Air Polishing
Purpose & Key Features:
Efficient removal of stains and biofilm
Delivers adjustable slurry: air + water + powder
Propels abrasive particles to the tooth surface
Pressures:
Air pressure: 40–100 PSI
Water pressure: 20–60 PSI
Uses & Advantages:
Advantages:
NO heat generation
ergonomic> than handpiece polishing
powders are less abrasive than polishing paste
Uses:
Removes extrinsic staining (heavy): Tobacco, chlorhexidine, and betel
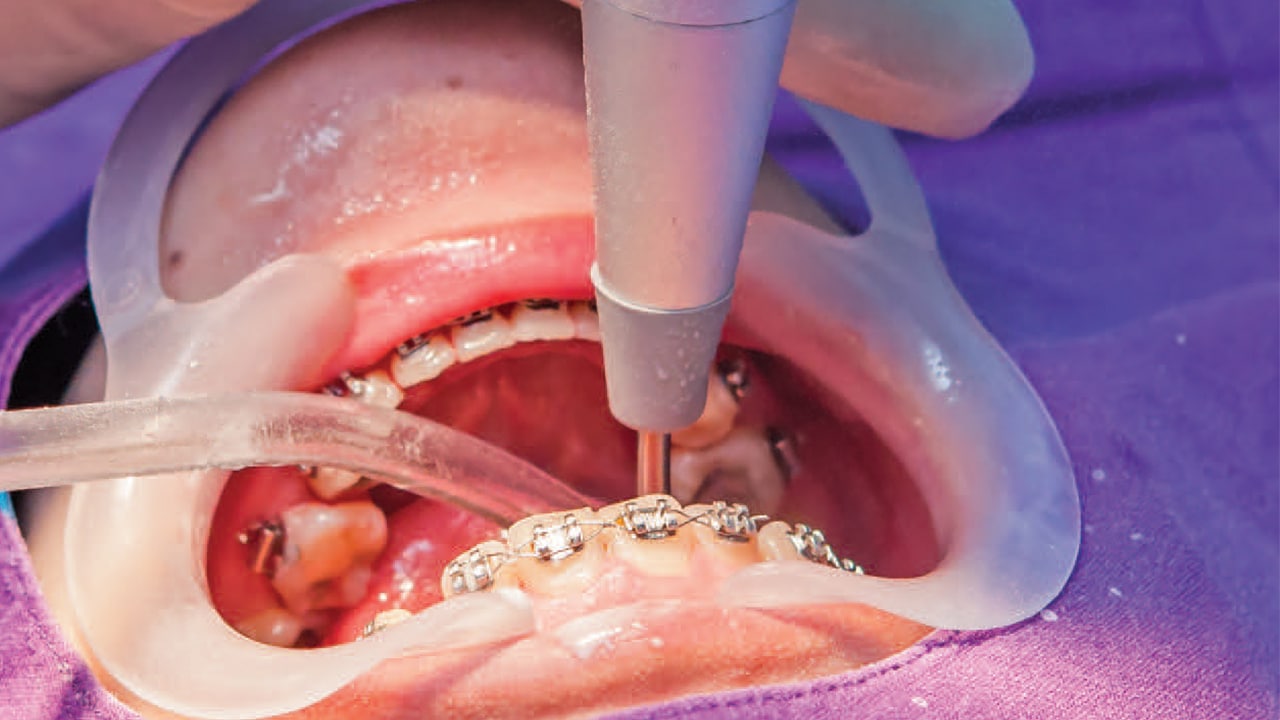
Preferred for orthodontic appliances
Acceptable before sealant placement
Personal Protective Equipment (PPE)
Clinician (mandatory): Level 3 mask or higher, gown, gloves, face shield
Patient: Eye protection (prescription glasses or safety glasses), Mask + shield combination, and extra bib or paper towel

Contraindications
Systemic (Air polishing):
Respiratory disease or swallowing/breathing disorders: asthma, COPD, cystic fibrosis, and pulmonary hypertension
Communicable airborne diseases: cold, flu, and COVID.
Very immunocompromised patients: AIDS, cancer treatment, uncontrolled diabetes, immunosuppressive meds, hemophilia, neutropenia, agranulocytosis

Oral contraindications (air polishing):
open wounds
≤3 mm supporting alveolar bone → risk of subcutaneous emphysema
Caused by angulation into sulcus
Symptoms: swelling, tenderness, crackling sensation, and extreme pain
Management: emergency treatment, observation, antibiotics, and analgesia

Systemic (Prophy-Jet technique):
End-stage renal disease, Addison’s disease, Cushing’s disease, metabolic alkalosis
Patients on potassium, antidiuretics, or steroid therapy

Oral contraindications (Prophy-Jet):
Root surfaces, Soft, spongy, or inflamed gingiva

Systemic (Sodium bicarbonate only):
sodium-restricted diet, high blood pressure, kidney disease, heart problems

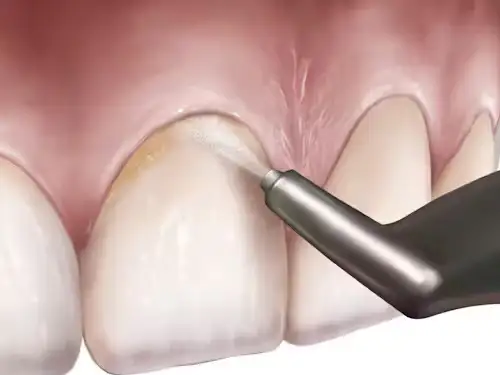
Technique — Nozzle Position & Angulation
Prophy-Jet Technique:
Nozzle 4–5 mm from tooth
Anterior teeth: 60° to the facial/lingual surfaces
Posterior teeth: 80° to buccal/lingual surfaces
Occlusal surfaces: 90° to occlusal surfaces

Air-Flow Technique:
Supragingival:
Nozzle 2–5 mm from tooth
Angulation: use between 15°–80° (avoid 90°)

Subgingival (plastic tip):
Insert inactive tip to base of pocket, slide apically until contact with JE, withdraw 1 mm coronally (away from base)
Activate and apply 5 seconds with overlapping vertical strokes
FDA: approved for pockets ≤5 mm (Canada: ≤10 mm)
Note: tip directs to root surface, not base of pocket

Powders — Properties & Indications
Sodium Bicarbonate (SB)
Original powder: salty taste and may sting
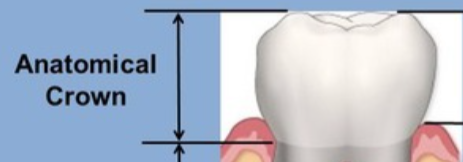
Use: anatomical crown only
Compatible: amalgam, gold, porcelain; NOT for some restorations or root surfaces
Mohs hardness: 3.0 size: 74 µm
Aluminum Trihydroxide
Alternative to SB
Use: anatomical crown only; not for restorations
Mohs: 4.0 size: 80 µm

Calcium Carbonate
Main ingredient in antacid
Use: anatomical crown only; effect on restorations unknown
Mohs: 3.0 size: 45 µm
Calcium Phosphosilicate
Bioactive glass — researchers warn against use (destructive to enamel/root)
Mohs: 6.0 size: 120 µm

Glycine
Amino acid powder
Reduces abrasiveness to the root by ~80% vs SB
Use: supra- and subgingival; safe on all restorations
Also detoxifies the root surface
Mohs: 2.0 size: 20 µm

Erythritol
Water-soluble polyol (sweetener)
Use: supra- and subgingival; safe on all restorations
Detoxifies the root surface
Mohs: <2.0 size: 14 µm

Clinical Reminders
Always review manufacturer instructions and powder compatibility with restorations and root surfaces