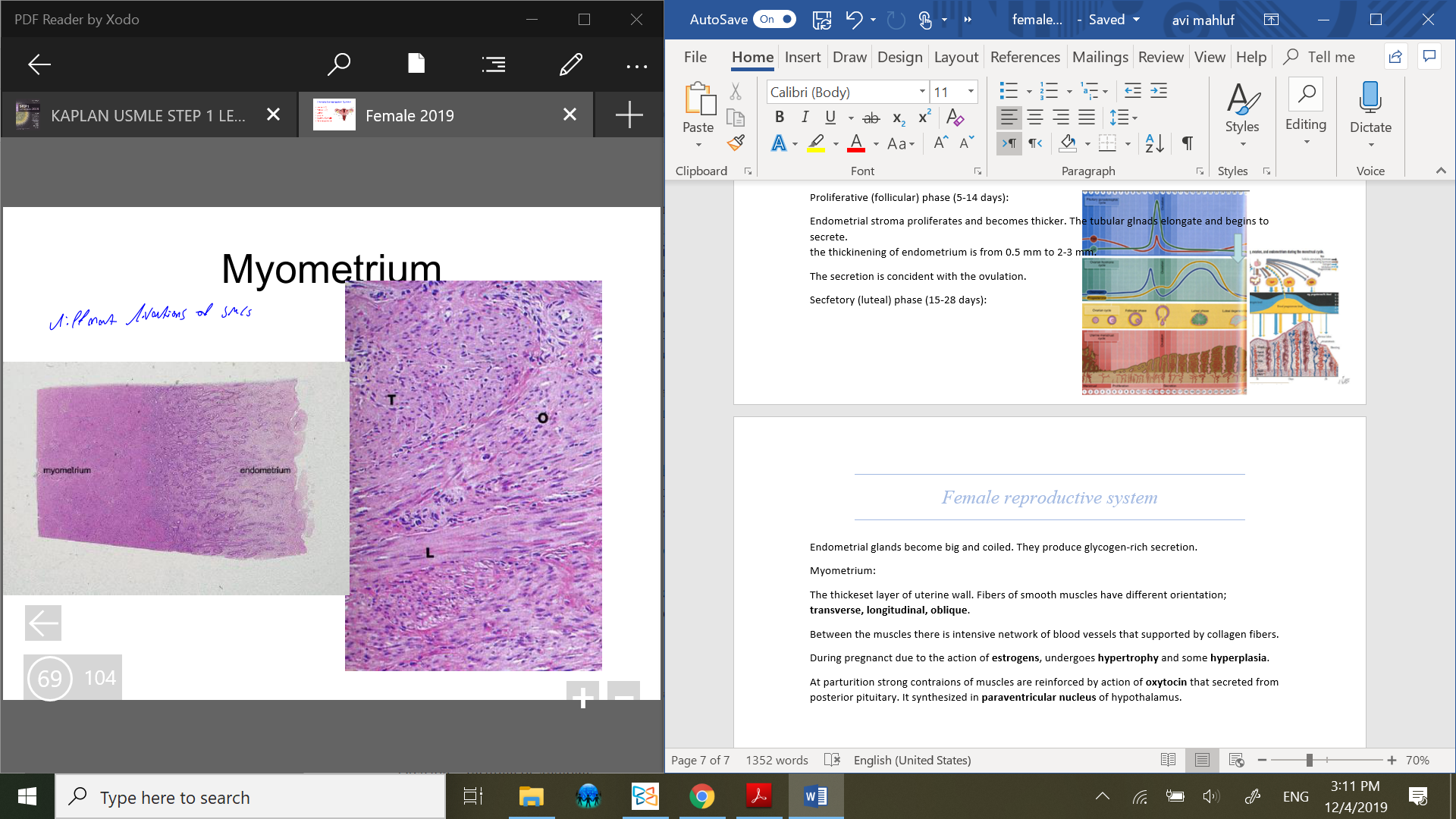
Myometrium:
The thickeset layer of uterine wall. Fibers of smooth muscles have different orientation;
transverse, longitudinal, oblique.
Between the muscles there is intensive network of blood vessels that supported by collagen fibers.
During pregnancy due to the action of estrogens, undergoes hypertrophy and some hyperplasia.
At parturition strong contractions of muscles are reinforced by action of oxytocin that secreted from posterior pituitary. It synthesized in paraventricular nucleus of hypothalamus.
Uterine cervix:
Protrudes into upper vagina. It contains endocertical canal that connects uterus and vagina.
Funciton – admit spermatoza to the genital tract.
The cervix divided into:
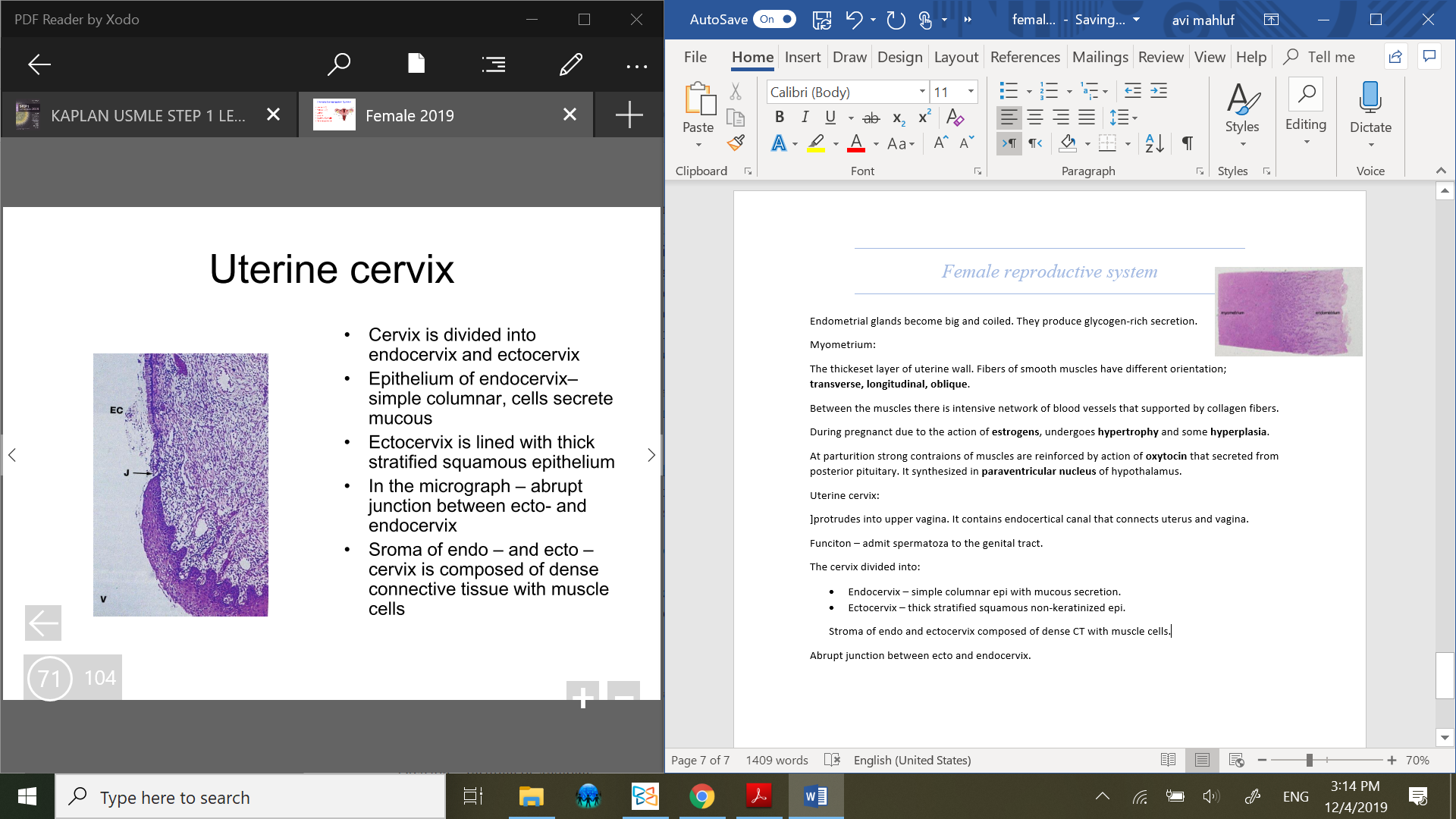 Endocervix – simple columnar epi with mucous secretion. presence of endocervial glands, in the mucosa there is immune system components. during menstural cycle it undergoes changes.
Endocervix – simple columnar epi with mucous secretion. presence of endocervial glands, in the mucosa there is immune system components. during menstural cycle it undergoes changes.Ectocervix – thick stratified squamous non-keratinized epi.
Stroma of endo and ectocervix composed of dense CT with muscle cells.
Abrupt junction between ecto and endocervix.
cervical smear tests – detect malignant cells.
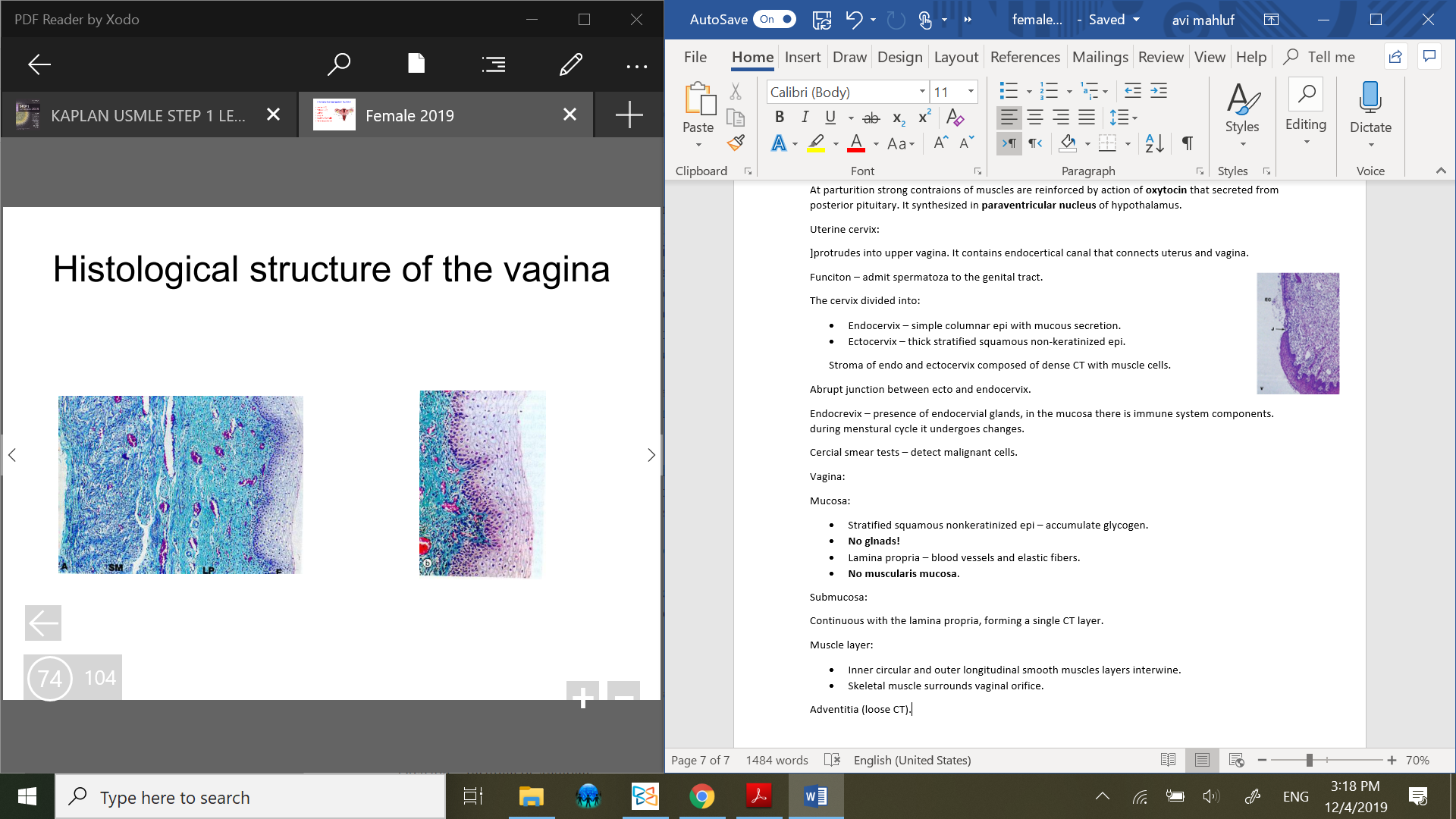
Vagina:
Mucosa:
Stratified squamous nonkeratinized epi – accumulate glycogen.
Lamina propria – blood vessels and elastic fibers.
No glnads!
No muscularis mucosa.
Submucosa:
Continuous with the lamina propria, forming a single CT layer.
Muscle layer:
Inner circular and outer longitudinal smooth muscles layers interwine.
Skeletal muscle surrounds vaginal orifice.
Adventitia (loose CT).
Brests (mammary glands):
Highly modified appocrine sweat glands. Until puberty brests have the same structure in both sexes.
After puberty the female brests develop under influence of pituitary, ovarian and other hormones.
the breasts undergo changes during ovarian cycle.
After menopause the brests like other female reproductive tissues undergo progressive atrophy and involution.
Structure:
Each breast consists of 15-25 brest lobes, each lobe consist of compoud tubulo-acinar glands.
Each lobe has lactiferous duct that before opening forms dilatation; sinus.
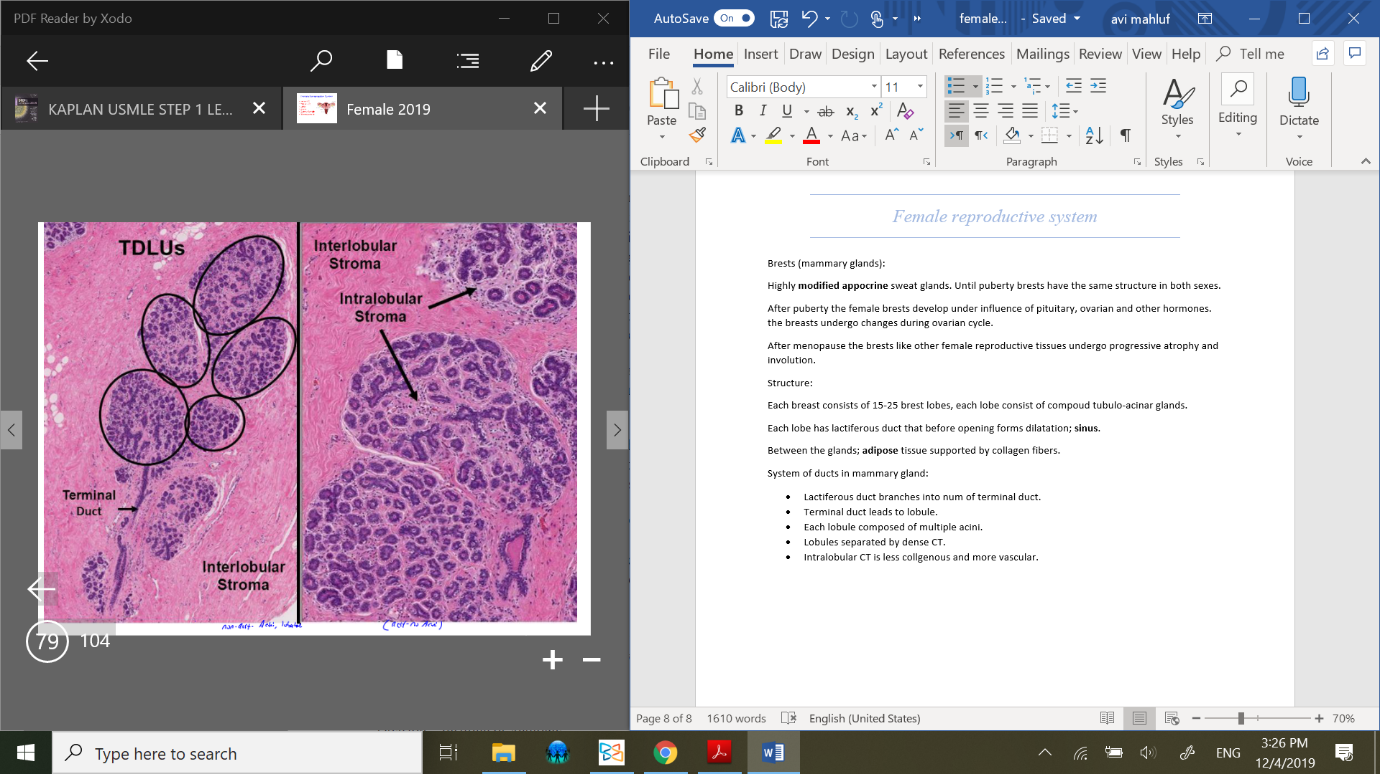 Between the glands; adipose tissue supported by collagen fibers.
Between the glands; adipose tissue supported by collagen fibers.
System of ducts in mammary gland:
Lactiferous duct branches into num of terminal duct.
Terminal duct leads to lobule.
Each lobule composed of multiple acini.
Lobules separated by dense CT.
 Intralobular CT is less collgenous and more vascular.
Intralobular CT is less collgenous and more vascular.
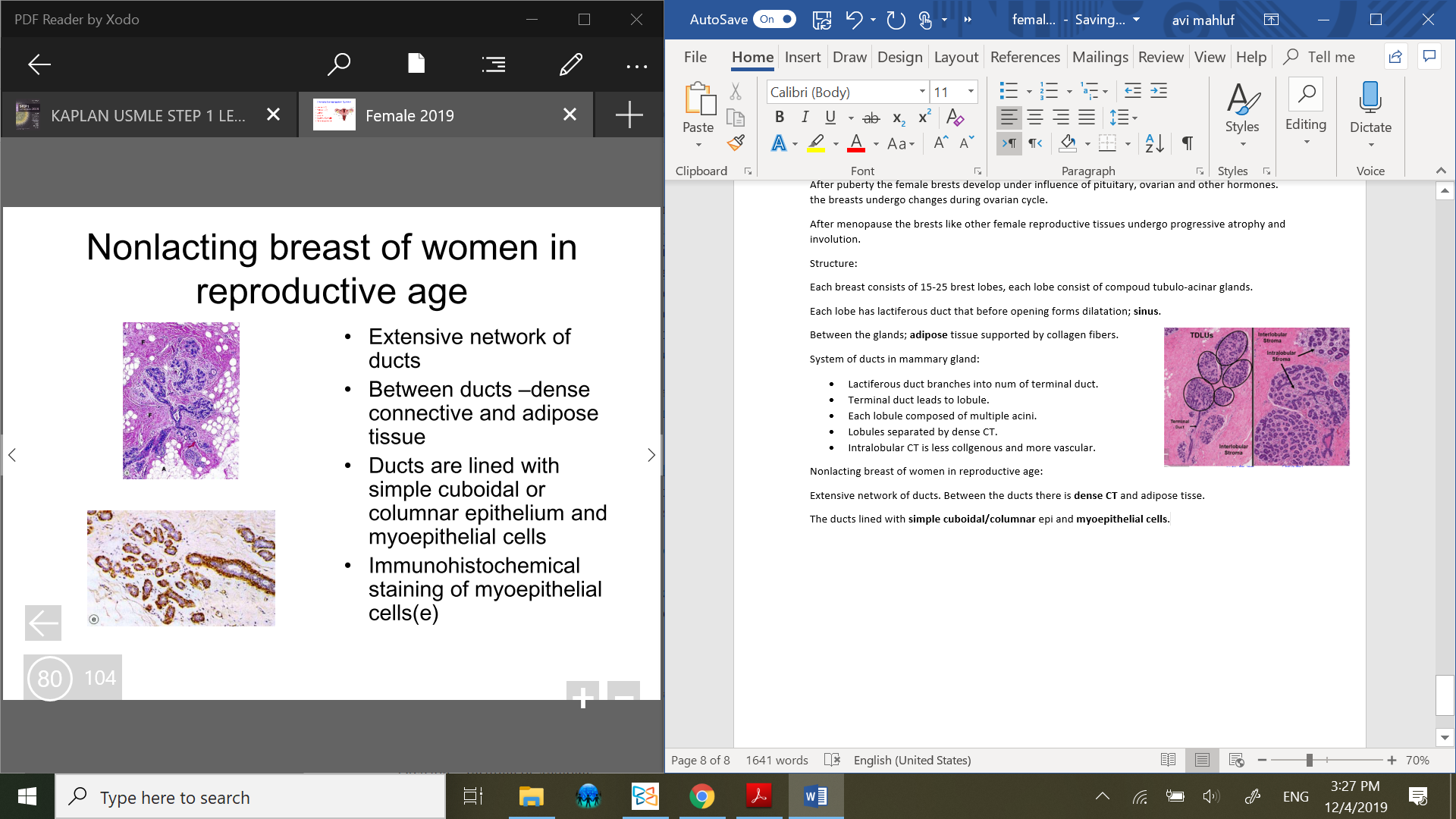
Nonlacting breast of women in reproductive age:
Extensive network of ducts. Between the ducts there is dense CT and adipose tisse.
The ducts lined with simple cuboidal/columnar epi and myoepithelial cells.
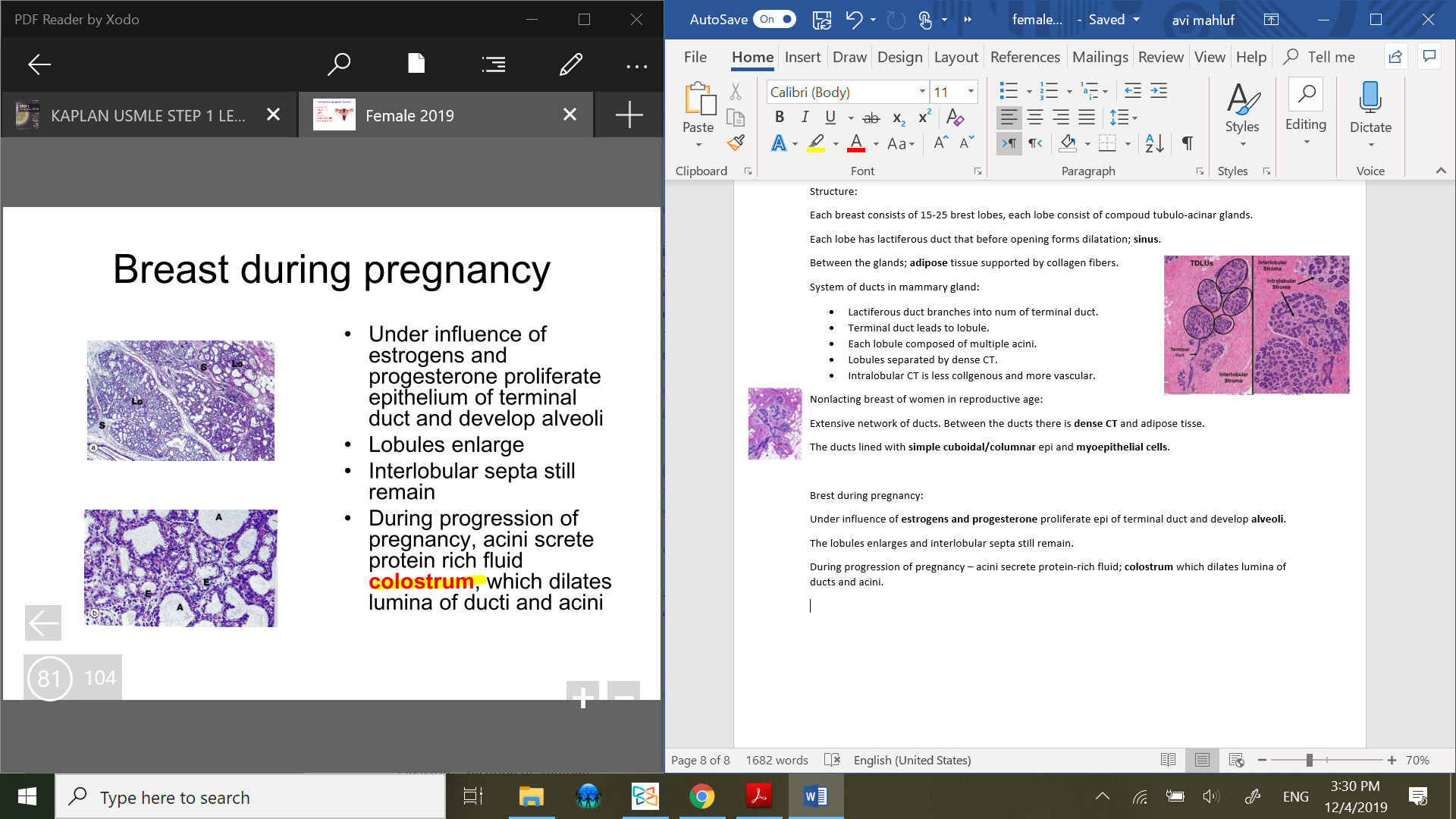
Brest during pregnancy:
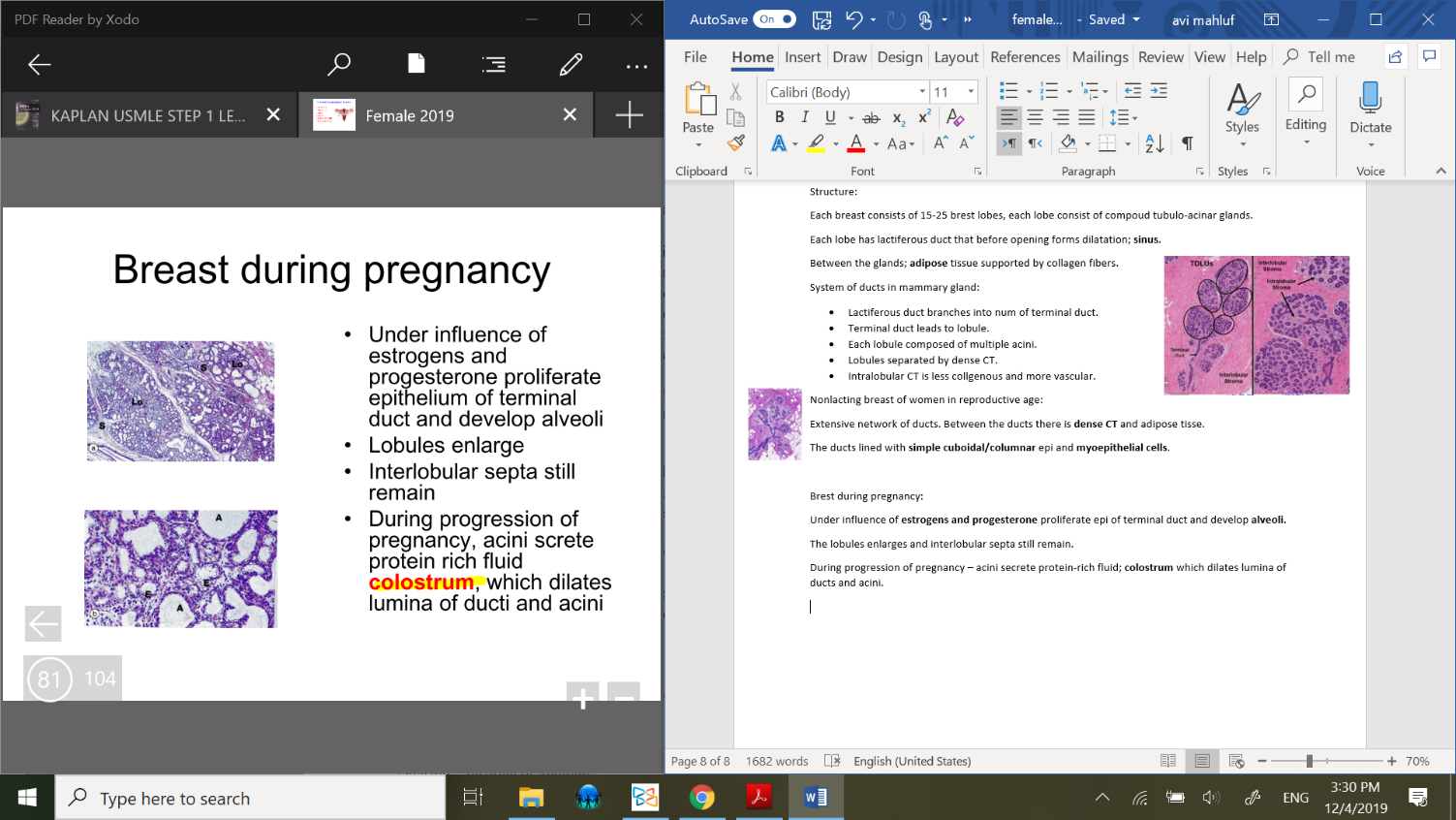 Under influence of estrogens and progesterone proliferate epi of terminal duct and develop alveoli.
Under influence of estrogens and progesterone proliferate epi of terminal duct and develop alveoli.
The lobules enlarges and interlobular septa still remain.
During progression of pregnancy – acini secrete protein-rich fluid; colostrum which dilates lumina of ducts and acini.
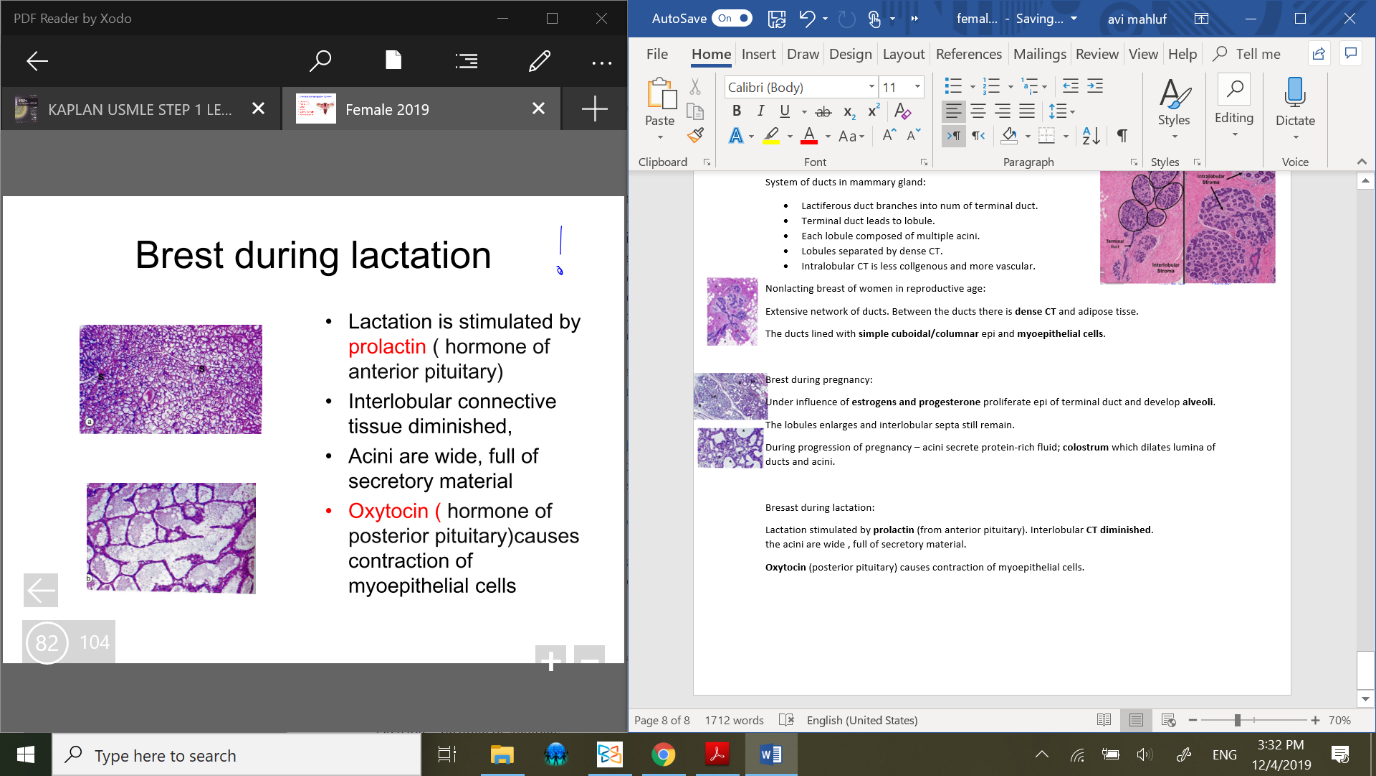
Bresast during lactation:
Lactation stimulated by prolactin (from anterior pituitary). Interlobular CT diminished.
the acini are wide , full of secretory material.
Oxytocin (posterior pituitary) causes contraction of myoepithelial cells.
Menarche:
1st menstrual cycle. The culmination of serires of physiological and anatomic processes of puberty;
attainment of a sufficient body mass (17% body fat).
Adipose tissue can convert adrenal androgens into estrogens.
releasing GnRH in arcuate nucleus of hypothalamus 🡪 estrogen secreted by ovareis due to pituitary hormones.
Over an interval of 2-3 years, estrogen stimulates growth of uterus, height growth, breast, widening of pelvis and increased regional adipose tissue.
Estrogen also stimulates growth and vascularity of one endometrium.
Fluctations of hormone levels can result in changes of adequacy of blood supply to parts of endometrium.
Development of female reproductive system:
Sex of embryo determined genetically at fertilization by Y-chromosome which has SRY (sex-determining region on Y). its Protein is the testis-determining factor🡪 male.
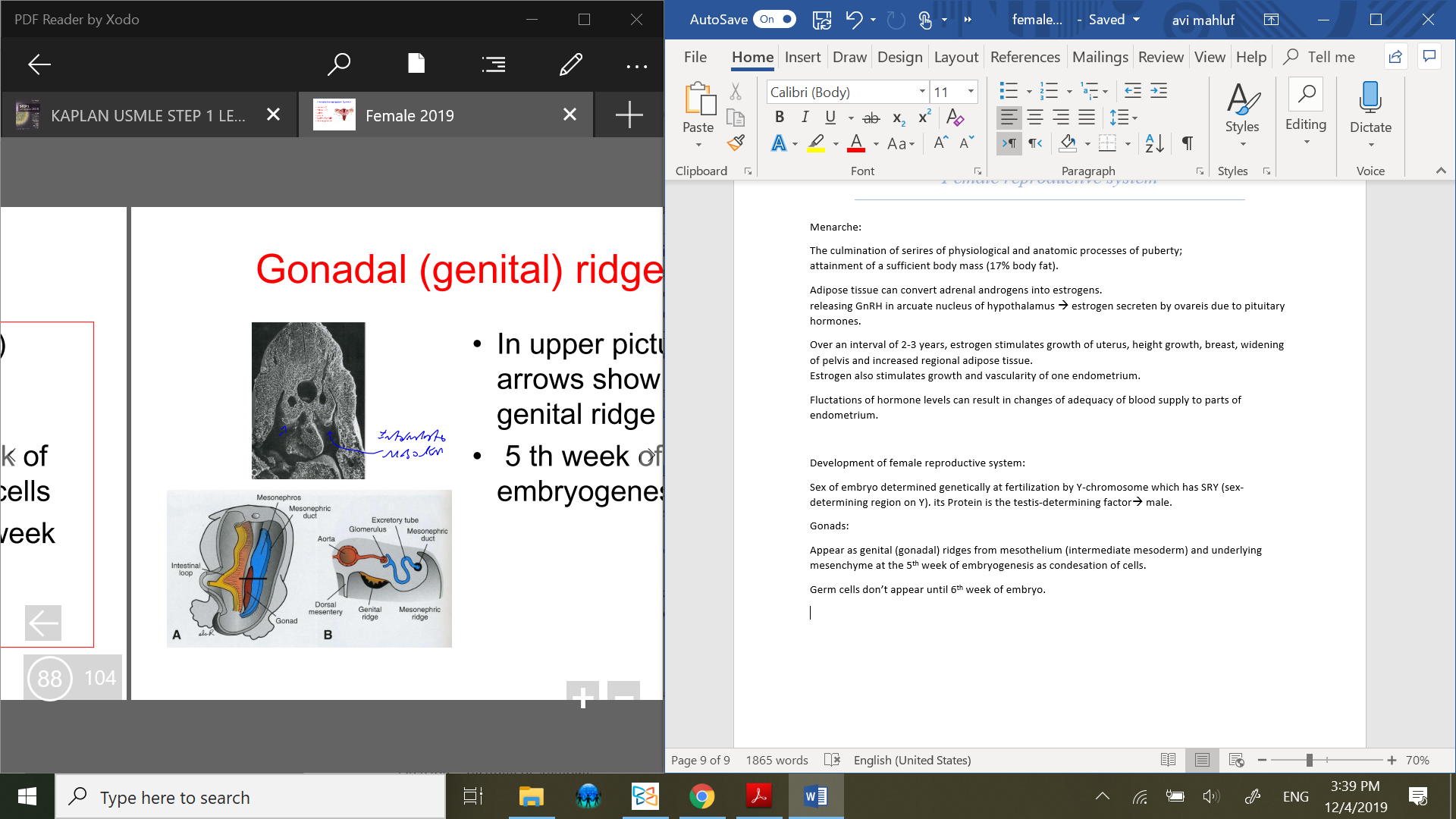
Gonads:
Appear as genital (gonadal) ridges from mesothelium (intermediate mesoderm) and underlying mesenchyme at the 5th week of embryogenesis as condesation of cells.
Germ cells don’t appear until 6th week of embryo.
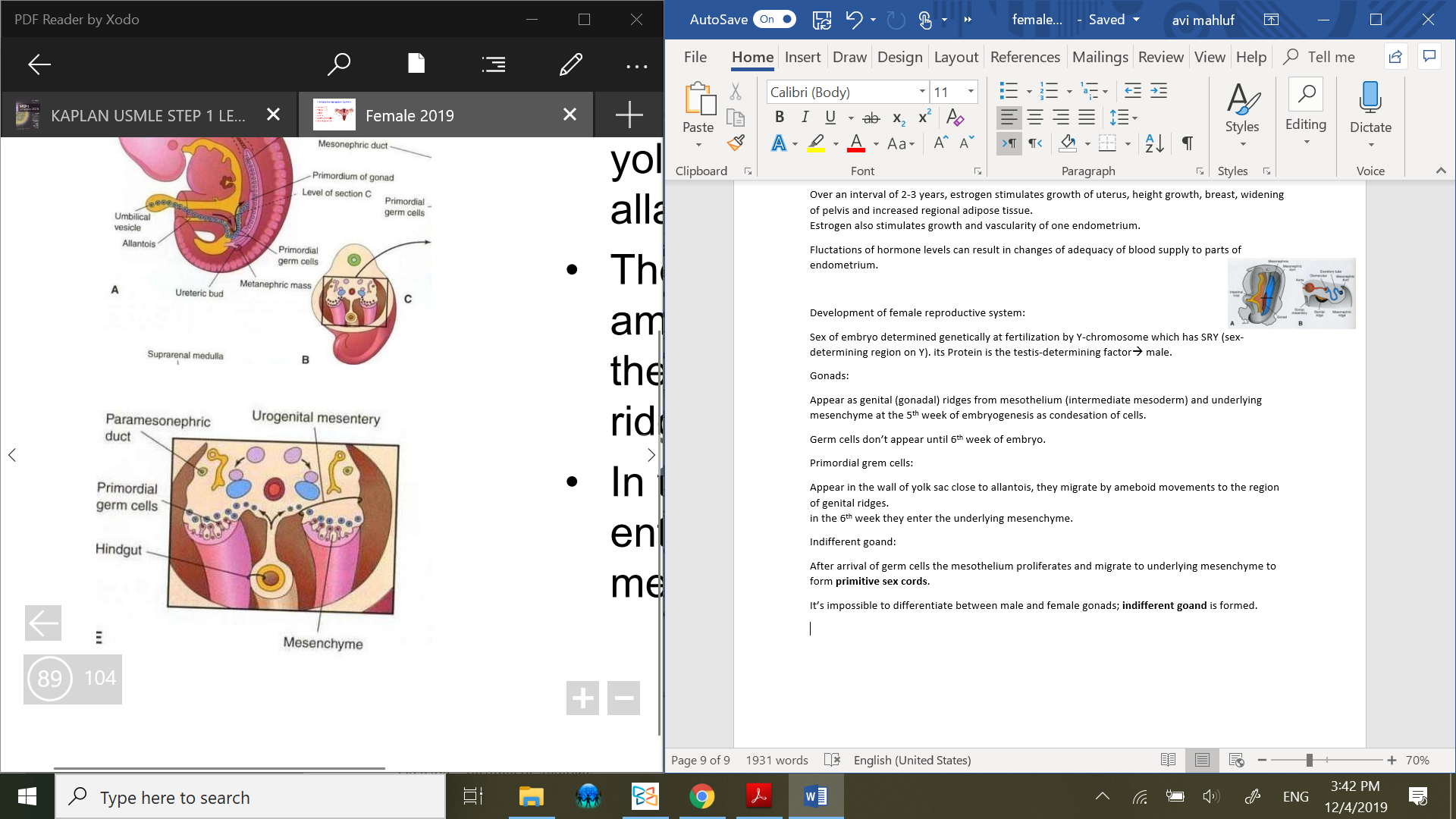
Primordial grem cells:
Appear in the wall of yolk sac close to allantois, they migrate by ameboid movements to the region of genital ridges.
in the 6th week they enter the underlying mesenchyme.
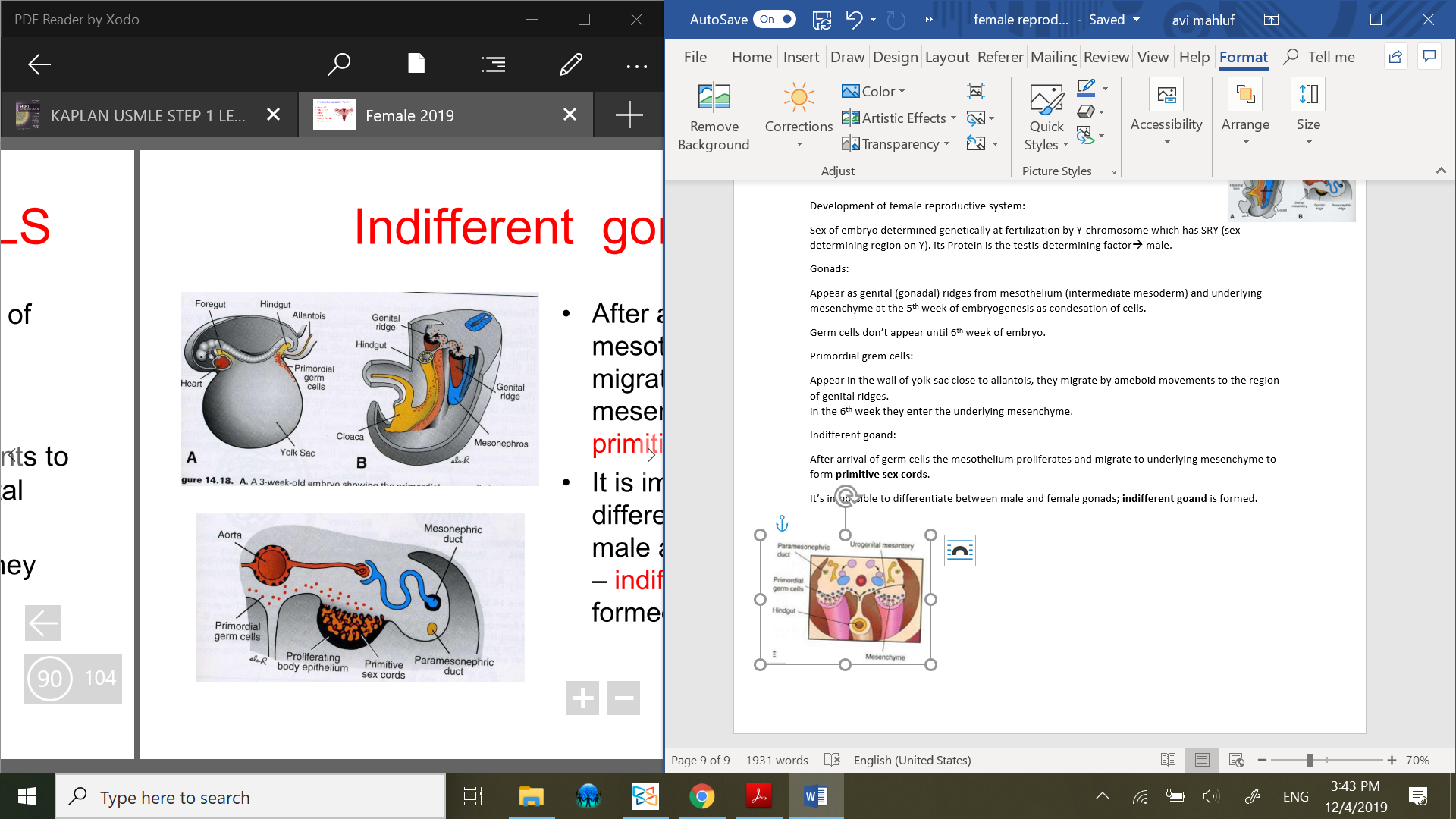
Indifferent goand:
After arrival of germ cells the mesothelium proliferates and migrate to underlying mesenchyme to form primitive sex cords.
It’s impossible to differentiate between male and female gonads; indifferent goand is formed.
Ovary development:
From 7th week of embryogenesis starts development of the ovary. Primitive sex cords form irregular cell clusters 1st in medullar part of ovary.
later they degenerate and replaced by vascular stroma that forms the ovarian medulla.
The surface epi (mesodermal origin) proliferate and in the 7th week form the surface epi develops the cortical cords.
In the 4th month these cords isolate cell clusters derived from medullary cords.
From surface epi develop; follicular cells.
Genital ducts; indifferent stage:
In both; male and female present mesonephric and paramesonephric (Mullerian) ducts. They develop from coelomic epi.
From paramesonephric ducts develop:
female – oviduct, uterus, parts of vagina.
male – disappears.
Genital ducts in female:
Main ducts develop from paramesonephric duct. It’s possible to differentiate 3 parts in each duct;
Cranial vertical portion – opens into abdominal cavity.
Horizontal part.
Caudal vertical part – fuses with the duct from opposite side.
the descending vertical part develop into uterine tube, uterine canal that at the beginning separated by septa. Fused caudal parts finally form corpus and cervix of uterus.
Vagina development:
Paramesonephric duct reaches the urogenital sinus. At 1st develop sinovaginal bulbs and later vaginal plate.
The vaginal plate proliferates and at 5th month becomes canalized.
finally the vagina develops from 2 sources;
Uterine canal.
Urogenital ridge.
From upper urogenital sinus develop urinary bladder.
from pelvic part of urogenital sinus all female urethra and prostatic-membranous parts of male urethra.
from lower urogenital sinus develop spongy part of male urethra and vagina (1/4, lower part) and vaginal vestibule.
External genitalia; indifferent stage:
In 3rd week mesenchymal cells from primitive stark migrate around cloacal membrane and form;
cloacal folds, genital tubercle.
Later cloacal fold is subdivided into; urethral fold and anal fold.
At the same time develop another pair of elevations; genital swellings.
genital swellings in male develop into scrotal swellings and in female; labia majora.
From genital tubercle – develops clitoris.
from urethral folds – develops labia minora.
Period of gonads and external genitalia differentiation:
Gonads develop 1st! (at the beginning of 7th week). The external genitalia possible to differentiate at the 9th week.