Skeletal muscle
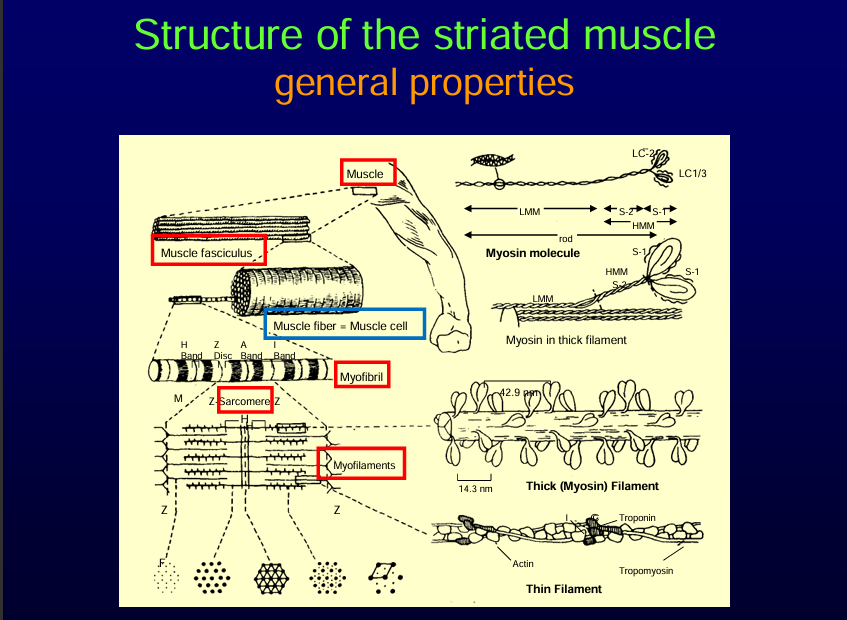
Structrure of striated muscle
Thin and thick filaments make up the sarcomere——> group of sarcomere———>group of myofibril——→ group of muscle fibre———> muscle fasciles.
Note:
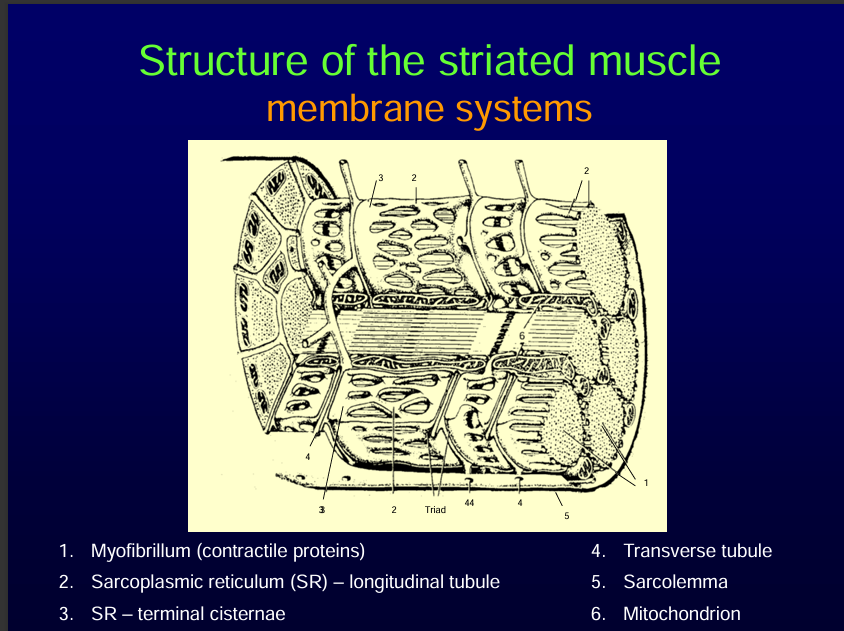
Sarcoplasmic reticulum is the endoplasmic reticulum in the muscle cells.
It is responsible for calcium storage.
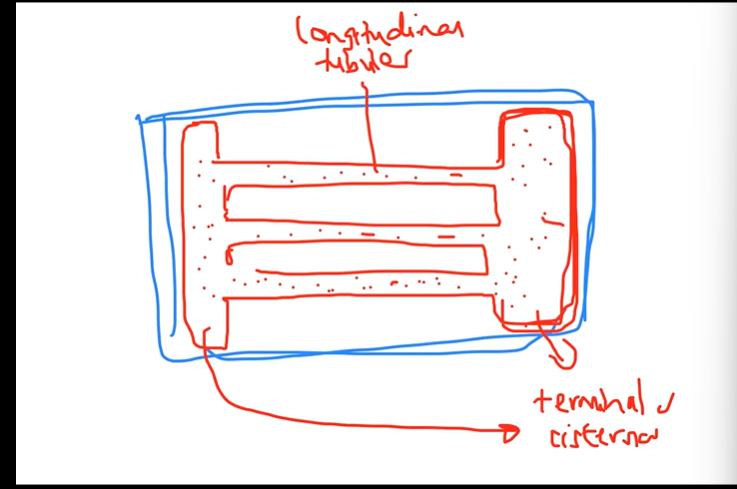
It has two parts:
1. Longitudinal tubules. 2.Terminal cisternea. SEE DIAGRAM BELOW
Sarcolemma is the plasma membrane of the muscle cell.
The sarcolemma has T tubules (Transverse tubule). T-tubules are invaginations (foldings) of the sarcolemma that dive deep into the muscle fiber.
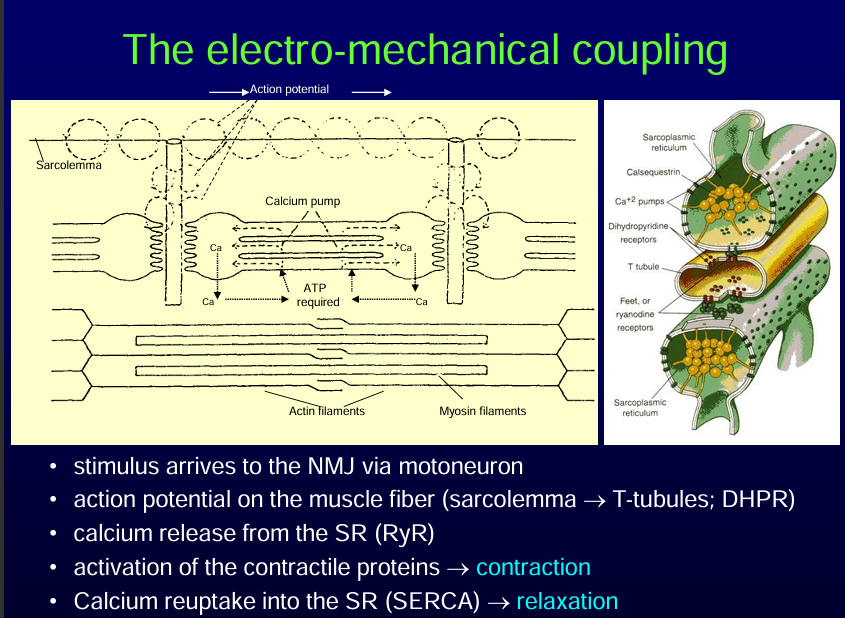
Electro-Mechanical Coupling Steps
Neuromuscular Junction (NMJ) Stimulation
A stimulus arrives via a motoneuron.
Acetylcholine (ACh) is released at the NMJ, binding to receptors on the sarcolemma, initiating a muscle action potential.
Action Potential Propagation
The action potential spreads along the sarcolemma and dives into the T-tubules.
Voltage-sensitive DHPR (dihydropyridine receptors) in the T-tubules detect the depolarization. DHPR is a volatage gated calcium channel.
Calcium Release from the Sarcoplasmic Reticulum (SR)
DHPRs mechanically interact with RyR (ryanodine receptors) on the SR membrane. DHPR and RyR are coupled with each other.
RyR opens, causing calcium ions (Ca²⁺) to flood into the cytosol.
Activation of Contractile Proteins → Contraction
Calcium binds to troponin (Tc subunit), causing a conformational change that moves tropomyosin off actin binding sites.
Myosin heads bind to actin, and cross-bridge cycling occurs → muscle contraction.
Calcium Reuptake → Relaxation
Calcium is actively pumped back into the SR via SERCA (Sarcoplasmic/Endoplasmic Reticulum Calcium ATPase).
Cytosolic calcium decreases, troponin-tropomyosin complex blocks actin sites, and the muscle relaxes.
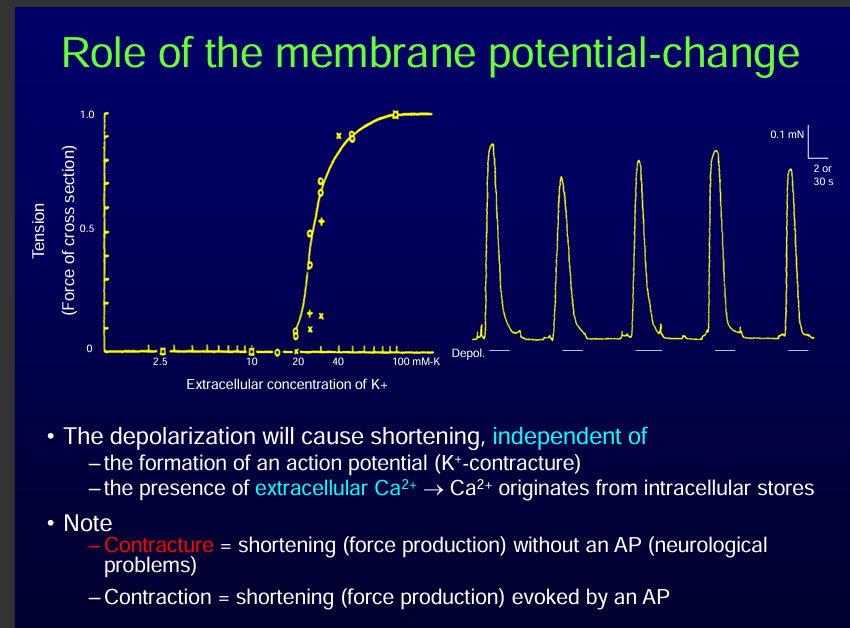
NOTE: Contraction of a muscle without an action potential is called a contracture.
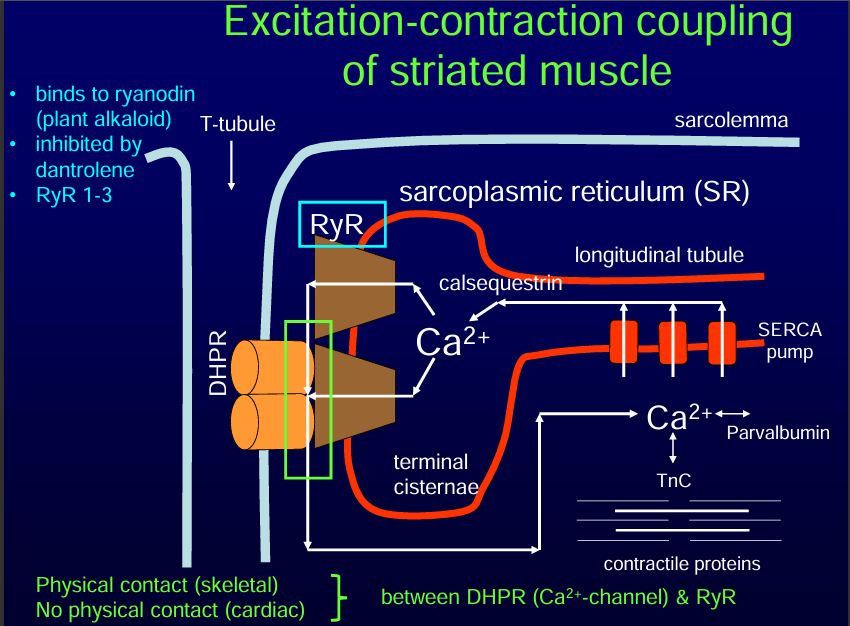
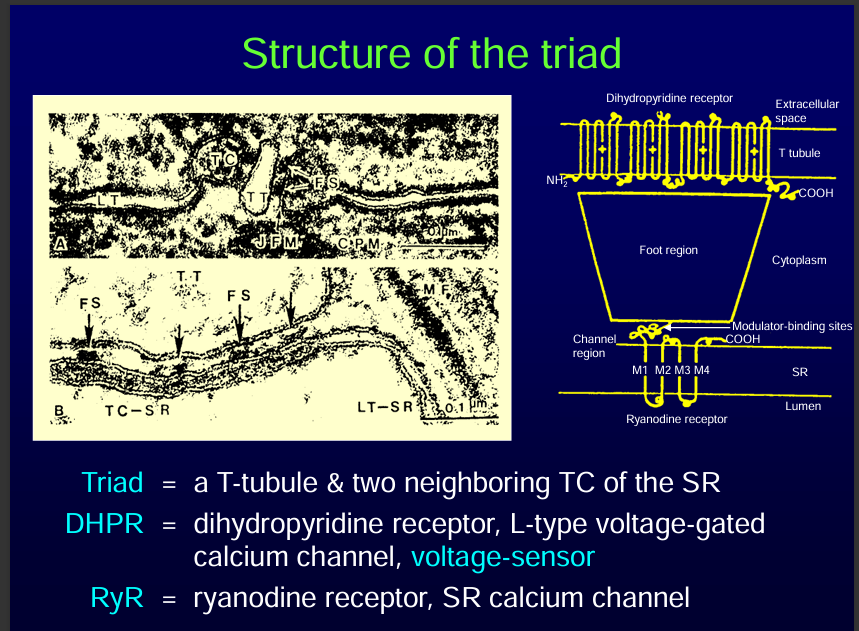
A triad is a T-tubule and two neighbouring Terminal cisternae of the sarcoplasmic reticulum.
Differences between the skeletal muscle and cardiac muscle:
The skeletal muscle has a triad while cardica muscle has a diad
Extracellular calcium is not needed for skeletal muscle contraction rather, calcium is released from the sarcoplasmic reticulum while for cardiac muscle, extracellular calcium is needed for contraction.
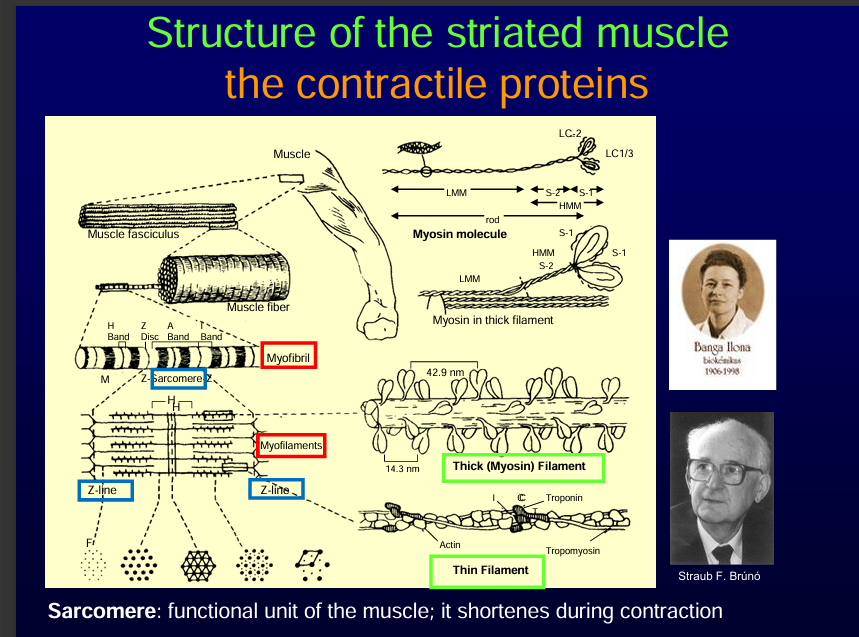
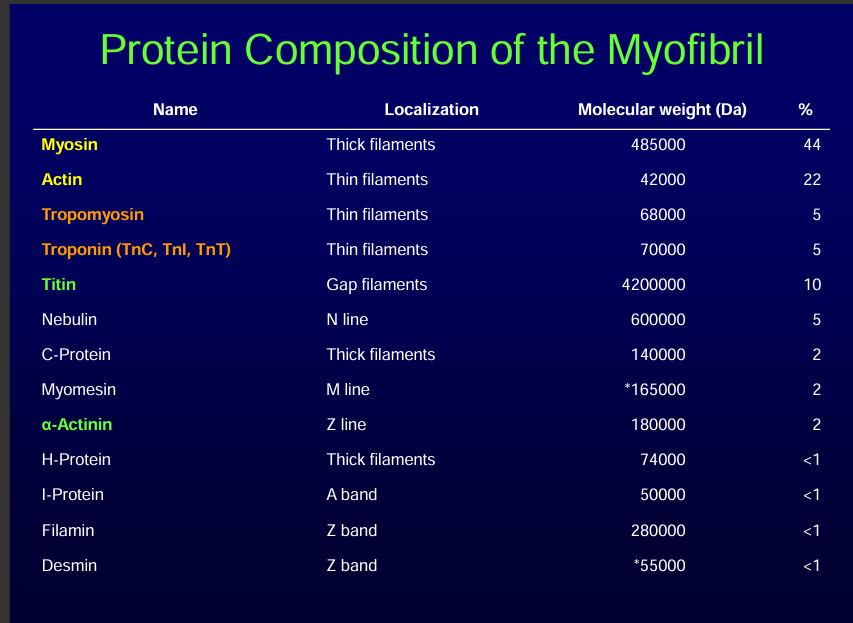
The contactile protein
Thick: myosin
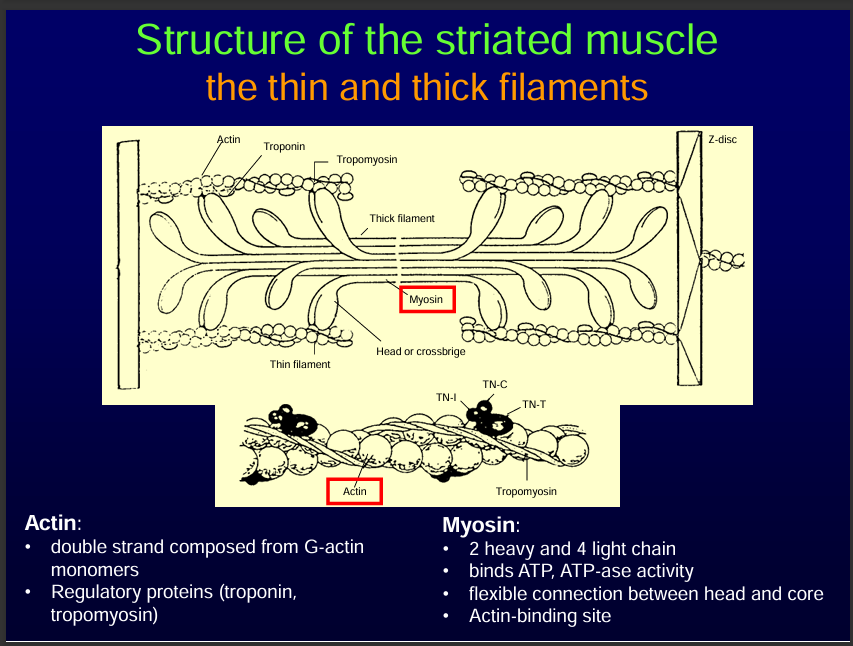
Thin: actin+tropomysosin+troponin
Sarcomere us the basic functional unit of the muscle. It shortens during contraction.
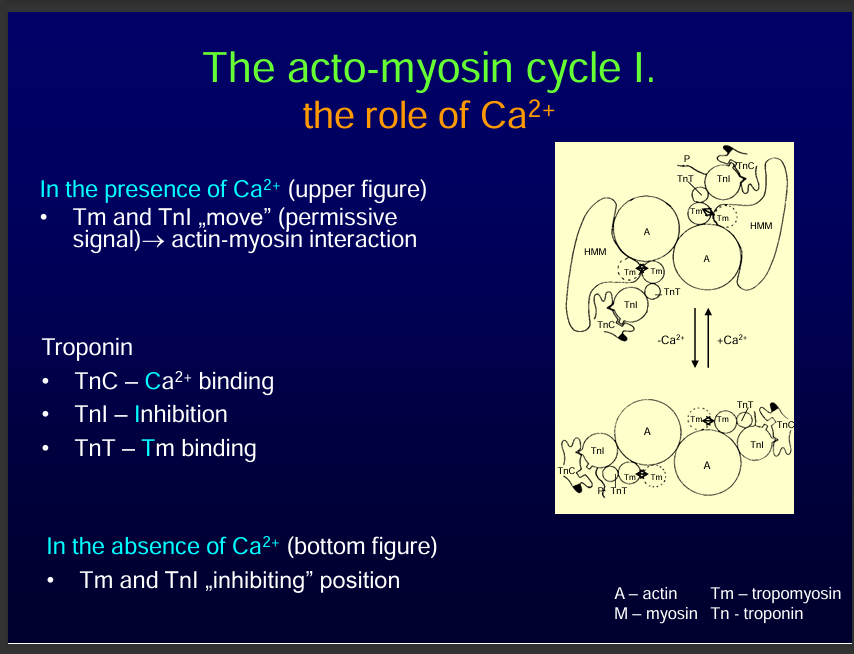
In the presence of calcium, calcium Binds to Troponin C
Ca²⁺ binds to Troponin C (TnC) on the thin filament.
Troponin changes shape, moving tropomyosin away from myosin-binding sites on actin.
This exposes the binding sites so myosin heads can attach.
Note: Troponin has 3 subunits:
Subunit | Main Function | Action |
|---|---|---|
TnC | Calcium binding | Triggers conformational change → moves tropomyosin. |
TnI | Inhibition | Blocks actin–myosin binding when Ca²⁺ is low. |
TnT | Tropomyosin binding | Anchors troponin to thin actin filament. |
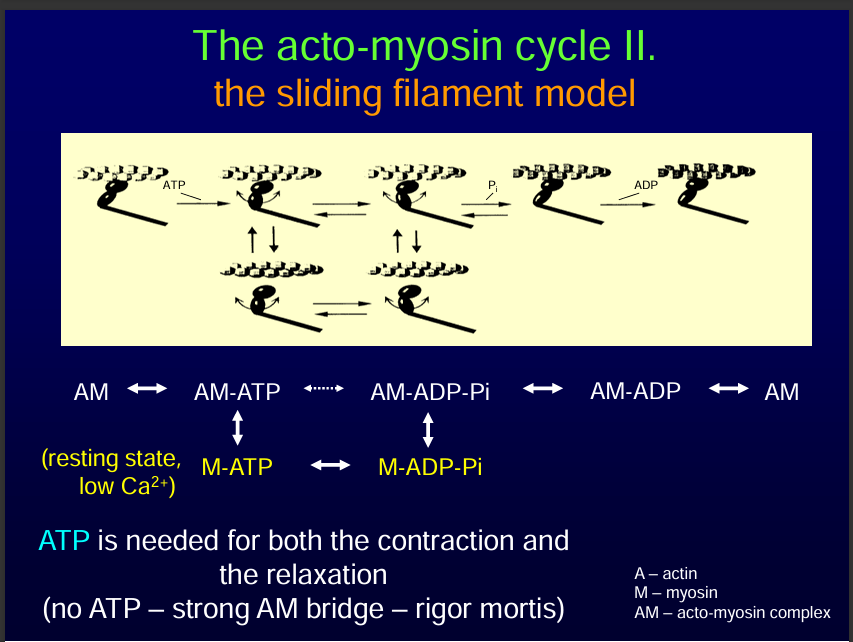
Actin myosin cycle
This is also called Cross-Bridge Formation (Contraction).
Myosin heads bind to actin → forming cross-bridges.
Myosin performs a power stroke:
ADP + Pi is released from myosin.
Actin filament slides toward the center of the sarcomere.
ATP binds to myosin → myosin releases actin.
ATP is hydrolyzed → myosin head is “re-cocked” for another stroke.
This cycle repeats as long as Ca²⁺ and ATP are present → sarcomere shortens → muscle contracts
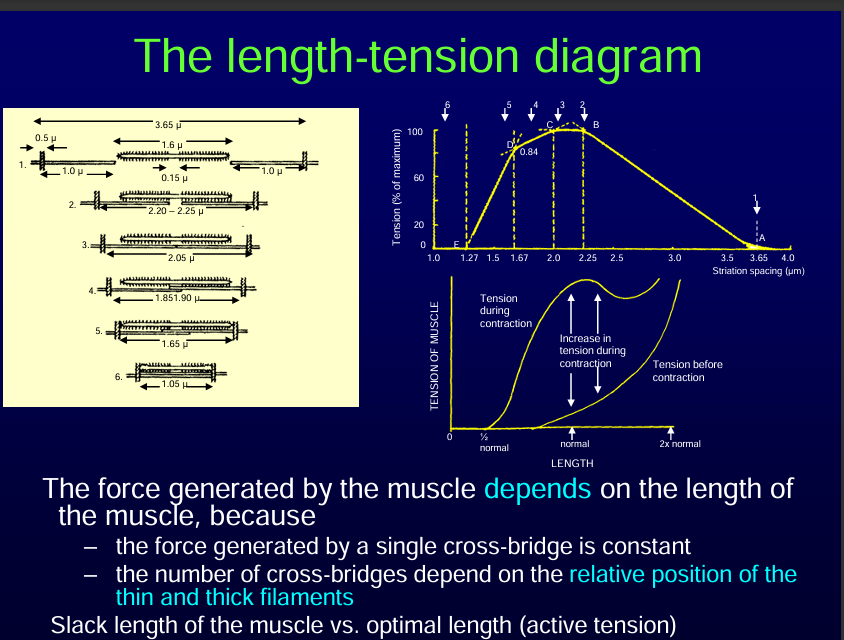
The force generated by the muscle depends on the length of the muscle.
The number of cross bridges determines the strength of the contraction. If there are more cross bridges, the strength of contraction would be stronger.
The number of cross bridges depends in the relative postition of thin and thick filaments.
Maximum tension is between 2.2-2.5 micrometres
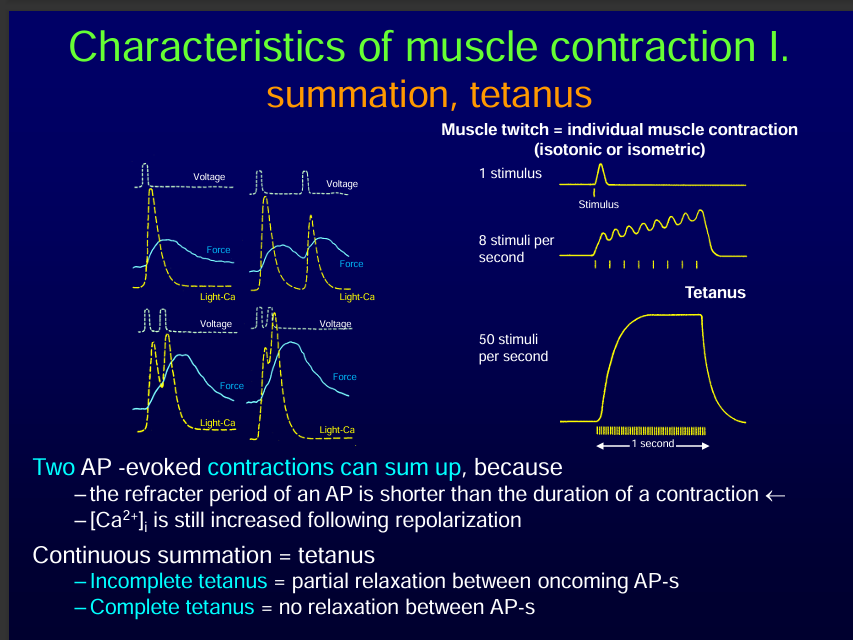
The contraction lasts longer than the refactory period so another AP can start and fuse with the previous one.
Great notes! 👍 Let’s organize and expand them into a clear overview of Characteristics of Muscle Contraction II so it’s easier to study.
Characteristics of Muscle Contraction II
1. Motor Unit
Definition: A motor unit = one motor neuron + all the muscle fibers it innervates.
Within a motor unit, all fibers contract together when the neuron fires.
Contraction is typically tetanic (sustained, maximal force), not single twitches.
Regulation of Force and Precision
Force regulation: Depends on the number of active motor units recruited.
Precision of movement: Depends on the number of fibers per motor unit.
Small motor unit (few fibers) → fine control (e.g. eye, fingers).
Large motor unit (many fibers) → powerful contraction (e.g. quadriceps).
Recruitment: Sequential activation of motor units to increase force.
Fatigue: Prolonged activity reduces the ability to generate force.
Paralysis/Atrophy: Loss of neural input leads to muscle wasting.
2. Elastic Elements in Muscle
Series elastic elements: Tendons and cross-bridges (in line with the contractile elements).
Parallel elastic elements: Connective tissue around fibers (endomysium, perimysium).
Role: They store elastic energy and contribute to smooth, efficient movement.
3. Clinical Conditions
Hypocalcemic Tetany:
Low extracellular Ca²⁺ → increased excitability of nerves → sudden, painful contractions.
Denervation Hypersensitivity:
If nerve supply is lost, nAChRs spread outside the end-plate region, making the muscle overly sensitive to ACh or drugs.
4. Muscle Diseases
Myasthenia Gravis
Autoimmune disease → antibodies attack nAChRs at NMJ.
Leads to muscle weakness, worsens with activity.
Myotonias
Defective relaxation after contraction (ion channel mutations).
Muscular Dystrophies
Progressive degeneration of muscle fibers (e.g., Duchenne dystrophy).
Malignant Hyperthermia
Genetic disorder of RyR calcium channels.
Triggered by certain anesthetics → excessive Ca²⁺ release, hypermetabolism, dangerous rise in body temperature.
Central Core Disease
Congenital myopathy → defects in RyR → muscle weakness and structural abnormalities in fibers.