Contraceptives
1. Explain the menstrual cycle, including hormones involved and key steps in the cycle.
Menstrual Cycle series of hormonal regulated events to prepare the female body for pregnancy starting at 12 years old and lasts for 28- 30 days
Follicular Phase - Days 1-13 where the endometrium is sloughed off and FSH steadily increases until dominant follicle emerges and secretes estrogen to develop the follicle and thicken endometrial lining.
Ovulation phase - Day 13-15 where LH surges from the prolonged estrogen level increase and a high volume, thin, clear mucus, with high elasticity is produced to aid in fertilization if 2 days prior.
Luteal Phase - Day 16-28 when the corpus luteum begins to form and androgens and progesterone levels increase for fertilization. If no fertilization corpus luteum degenerates, progesterone and estrogen levels decrease.
2. Describe the biosynthesis, pharmacokinetics, and physiologic effects of estrogen and progestins.
Estrogen | Progestins | |
biosynthesis | premenopausal women ovaries and placenta as estradiol and estrone and estriol (most to least potent) | premenopausal women in the ovaries and placenta as progesterone |
Pharmacokinetics | plasma-protein binding to sex hormone-binding globulin SHBG or albumin. metabolized by the liver and excreted as urine | protein binding to corticosteroid binding globulin and albumin metabolized by the liver and excreted as urine |
Physiologic effects | helps with the growth and development of the vagina, uterus, fallopian tubes, breasts, axillary and pubic hair. | supressess menstruation produces thick cervical mucus to stop sperm help maintain pregnancy and develop mammary glands |
Metabolic effects | lipids increases TG and HDL decreases TC and LDL alters bile composition in liver increases coagulation factors and decreases anticoagulation factors causes pubertal growth spurt of long bones, decrease activity and number of osteoclasts increases libido causes salt and water retention before menstruation inhibits comedone and acne formation | increases basal and post carb insulin levels stimulates lipoprotein lipases and enhance fact deposition slight increase to LDL and little to no decrease in HDL depressant and hypnotic effects |
3. Define key terms associated with contraception, such as breakthrough bleeding (BTB), spotting, amenorrhea, withdrawal bleeding, back-up method, perfect use.
Breakthrough bleeding (BTB): Bleeding during active pills requiring a pad/tampon.
Spotting: Less bleeding than menses, not requiring a pad/tampon.
Amenorrhea: Absence of menses.
Withdrawal bleeding: Bleeding due to hormone withdrawal in a medication
Back-up method: Additional contraception (condom, spermicide, diaphragm).
Perfect use: Correct and consistent use of contraception.
Typical use: actual inconsistent and incorrect use of contraceptive
4. Describe the indication, physical assessment, and treatment goals to consider with the use of contraception.
Indications: Assessing interest, reproductive knowledge, and potential need for a pregnancy test.
Reasonably certain a woman is not pregnant based on:
lack of sexual intercourse since start of last menses,
7 days or less than start of normal menes,
within 4 weeks postpartum
perfect use of contraception,
nearly (85%) or fully breastfeeding, amenorrheic and less than 6 months postpartum
Physical assessment: Blood pressure (less than 160/110 mmHg), absence of vascular disease safe for hormonal contraceptives.
If BP greater than 140/90 refer to PCP for further info.
Treatment goals: Preventing pregnancy by inhibiting sperm-ovum contact or preventing implantation. Additional goals include managing premenstrual dysphoric disorder (PMDD), improved dysmenorrhea, menstrual cycle regularity, decreased acne, manage endometriosis and polycystic ovarian syndrome.
5. Explain the nonpharmacologic and pharmacologic therapies.
Non-pharmacologic: Abstinence, periodic abstinence (natural family planning or ovulation method), spermicides, barrier methods (condoms, diaphragm, cervical cap).
Pharmacologic: Combined hormonal contraception (oral, transdermal, vaginal), progestin-only contraception (pills, injectables, implants, intrauterine devices).
6. For each class of medication, explain the mechanism of action, relevant pharmacokinetic/pharmacodynamic parameters, relevant pharmacology, formulation, contraindications/precautions, common and serious ADRs, common DDIs, and monitoring parameters.
Combined Hormonal Contraceptives
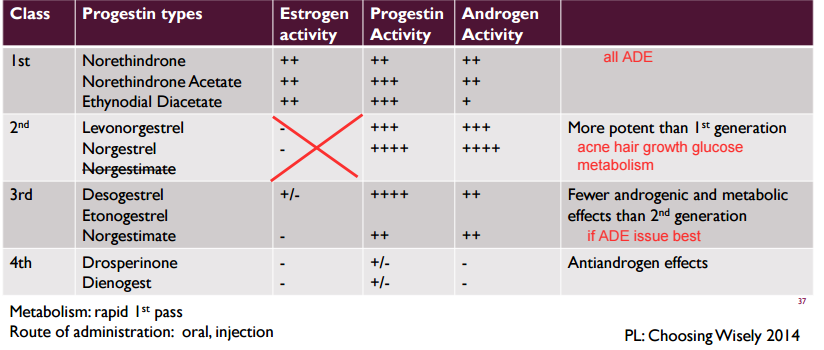
MOA: Estrogens suppress FSH and prevent development of dominant follicle as well as stabilize endometrial lining for bleeding control.
MOA: Progestins decrease GnRH to decrease LH and FSH, thicken cervical mucus to stop sperm , slow tubal motility, delay sperm transport, alter endometrial lining to inhibit implantation.
Pharmacokinetics: both metabolised by CYP3A4 and by first pass hepatic and excreted as urine
Formulations: Oral, patch, vaginal ring.
Contraindications
Known or suspected pregnancy
breastfeeding women < 6 weeks postpartum
current breast cancer
35+ age and heavy smoker 15+ cigs a day
uncontrolled HTN > 160/100 mmHg
acute or history of DVT/PE with high risk of recurrence, thrombogenic mutations
major surgery with prolonged immobilization
migraines with aura
migraines without aura for 35+ age
multiple risk factors for CV disease like old age, smoking, diabetes, HTN
diabetes with vascular or microvascular complications
diabetes for 20+ years
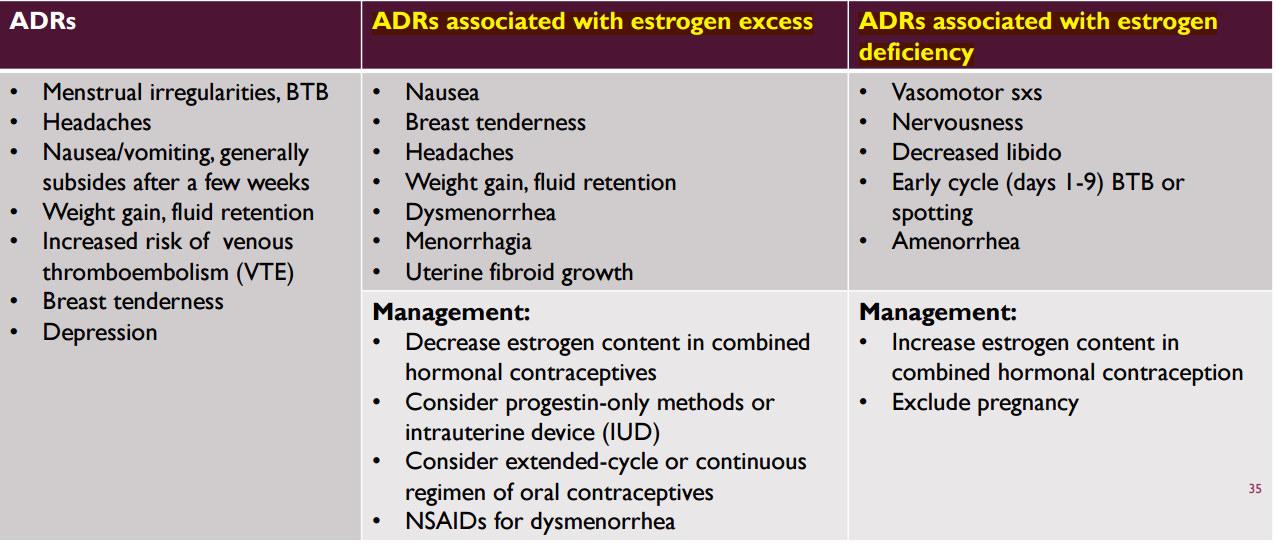
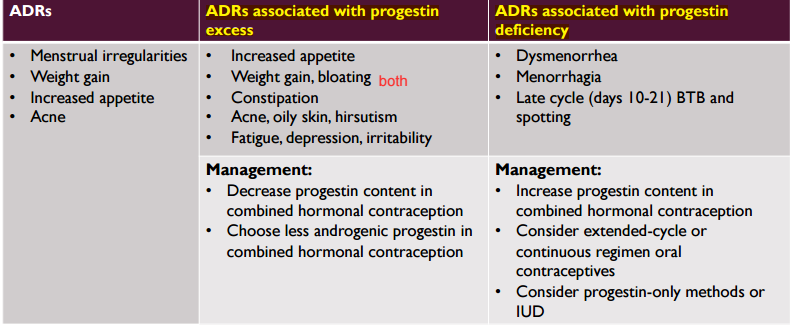
Serious ADRs: Described using the acronym ACHES
Abdominal pain, Chest pain, Headaches, Eye problems, Severe leg pain
if any stop contraceptive and seek medical help.
DDIs:
CYP3A4 inducers (PS PORCS) decrease efficacy by increasing liver clearance causing BTB or spotting.
CYP3A4 inhibitors (G ❤ PACMAN) increase efficacy by decrease liver metabolism
antibiotics decrease CHC efficacy by reducing bacteria and gut metabolism causing BTB or spotting may need back up
lamotrigine can increase or decrease levels with CHC changing seizure control
warfarin can increase or decrease levels with CHC should monitor INR for risk of thrombosis and bleeding
theophylline can decrease levels with CHC changing respiratory control
cyclosporine can increase levels with CHC should monitor the concentration of cyclosporine and signs and symptoms of renal and hepatic cyclosporine
Combined Oral Contraceptives
Monophasic - same amount of estrogen and progestin in 21 or 28 day of active pills with 7 days of placebo
Multiphasic - contains variable amounts of estrogen and progestin for 21 days then 7 days of placebo for a lower total monthly dose of progestin
Biphasic - Azurette white 21d combo, light-green 2d placebo, light blue 5d estrogen only
Triphasic - Tri-Lo-Marzia - white 7d combo, light blue 7d combo, blue 7 day combo, doses of estrogen and progestin varies between days
Quadphasic - Natazia dark yellow 2d estrogen, medium red 5d combo, light yellow 17d combo, dark red 2d estrogen, white 2 day placebo,
Extended Cycle - Seasonale and Jolessa contains 84d of active tablets then 7 days of placebo to produce 4 cycles a year
may cause more BTB or spotting
better for anemic, dysmenorrhea, menorrhagia, endometriosis conditions
Continuous cycle - Lybrel or Amethyst that has no placebo tables at all
higher BTB and spotting from higher estrogen/progestin exposure
long term effects unknown
may be hard to determine pregnancy since irregular periods
Shortened Hormone Free Interval - Lo Loestrin-24 Fe,Beyaz,Yaz
contains 21-24 days of active tablets
shorten menses and decrease hormone withdrawal side effects
better for patients with dysmenorrhea or heavy menstrual cycles
Drospirenone and Ethinyl Estradiol
less antimineralocorticoid and antialdosterone activity
increased risk of blood clots 74% compared to other low-dose oral contraceptives
examples of Yasmin,Yaz,Beyaz
Minastrin 24 Fe and Lo Minastrin Fe
chewable tablet formulation with same hormonal levels as Loestrin
need doctor approval to substitute
COC- starting contraception
day 1 of menstrual flow no backup but more rapid contraceptive effects
first sunday start need backup contraceptive for 7 days, but maybe no bleeding on weekends
Immediate starting regardless of menstruation need backup for 7 days
COC - missed doses
1 active pill - take ASAP even if 2 same day no backup
2 consecutive - take last missed pill and discard other missed even if means starting new pack along with backup for 7 days
3+ consecutive - consult package insert
Combined Transdermal Patch
Norelgestromin and EE aka Xulane
provides slow sustained hormone release causing constant blood levels
increased risk for VTE from higher estrogen then CHC
best for women with menstrual migraines
avoid in women weighing 90+ kg
ADR: same as COC (weight gain, menstrual irregularities, breast tenderness) along with skin irritation resolved by site rotation or anti-inflammatory products
Patient Counseling:
start after 5 days of menses onset for no backup
start other days use backup for 7 days
apply 1 patch a week for 3 weeks then remove for 1 along with 5 days backup each first week
do not cut it and no need to remove for bathing, swimming, exercise
Missed Dose:
less than 24 hrs apply new patch and no backup
24+ or unsure apply new patch and restart cycle with 7 days backup
Combined Vaginal Ring
Etonogestrel and EE aka Nuvaring
for 28 days releases 15 mcg of EE and 120 mcg of Etonogestrel a day for 3 weeks
ADR: same as COC along with higher thromboembolic risk, decreased nausea headache breast tenderness, increased risk for less libido. ring specific being foreign body sensation, device expulsion, vaginal symptoms
Patient counseling
start on or before 5th day of menstrual cycle for no backup
start other days 7 days backup
may be placed anywhere in vagina for 3 weeks then removed for 1 week
bleeding in first 2-3 days of ring removal.
discard foil in pouch not down toilet
Missed Dose:
less than 3 hours rinse ring with warm water reinsert with no backup.
more than 3 hours rinse with warm water and reinsert with 7 days backup.
Progestin Only
Micronor aka Errin
norethindrone containing best for those intolerant or contraindicated to estrogen products
Patient Counseling
no adverse effect on lactation
less effective than COC
higher incidence of ectopic pregnancy
ADR
irregular menses
decreased duration and amount of menstrual flow
spotting amenorrhea
Norgestrel
Opill OTC
Patient Counseling
no adverse effect on lactation
less effective than COC
higher incidence of ectopic pregnancy
Progestin Only Pill Patient Counsel
must be taken at same time daily or lower efficacy
must start on Day 1 otherwise backup for 2 days after start
less than 3 hr missed dose take pill ASAP no backup
more than 3hr missed dose take pill ASAP with 2 days backup (EC)
DPMA
best for breastfeeding, estrogen intolerant, medical condition preventing estrogen
Contraindicated for current diagnosis of breast cancer
ADR
BBW for decreased bone mineral density
menstrual irregularities (spotting, prolonged bleeding, amenorrhea)
significant weight gain of 5 lbs in first year
breast tenderness
depression
acne
hirsutism
Start every 3 months within 7 days of onset of menstrual bleeding
if administered after 7 days backup contraception
Nexplanon
long acting reversible contraceptive (LARC) rod that lasts up to 3 years
not for overweight or obese women
ADR
irregular menstrual bleeding first 6-12 months
longer heavier periods with spotting
headache
mood changes
acne
weight gain
DDI with CYP450 inducers (PS PORCS)
surgically start within first 5 days of menstrual cycle in women with no previous contraceptives
backup for 7 days if any other day
removed and replaced every 3 years
Intrauterine Device (IUD) LARC
MOA:
inhibit sperm migration
damage ovum or stop transport
endometrial suppression and thickening of cervical mucus (levonorgestrel)
Types
Copper Paragard - replaced every 10 years and no DDI
Mirena/Kyleena/Liletta - replaced every 5 years and small amounts of levonorgestrel
Skyla - replaced every 3 years and smallest amounts of levonorgestrel
Insert by a trained clinician
start first 7 days of menses
7 days backup if after first week
Contraindications
current pelvic inflammatory disease (PID) or STD
undiagnosed abnormal vaginal bleeding
malignancy of genital tract
allergy to IUD or Wilson’s disease for Copper
Early danger Signs (PAINS)
Period Late (pregnancy abnormal spotting or bleeding)
Abdominal pain or pain with intercourse
Infection exposure or abnormal vaginal discharge
Not feeling well with fever or chills
String missing, shorter, or longer
ADRs
risk of PID first 20 days after insertion
vaginal inflammation
ovarian cysts
acne
headache
Return to Fertility
Hormonal Contraceptive | Return to Fertility |
progestin only | immediate |
CHC | 1-2 weeks after stopping |
IUD | 30 days from removal |
nexplanon | 6 weeks |
injectable | 10 months |
Emergency Contraceptive
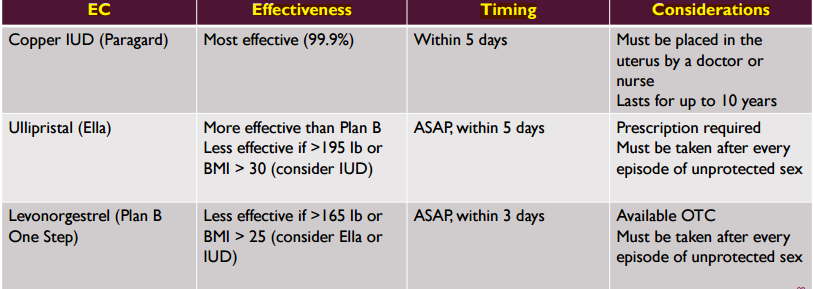
7. For each specified medication, recall brand/generic names, dosage forms, and when backup
Type | Brand | Generic | timing and Form | When backup |
Combined Oral Contraceptive | Azurette | Desogestrel and EE | biphasic tablets | 7 days if 2+ pills missed or if missed pills in week 1 immediate start |
Combined Oral Contraceptive | Tri-Lo Marzia | Norgestimate and EE | triphasic tablets | 7 days if 2+ pills missed or if missed pills in week 1 immediate start |
Combined Oral Contraceptive | Natazia | Dienogest and valerate estradiol | quadphasic tablets | 7 days if 2+ pills missed or if missed pills in week 1 immediate start |
Combined Oral Contraceptive | Seasonale or Jolessa | Levonorgestrel and EE | extended cycle tablets | 7 days if 2+ pills missed or if missed pills in week 1 immediate start |
Combined Oral Contraceptive | Lybrel or Amethyst | Levonorgestrel and EE | continuous cycle tablets | 7 days if 2+ pills missed or if missed pills in week 1 immediate start |
Combined Oral Contraceptive | Lo Loestrin-24 Fe or Beyaz or Yaz | Drospirenone and EE and levomefolate | shortened hormone free interval tablets | 7 days if 2+ pills missed or if missed pills in week 1 immediate start |
Combined Oral Contraceptive | Minastrin 24 Fe and Lo Minastrin Fe | Drospirenone and EE and levomefolate | shortened hormone free interval chewable | 7 days if 2+ pills missed or if missed pills in week 1 immediate start |
Combined Transdermal Patch | Xulane | Norelgestromin and EE | 21 days total rotate weekly 7 days patch free | 7 days if no patch for 24 hours starting before 5 days from onset of menses |
Combined Vaginal Ring | Nuvaring | Etonogestrel and EE | 21 day active total 7 days ring free | 7 days backup if 3+ hours missed dose inserted after 5th day of cycle |
Progestin Only | Micronor | Errin | 0.35 mg of norethindrone daily pill with no breaks | 2 days if missed dose for 3+ hours or not Day 1 start |
Progestin Only | Opill | Norgestrel | 0.0075 mg daily of Norgestrel with no pill breaks OTC | 2 days if missed dose for 3+ hours not Day 1 start |
Progestin Only | Depo-Provera DPMA | Depot Medroxyprogesterone Acetate | IM or SC injected every 3 months | 7 days if after 7 days of onset menstrual bleeding |
Progestin Only | Nexplanon | Etonogestrel | LARC rod that lasts for 3 years | 7 days backup if inserted after day 5 in menstrual cycle |
Progestin Only | Mirena/Liletta/Kyleena skyla | levonorgestrel | LARC IUD that lasts for 5 or 3 years | 7+ days since start of menes |
copper | Paragard | Copper | IUD | cant miss |
8. Given a patient case, develop appropriate, evidenced-based non-pharmacologic and pharmacologic treatment recommendations.
above tables
9. Provide thorough patient counseling for hormonal contraceptives, including initiation, administration, missed doses, adverse effects of hormonal contraceptives.
above tables