2027 notes
Ataxia
Learning outcomes
- outline the pathophysiology, prognosis and general management of conditions with cerebellar ataxia
- Use the ICF framework to organise and prioritise problems, and set patient-centered goals for people with cerebellar ataxia
- design appropriate assessment and treatment plans for people with cerebellar ataxia based on clinical reasoning and research evidence
Summary
- Ataxia is the loss of coordination NOT due to muscle weakness
- Pathophysiology and prognosis of ataxia depends on the cause of damage on the cerebellum
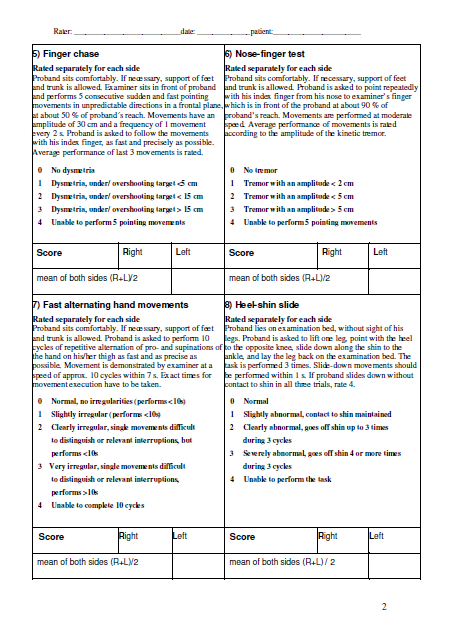
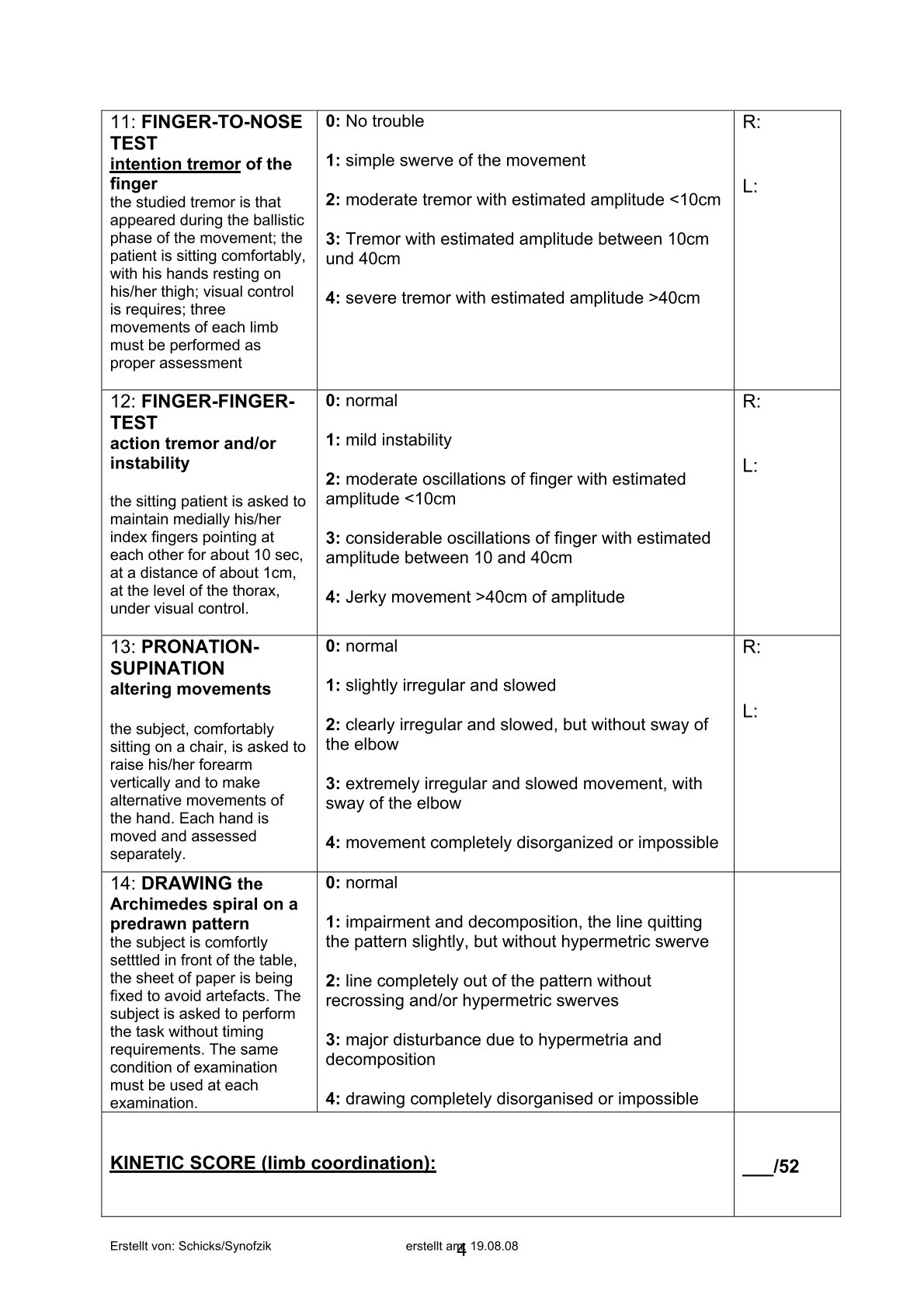
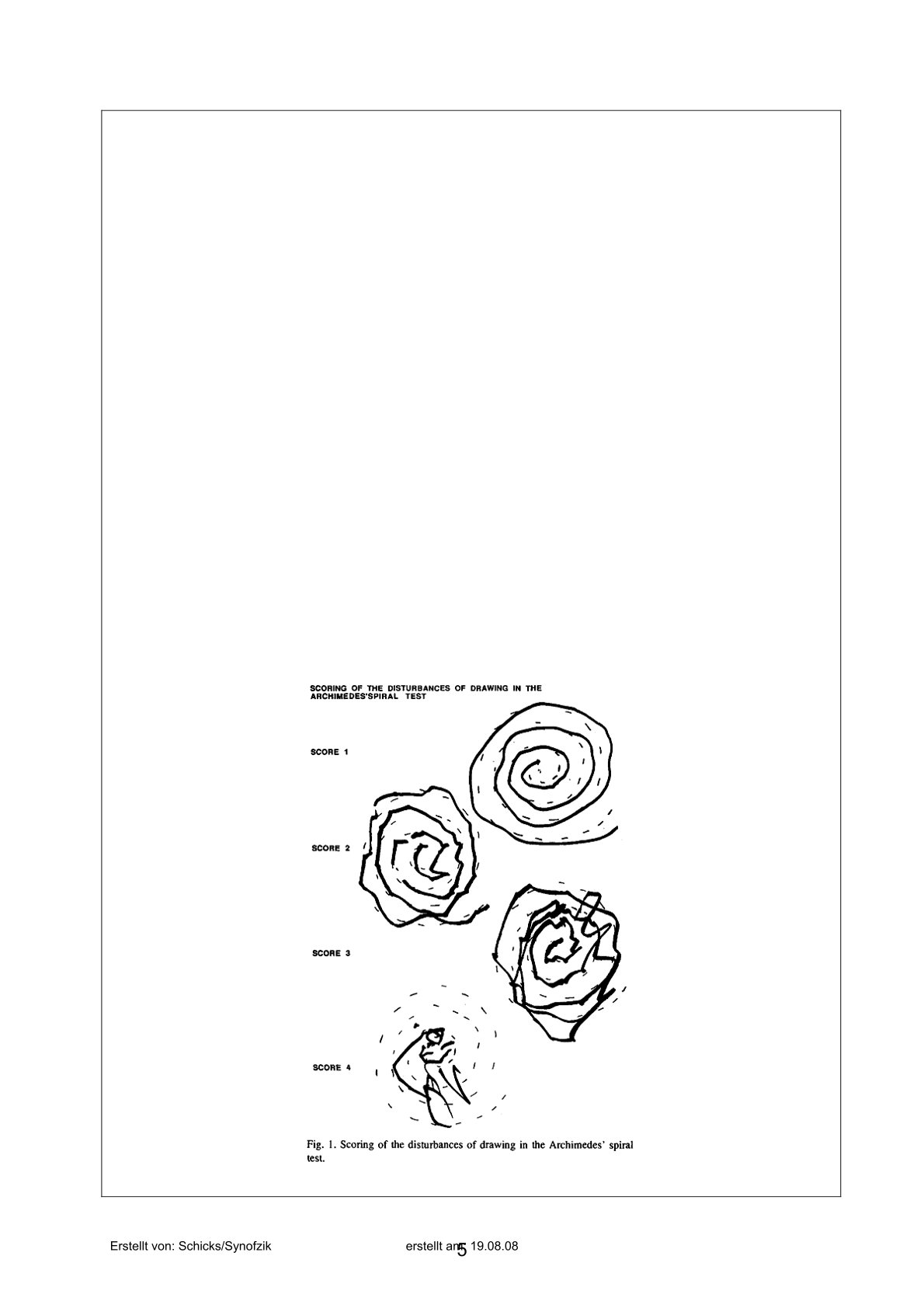
- Assessment: focus on these tests: finger-to-nose test, forearm supination-pronation test, rebound test, heel-to-shin test, berg balance scale
- Treatment: focus on restorative approaches (internal cues, balance, eye and muscle strength…), or else it is compensatory (external cues or equipment) or both
Definition
Ataxia: clumsiness or lack of balance or coordination that is not due to muscle weakness. (lack of coordination)
- We need strength and coordination to work together to perform an action
- If there is damage at the cerebellum, we must assess coordination first
Role of cerebellum
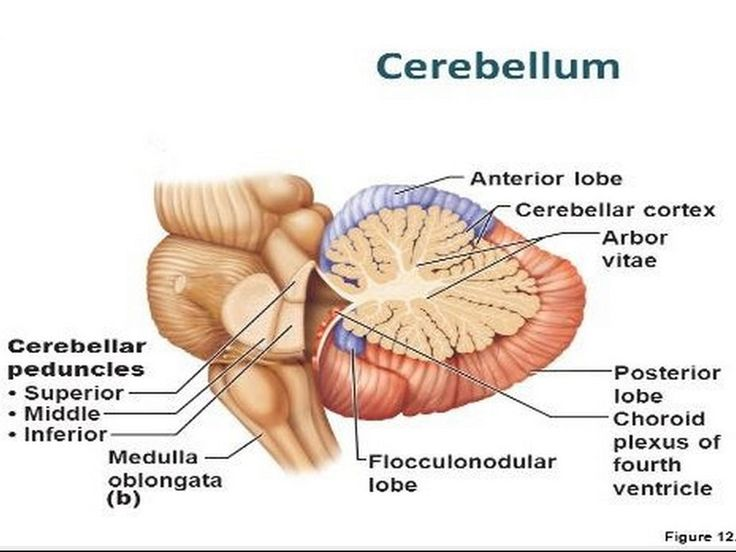
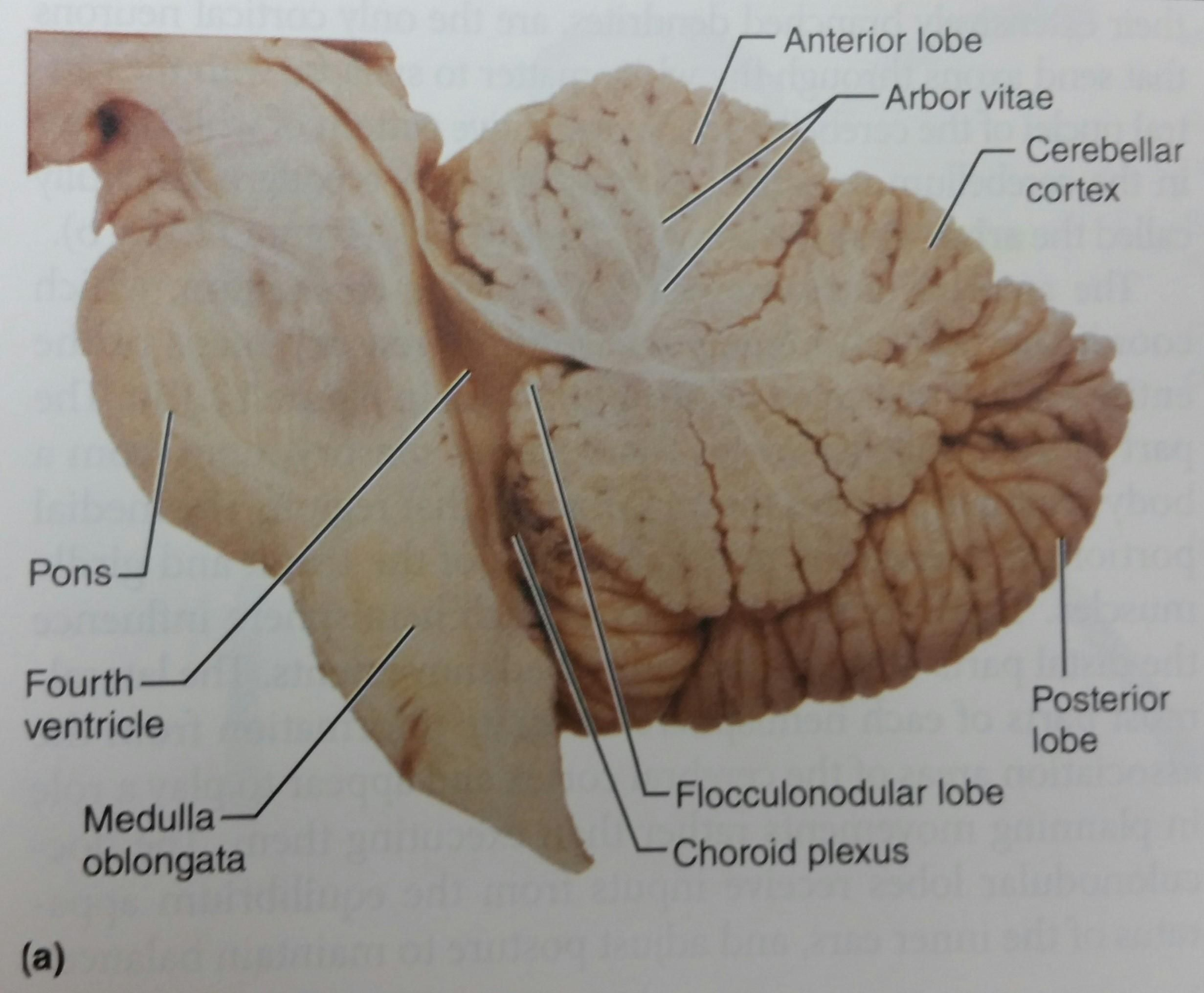
Function
- Coordinates muscles and balance during activity and walking
- The cerebellum detects any change in balance and movements, sends signals to the brain to adjust itself
- Needs to time the movement of the muscles to achieve a smooth action, otherwise, it would be haphazard
- Note the components of coordination
- Amplitude
- Speed (how fast)/timing (sequencing)
- Force
- Direction
- Controls eye movements, speech and swallowing
- Motor learning via practice and fine tuning
- Higher level processing such as language and emotions
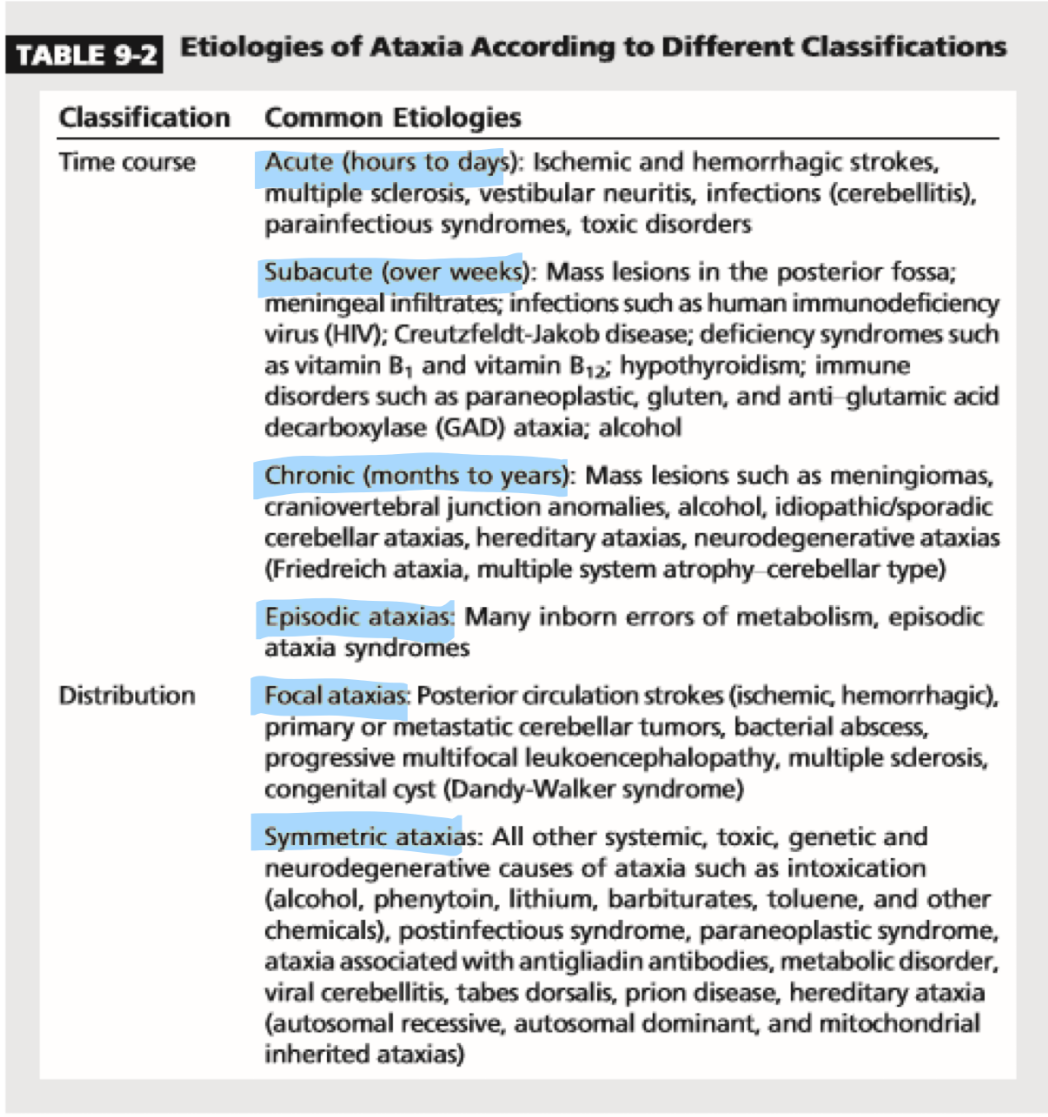
Classification of ataxia
- Acquired
- Due to external causes due to an event or a condition
- Acute (have a chance at recovery) or progressive/degenerative
- Examples: stroke, head trauma, tumour/cancer, multiple sclerosis, substance abuse
- Genetic
- Contains DNA that led to ataxia
- Often progressive/degenerative
- Examples: Friedreich's Ataxia, spinocerebellar ataxia
- Friedreich’s: damages the peripheral nerves, spinal cord and cerebellum
- SCA: family history (requires DNA testing)
- Idiopathic
- Unknown causes
- Example: multiple system atrophy
Specific causes and their presentations
- Stroke
- Occurs in the brainstem or cerebellum. Ischemia.
- Stroke in the cerebellum vs stroke in the cerebrum has two different presentations as ataxic stroke may not present with the classical signs of slurred speech, hemiparesis, or arm drift.
- Tests
- Finger-to-nose: hold your index finger at arm’s length and tell them to touch their nose and reach out to touch your fingertip
- will have incoordination, struggle with
- Heel-to-shin: lift each leg separately and slide heel along the opposite shin
- difficulty completing
- Finger-to-nose: hold your index finger at arm’s length and tell them to touch their nose and reach out to touch your fingertip
- Spinocerebellar ataxia
- Rare inherited neurodegenerative heterogeneous autosomal dominant disease that mainly affects the cerebellum, hence a subset of inherited ataxia
- Peripheral nerves, spinal cord and cerebellum are damaged
- Needs wheelchair within 10-20 years of diagnosis
- Friedreich’s ataxia
- Rare inherited neurodegenerative gene
- Lifespan is usually short but some live up to 50-60s
- Video
- Wide base of support
- Unsustained horizontal nystagmus
- Bilateral foot drop
- Bilateral pes cavus (high arch)
- Rapid hand opening-closing and finger tapping are slow but not ataxic
- Supination-pronation of forearm is mildly ataxic
- Finger-to-nose test shows mild ataxia as she approaches the target
- Multiple system atrophy
- Rare condition of the nervous system where there is gradual degeneration of the nerve cells in the brain -> impairment at the level of balance, movement and autonomic nervous system which controls basic functions such as breathing, digestion and bladder control
- Lifespan is 7-10 years after first symptoms but the lifespan varies widely
- Usually the death is not due to MSA but the secondary effects of the disease such as infection, blood clots in the lungs/embolism, or respiratory problems
- Example: Type C
- Facial masking increased
- When holding arms out, they tend to drift further than before
- Finger-to-nose progressed from unilateral to bilateral
- Gait is more unsteady, requiring more assistance to walk
Pathophysiology of ataxia
- Ataxic presentations differ based on the cerebellum lesions locations
- Focal lesions follow the table
- Diffused lesions where there are lesions at more than one site, there will be generalised symptoms
- For vermis, there will be truncal ataxia, sparing of limbs, vertigo
- For vestibulocerebellar, there will be gait ataxia, imbalance, vertigo
- For lateral cerebellum hemisphere, there will be ipsilateral incoordination
- Ataxia involves the cerebellum, its afferent or efferent pathways, vestibular system and proprioceptive pathways
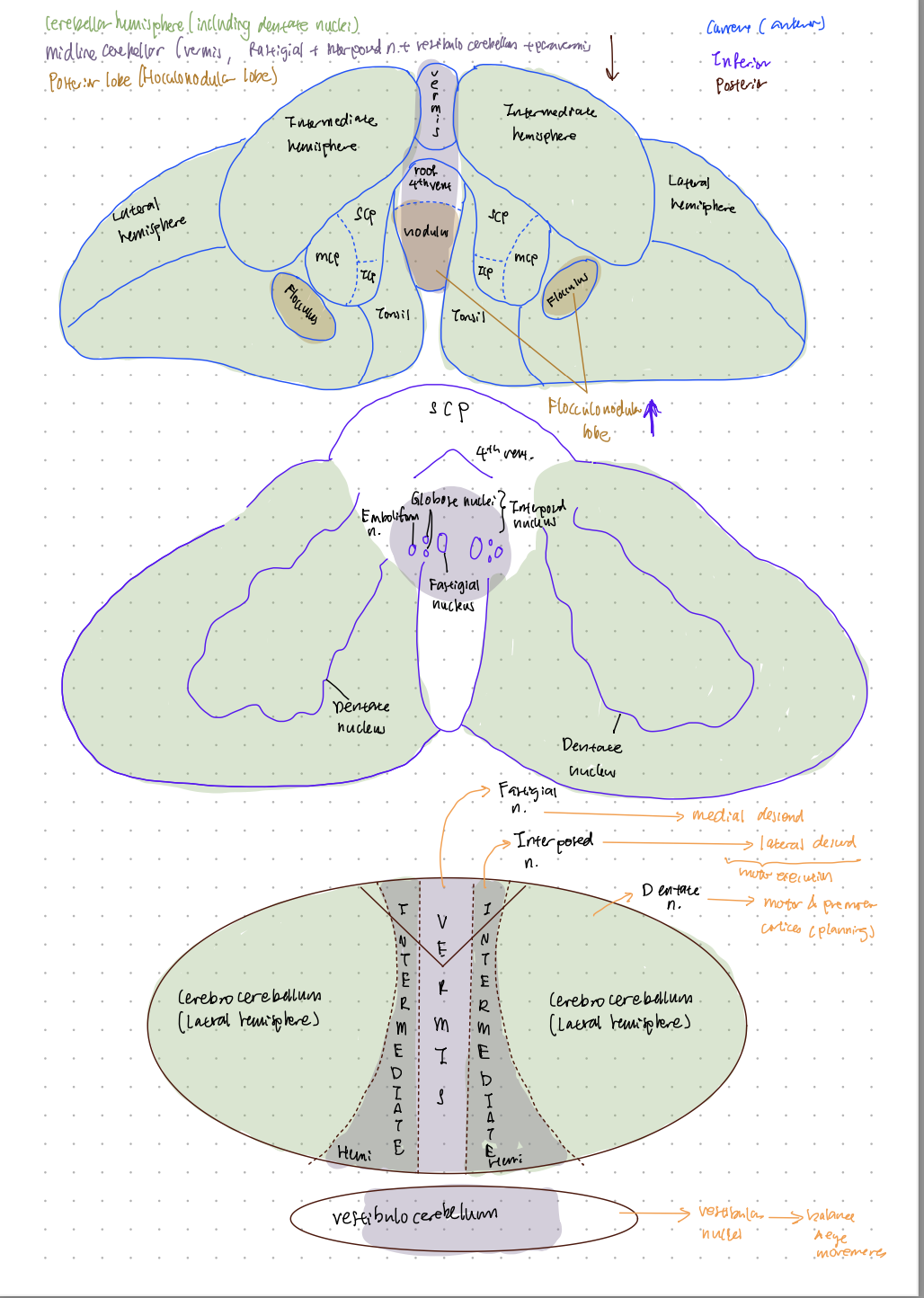
Type | Neuroanatomy | Function | Ataxia or ataxic presentation |
|---|---|---|---|
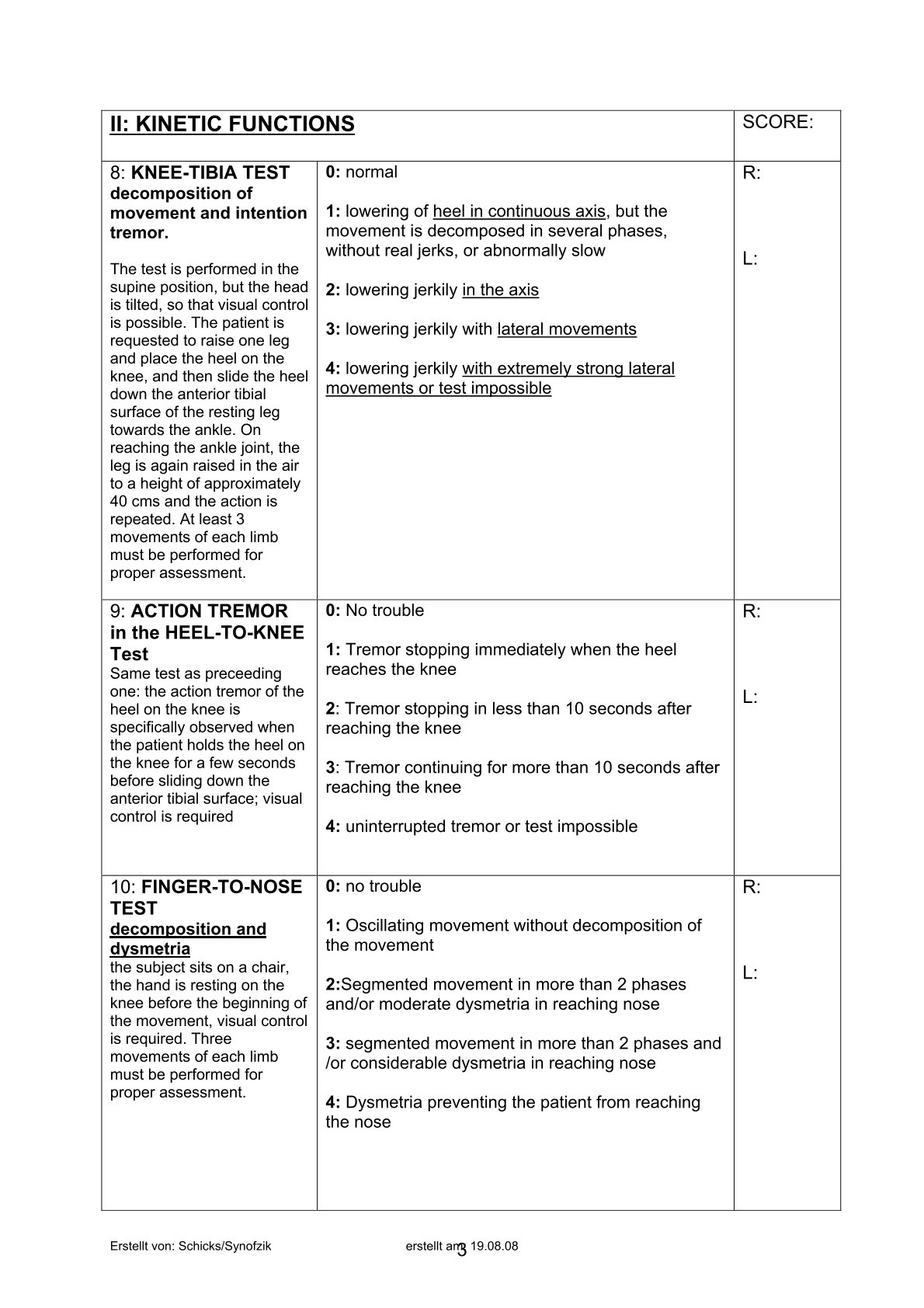
Cerebellar | Cerebellar hemisphere, including the dentate nuclei | Integration of sensory information and motor planning to perform a complex task | Ipsilateral limb ataxia (upper limb) Dysarthria (scanning speech) Dysdiadochokinesia Dysmetria Intention tremor (of the PROXIMAL limb) (essential=distal) |
Midline cerebellar (vermis which includes fastigial nuclei, paravermis which includes the interposed nuclei, vestibulocerebellar) | Motor execution Balance Lower extremity coordination Rapid and slow eye movements Vestibular function | Truncal ataxia (can be made more apparent when asked to hold their arms in front or stand still) Gait ataxia with imbalance (if removing visual cues makes it worse, refer to sensory ataxia instead) Dysmetria Ocular findings Head bobbing Vertigo | |
Posterior lobe (flocculonodular lobe) | Integration of information from the vestibular nuclei | Nystagmus Postural instability Gait ataxia | |
Frontal lobe of the cerebral cortex | Planning and initiating gait | Frontal ataxia (Bruns) Magnetic gait (shuffling of feet, not lifting them off the ground)
| |
MSK (gluteal muscles) | Stabilising the hip during weight bearing | Waddling gait rather than ataxia
| |
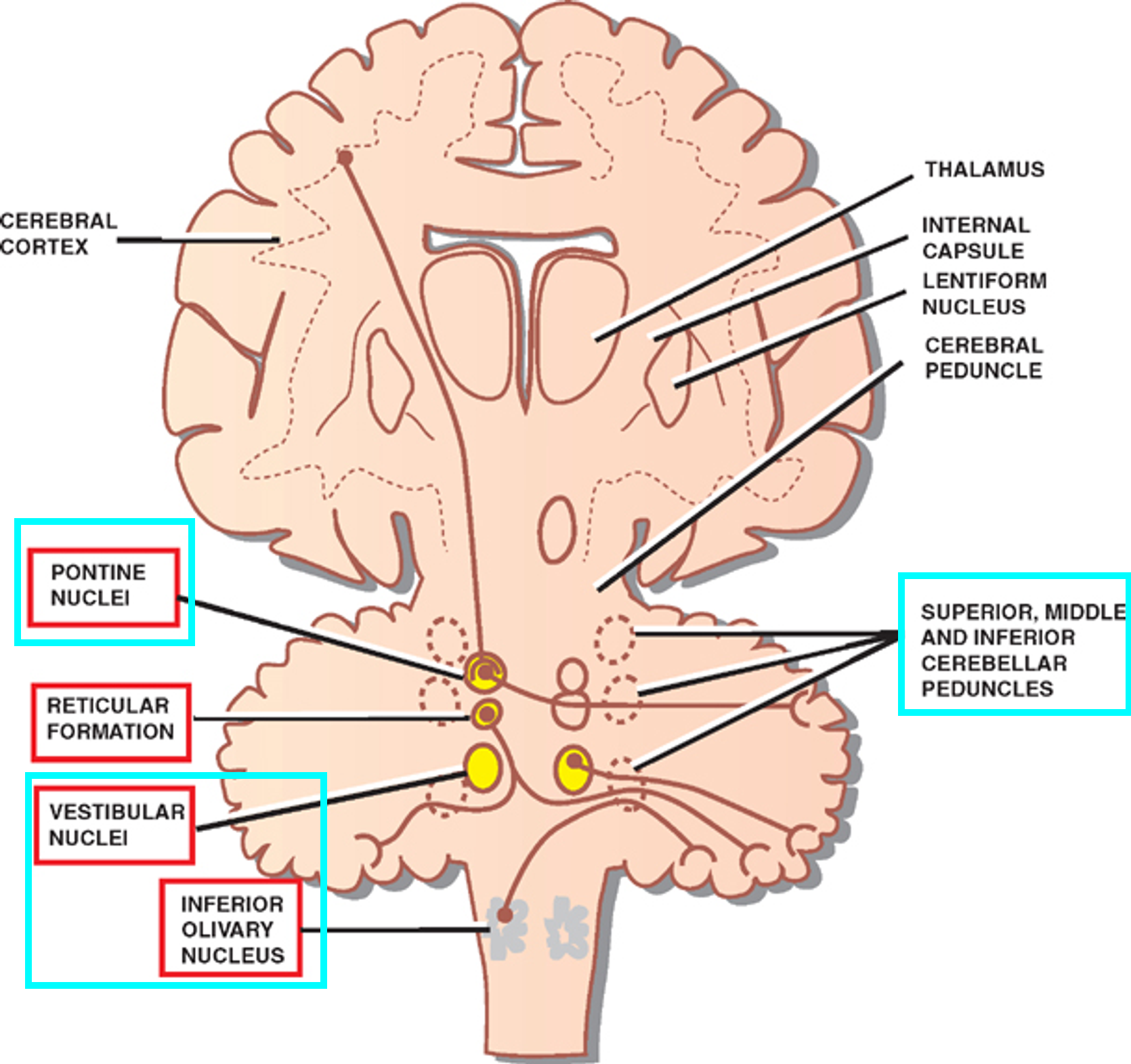
Brainstem (vestibular nuclei, inferior olivary nuclei, pontine nuclei, cerebellar peduncles) | Transmits information to and fro the cerebellum | Ataxia associated with cranial nerve dysfunction and motor-sensory deficits | |
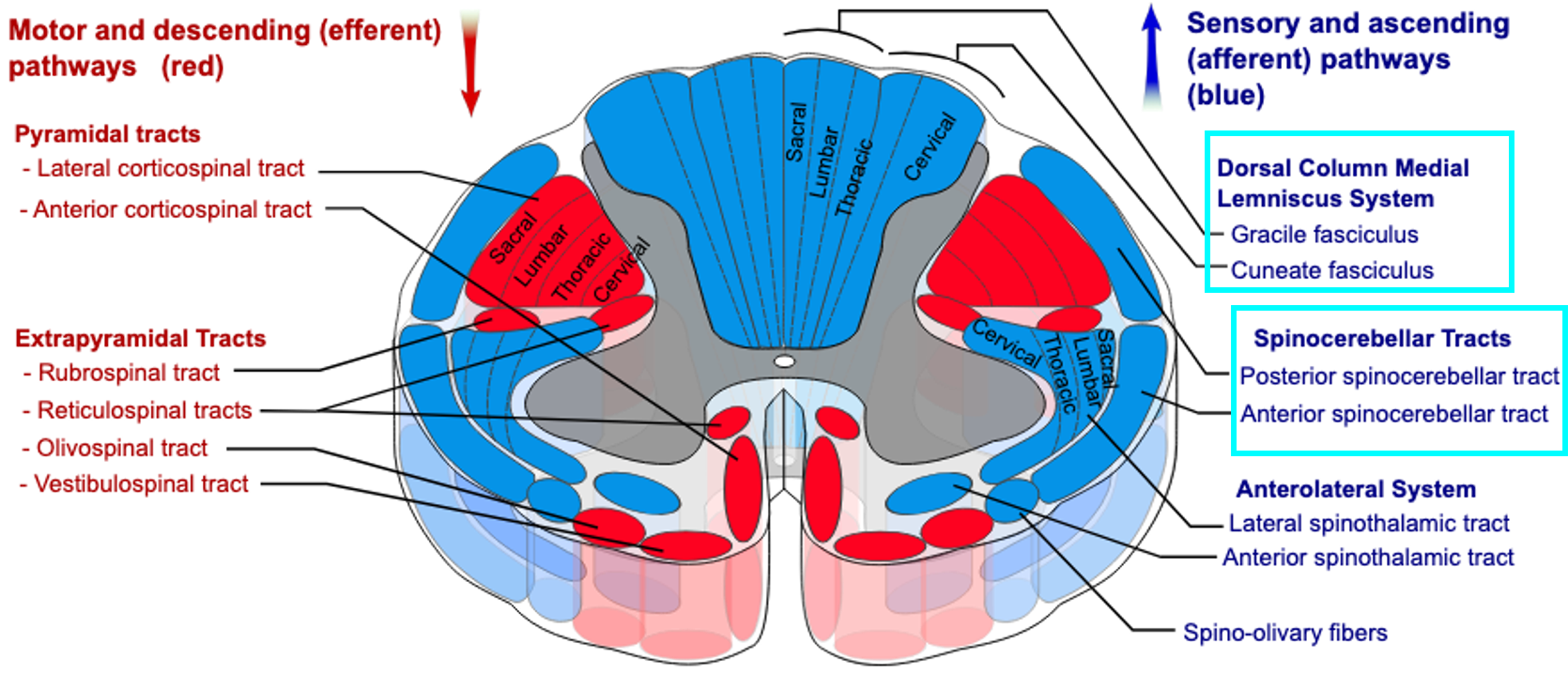
Sensory | Spinal cord (gracile and cuneate fasiculus, spinocerebellar tract/mossy fibres) | Sensory pathway conduction | Sensory ataxia |
Sensory | Proprioceptive system and visual system | Proprioception and visual input | Sensory ataxia with Romberg’s sign (unable to stand still when eyes are closed and feet are together)
|
Vestibular | Vestibular system (vestibular nerve, vestibular nuclei, labyrinth of the inner ear) | Sense of balance and spatial orientation Equilibrium | Imbalance associated with vertigo and dizziness Disequilibrium Tinnitus and hearing impairments Vertigo Nystagmus |
Prognosis of ataxia
- Hereditary: usually a shorter lifespan, and if severe enough, life ends in childhood or early years
- Progressive: symptoms worsen over time -> symptomatic treatment first
- Acquired: find the underlying cause -> remove the triggers for better prognosis
Impairments in ataxia (ICF)
Elements of coordination
- Amplitude
- Speed (how fast) / timing (sequence of action)
- Direction
- Force
Usually the symptoms will appear ipsilateral to the cerebellar lesion
- Example: Wallenburg syndrome/lateral medullary syndrome/posterior inferior cerebellar artery syndrome
- Occurs when the vertebral artery or the posterior inferior cerebral artery is occluded -> infarction of lateral medulla
- Typical presentation: motor, sensory, cognitive, speech and language deficits
- Other presentations that rely on specific nuclei and fibres: vertigo, nausea, imbalance, sitting/postural instability, blurry vision, horizontal and/or rotational nystagmus, crossed hemisensory disturbance, reduction of ipsilateral facial pain, contralateral reduction in trunk pain and temperature sensation, temperature sensation deficits
Problems:
- Dysmetria
- Difficulty in achieving the desired amplitude/distance
- Hypermetria: overshoot
- Finger-to-nose test: press into the target as they cannot stop themselves in time
- Eyes correcting overshoot to focus on the object
- Large amplitude square wave jerks (1 saccade to the right, pause, 1 saccade to the left) are more specific to cerebellar ataxia
- Ocular flutter (same as square wave but no pause) and opsoclonus (continuous and chaotic) -> cerebellar disease from paraneoplastic (neuroblastoma) or post-infectious syndromes
- Hypometria: undershoot
- Finger-to-nose test: pauses before the target and sometimes tries to reach further
- Eyes taking a second to move to catch the object
- You can have both hypermetria and hypometria
- Dyssynergia
- Incoordination of agonist, antagonist, and other synergistic muscles across a multi-joint system when performing a smooth action
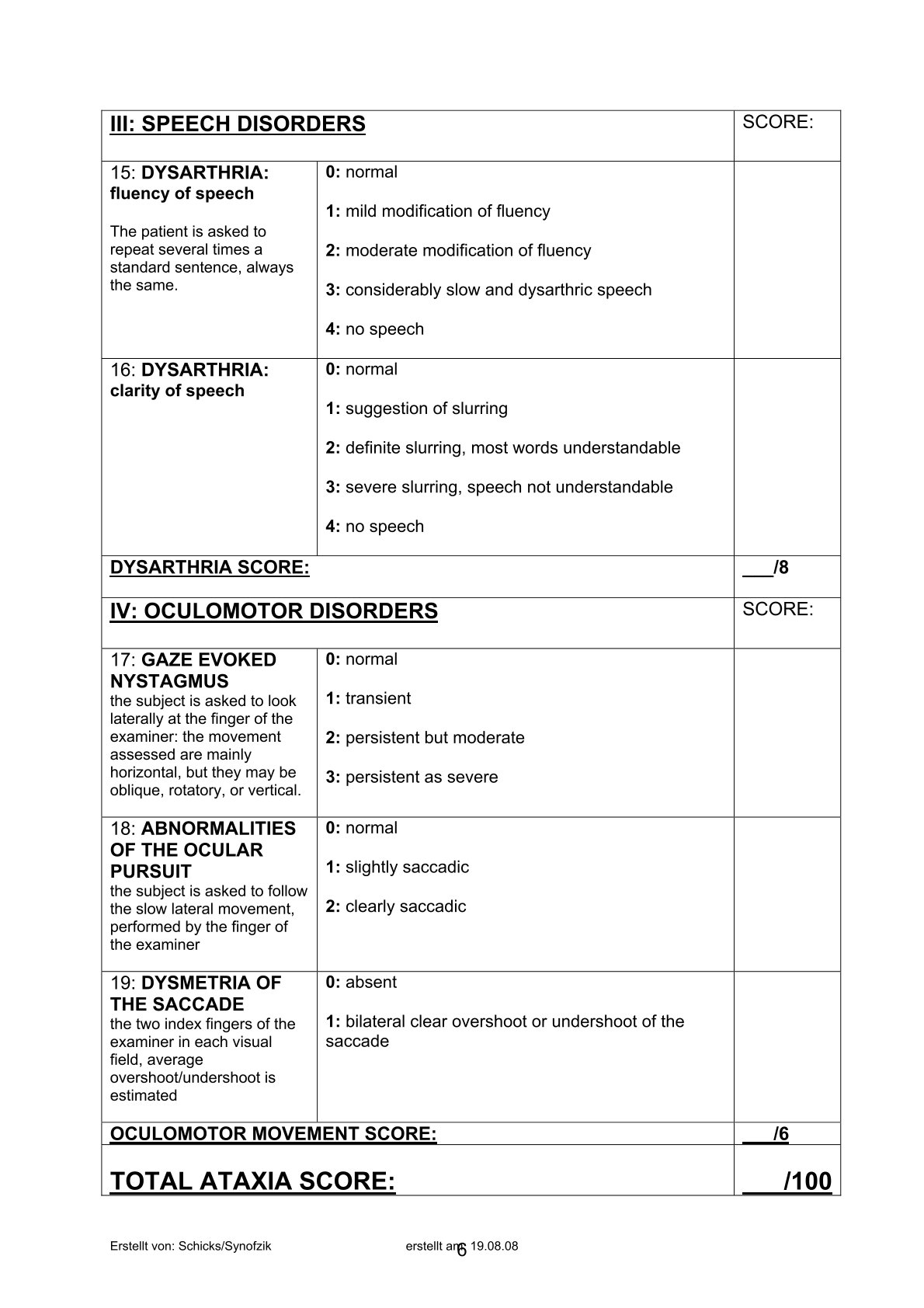
- Dysarthria/scanning speech
- Difficulty in pronunciation and articulation of speech due to the muscles involved in speaking are not sequenced
- Dysdiadochokinesia
- Difficulty in performing rapid alternating movements
- Rebound phenomenon
- Difficulty regulating the force between an agonist and an antagonist (lack of check)
- Normal: When resistance against the elbow flexion is suddenly removed, the limb will continue a short distance in the original direction of movement -> antagonist contracts after reaction time -> limb moves back in opposite direction
- Ataxia: complete absence of this phenomena -> large distance by limb in original direction
- Nystagmus: periodical rhythmic movements of the eye
- Uncontrollable eye movement, usually a repetitive, slow movement in a specific direction followed by a quick adjustment to the centre
- Focus on the motor beat and the linked coordination
- Lateral gaze nystagmus: slow drift to midline and saccadic beating to the eccentric side
- Upbeat nystagmus: lesion at the anterior aspect of the vermis
- Downbeat nystagmus: lesion at the foramen magnum
- Tremor
- The constant oscillatory movement about a joint
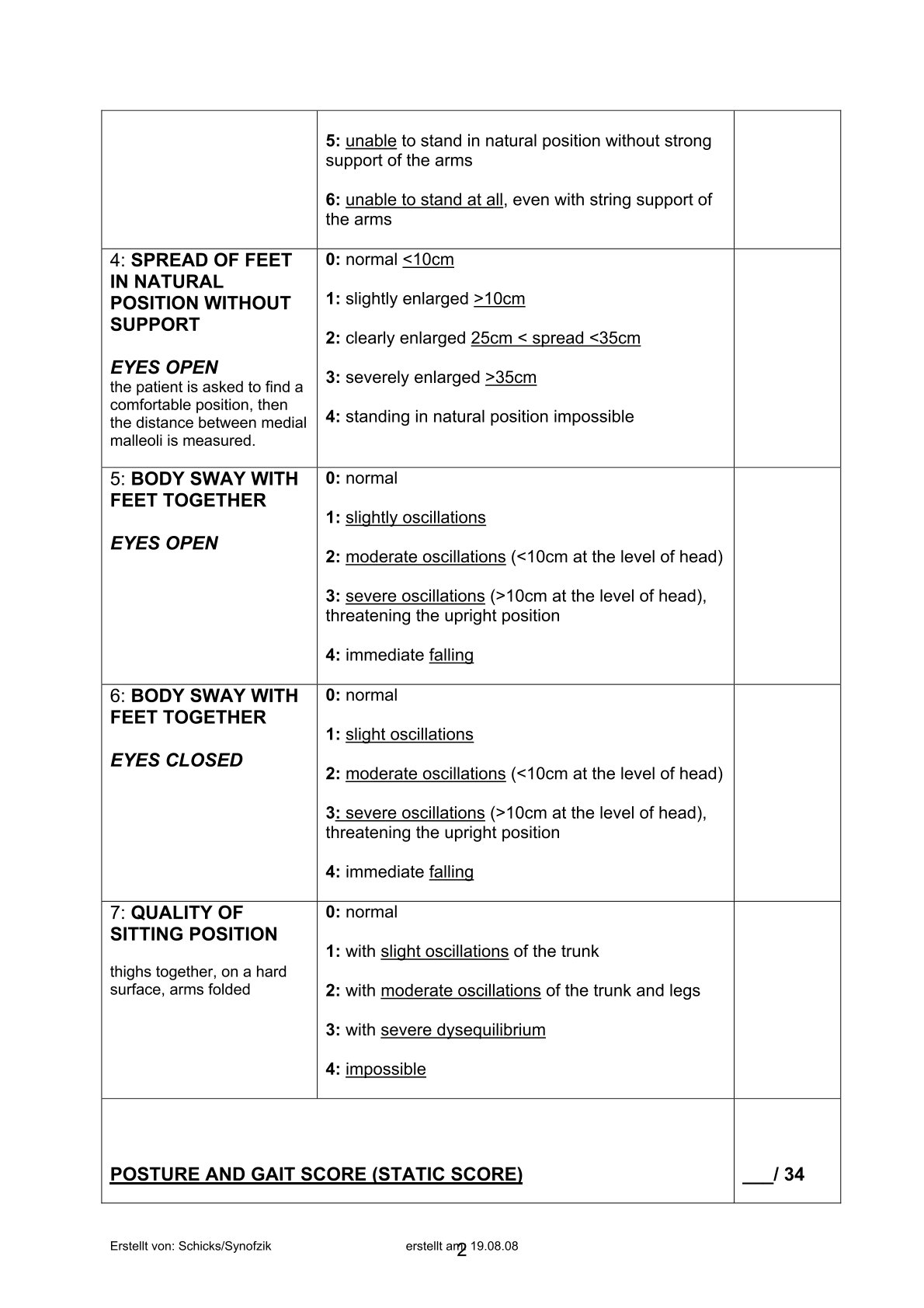
- Postural: during static sitting or standing, can be seen as truncal sway
- Intention: during movement at the proximal limb. Tremors that happen at the end of movements are called terminal tremor.
- Distal tremor is essential tremor
Parkinson’s disease vs cerebellar ataxia
Element | Parkinson’s disease | Cerebellar ataxia |
|---|---|---|
Frequency | Regular | Irregular |
Amplitude | Regular | Irregular |
Limb tremor (resting) | Present | Absent |
Ataxia: activity limitation
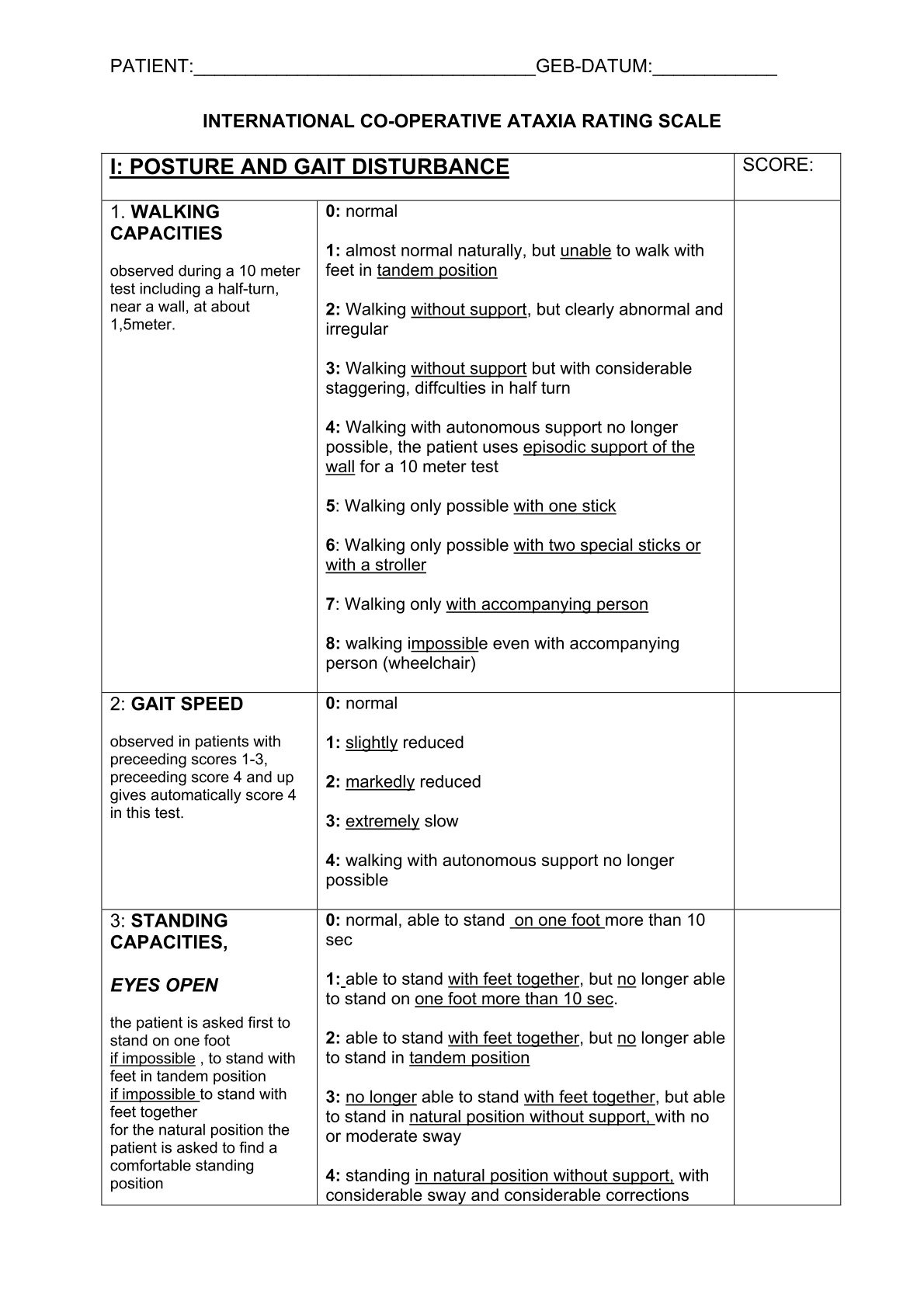
Ataxic gait: instead of thinking ‘is there an absence of coordination’, we should ask ‘how much incoordination is in this person’ = how much base of support?
- Wide base of support
- Irregular speed
- Irregular step length and step width (amplitude)
- Incoordination between hips, knees and ankle movements
Other examples of activity limitations
- PT-focused
- Bed mobility
- Transfers
- Sitting
- Standing
- Sit to stand
- Walking (indoors and outdoors)
- Stairs
- Reaching and manipulation
- OT-focused
- Showering
- Dressing
- Toileting
- Meal prep
- Laundry
- Cleaning
- Grocery shopping
Non-motor symptoms
- Psychiatric disorders
- Depression
- Anxiety is also a frequent complaint especially among patients with spinocerebellar ataxia
- Cognitive deficits
- This with classical cerebellar signs of motor syndromes can be explained by the disconnection at different levels of the cerebral-cerebellar circuit (Cerebral-cerebellar affective syndrome) (not about location but how it all works together)
- Visuospatial memory
- Language difficulties (anomia, agramatism)
- Executive dysfunction
- Poor planning, abstract reasoning
- Personality changes
- Affective swelling, disinhibition
- Difficulty interpreting and producing logical sequences
- This with classical cerebellar signs of motor syndromes can be explained by the disconnection at different levels of the cerebral-cerebellar circuit (Cerebral-cerebellar affective syndrome) (not about location but how it all works together)
- Sleep disorders
- Restless leg syndrome
- Sleep apnea
- Insomnia
- Frequent daytime sleepiness can be found in some but mechanism unknown
- Includes sleep hallucinations
- Fatigue
- Common symptom in neurodegenerative disorders
- Common in multiple sclerosis, parkinson’s disease, stroke
- Pain syndromes
- Cramps are present in 80% of SCA patients, ¼ listed as their very first syndromes
- 1-90 episodes a week
- Cramps are chief complaints which is almost ⅓ of all cases
- Lower extremities > face and trunk
- cramps
- Autonomic dysfunction
- Seen in specific neurodegenerative diseases such as early multiple system atrophy
- Symptomatic orthostatic dysfunction
- Urinary and erectile dysfunction
- Constipation
- Seen in specific neurodegenerative diseases such as early multiple system atrophy
Assessments
They measure spatial accuracy (amplitude) and temporal accuracy (timing and speed)
General observation: eyeball pattern recognition
Assessment | Type | Results | Reason |
|---|---|---|---|
General observation (eyeball pattern recognition) | Symptoms include
Serious or life-threatening causes
| ||
Age and gender | Children: cerebellitis Younger people (women): migraine | ||
Onset | Acute: needs special attention as can be fatal Chronic: primary tumor Intermittent pattern: transient ischemic attack, multiple sclerosis, inherited episodic ataxia | Differential diagnosis | |
Mental status | Site of motor corrdination Communicates with cerebrum for higher cortical functions | ||
Cranial nerve examination | Abnormal pursuit and saccade Extraocular dyskinsia Facial and tongue fasciculations: SCA3 Severe tongue atrophy and fasciculations: SCA 36 | ||
Vestibular signs | Vertigo, slow nystagmus Veer to ipsilateral Hearing loss for inner ear issues | ||
Cerebellar signs | Gait: tandem stance or walking are sensitive -> veer to same side, wide base in standing | ||
Extrapyramidal signs | Chronic progressive ataxia Indicates spread beyond cerebellum and brainstem SCA and parkinsonism (once striatum is involved, it is not responsive to levodopa) | ||
Strength | Symmetric proximal: myopathy Distal muscle weakness: generalised neuropathy | Degree of ataxia can be explained by muscle weakness | |
Proprioceptive sensory system | Positive romberg sign Worse when visual cues are removed If pure cerebellar, no diff | Spinocerebellar tracts: sensory input to cerebellum, hence sensory ataxia | |
Heel-to-shin (NIHSS item 10) | Impairment | ||
Finger-to-nose (NIHSS item 10) | Impairment | ||
Rebound test | Impairment | ||
Forearm supination-pronation test | Impairment | ||
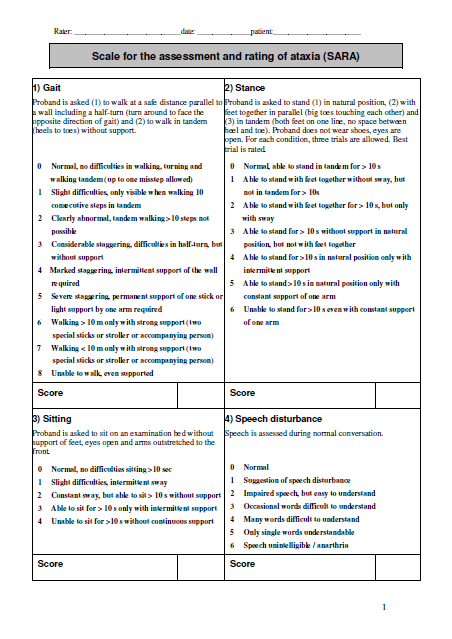
SARA | Impairment Activity limitation | ||
ICAR | Impairment Activity limitation | ||
Berg balance scale | Activity limitation |
Impairments and activity levels
- SARA
- ICARS
Activity scale
- Berg balance scale
Research evidence (Assessment)
Article | Systematic review of psychometric properties of balance measures for cerebellar ataxia | Balance outcome measures in cerebellar ataxia: a Delphi survey |
|---|---|---|
Authors | Stanley J winder Catherine M smith Leigh A hale Leica S claydon Susan L whitney Poonam Mehta | Stanley J winder Catherine M smith Leigh A hale Leica S claydon Susan L whitney |
Population | Mostly acquired ataxia (multiple sclerosis), needs more non-genetic ataxia | Cerebellar ataxia patients by 30 experts representing 10 countries |
Intervention | Berg balance, activity-specific balance confidence scale | SARA TUG BBS Available at low cost, require little equipment, and easy to perform |
Outcome | COSMIN: consensus based standards for the selection of health status Measurement Instruments Acceptable reliability and validity of measures but responsiveness is yet to be determined But quality of methodology in studies is mostly poor Quality of studies investigating psychometric properties of balance subcomponents: Poor to excellent MCID not determined | 75% consensus But psychometric properties have not been tested in genetic ataxia and responsiveness have not been tested |
Treatment approaches
- Restorative: impairment (80%)
- Eye and strengthening exercises, internal cues, balance
- Surgical and medical procedures for CNS recovery
- For stroke, they need this to be medically stable. To retore function, they will then need to rely on restorative methods
- Isoniazid pyridoxine, cannabis based medication, baclofen
- Thalamotomy, transcranial magnetic stimulation
- Compensatory: activity limitation and participation (20%)
- Environment such as tapes, visual, auditory, propriceptive
- Strategically placed weights to provide proprioceptive feedback and reduce tremors, improve motor functions and awareness of body position
- External such as walking aids
- Can be used to correct a movement and then be removed to facilitate restorative
- Parallel bars for walking
- Environment such as tapes, visual, auditory, propriceptive
Combine restorative and compensatory
All depends on
- Prognosis: acute vs degen
- Severity: mild vs severe
- Stage of rehab: early vs late
Other examples of treatment
Paper | Findings | Meaning |
|---|---|---|
Consensus paper: ataxic gait, 2022 | Training
Split belt treadmill paradigm for locomotive adaptation
Robot assisted gait training
Non-invasive brain stimulation + robotics + metaplasticity protocol: improvement in function of heel-to-shin, gait, sitting, and stance Dynamic movement orthosis: soft and flexible, improves gait parameters without restriction (decrease in trunk oscillations and body sway, decrease in double support phase and swing variability, increase in swing phase, increase in pelvic and knee ROM, increase control of knee during swing | When training, focus on intense multi-factor rehab. Mild-mod ataxia > severe ataxia in interlimb coordination and step length But they all can adapt walking patterns Robot (+ non invasive brain stim) + conventional is ok DMO is good |
Gait ataxia – specific cerebellar influences and their rehabilitations 2013 | FACTORS CONTRIBUTING TO ATAXIC GAIT Localisation of cerebellar functions
Balance impairments
Intralimb coordination
Oculomotor dysfunction
Dual tasking (cognitive and motor)
Adaptation of walking pattern
Ataxic gait rehab
| |
Systematic review of characteristics associated with cerebellar ataxia 2018 | P: 21 studies of quantitative gait assessment with 408 ataxic and 403 normal Findings:
| |
Rehabilitation of ataxic gait following cerebellar lesions: applying theory to practice | 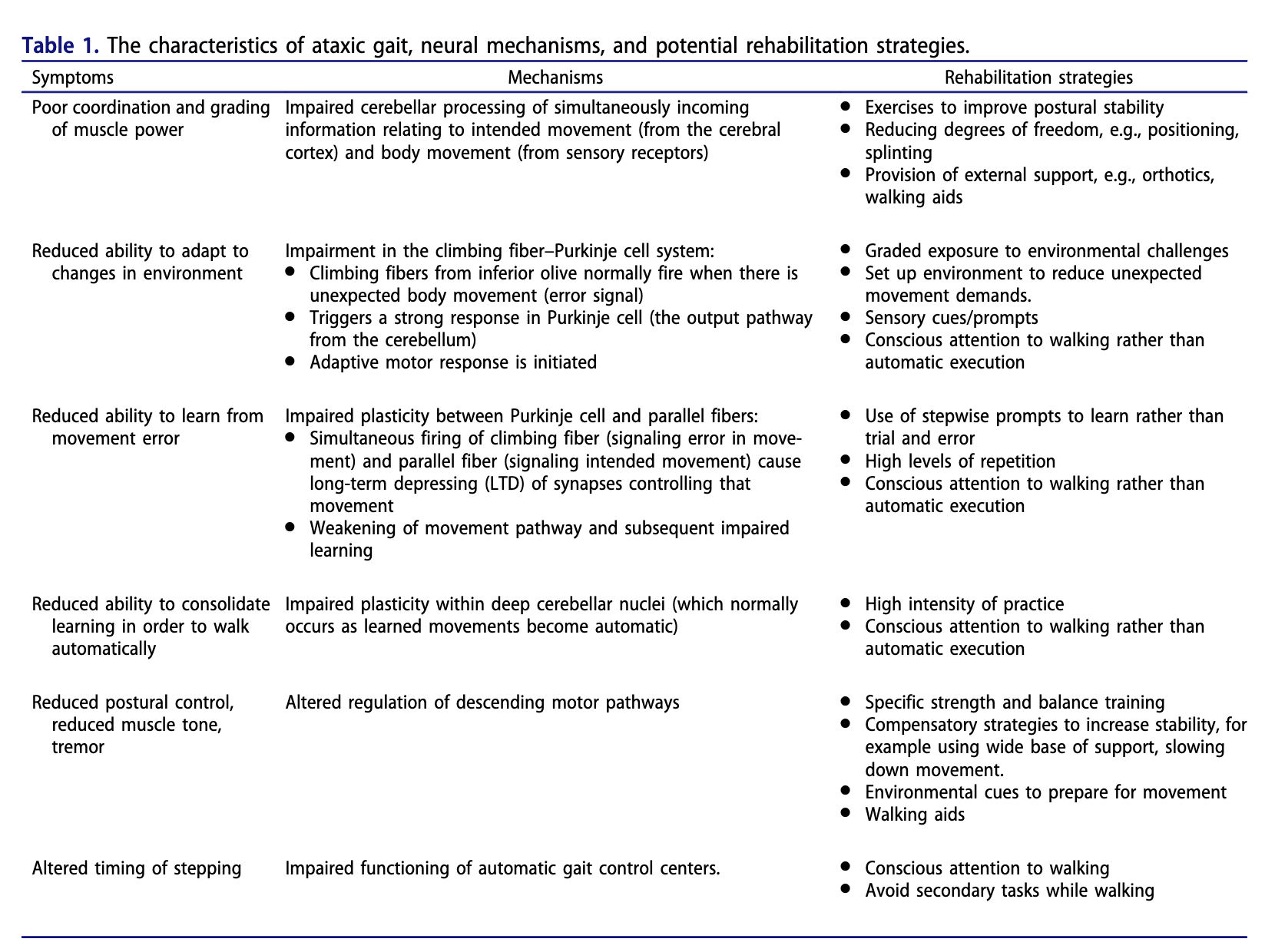 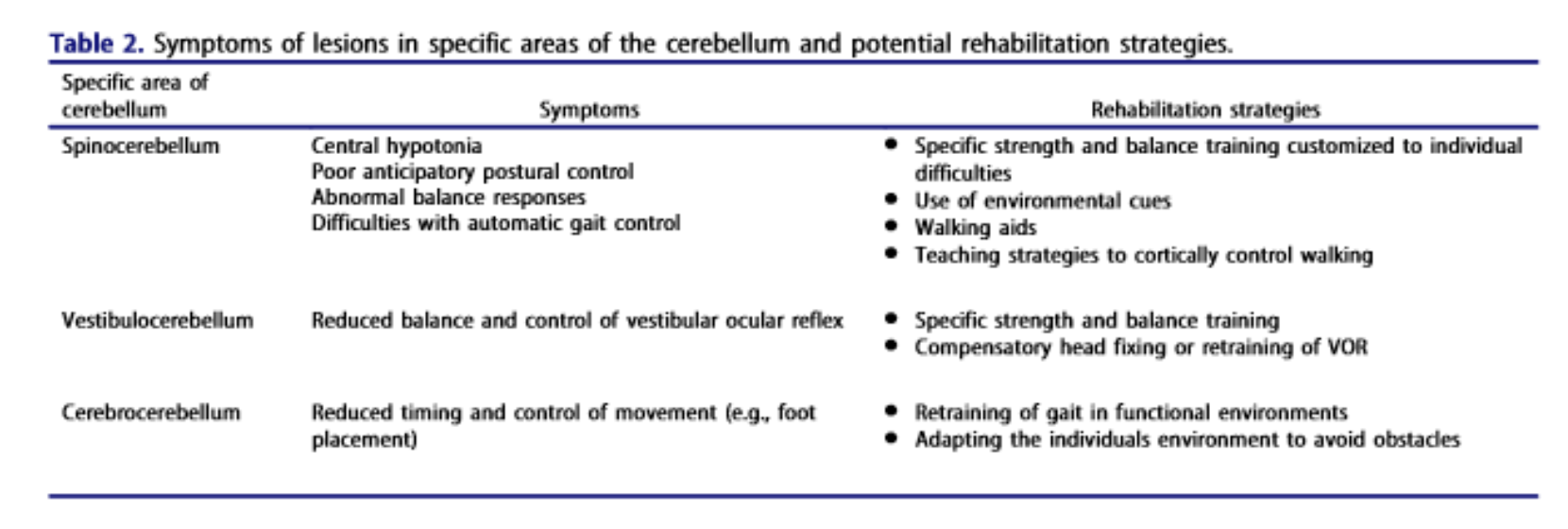 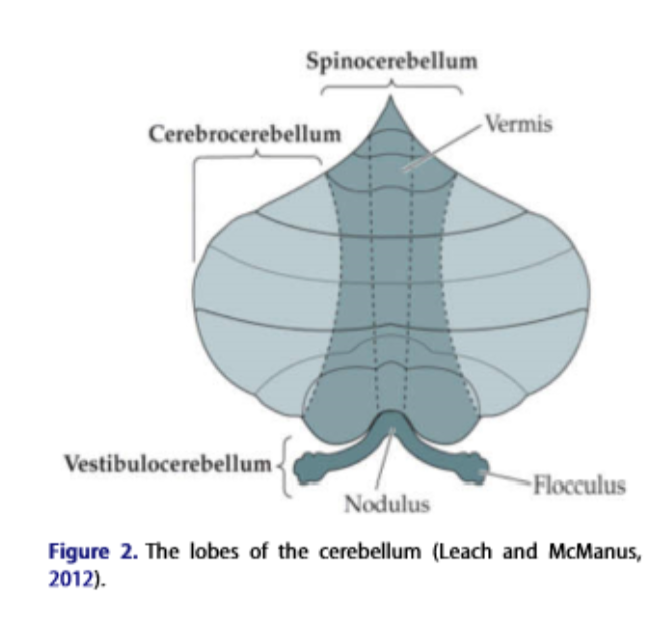 | |
Stability of the Trunk in Patients with Degenerative Cerebellar Ataxia During Walking 2016 |
|
Evidences (treatment)
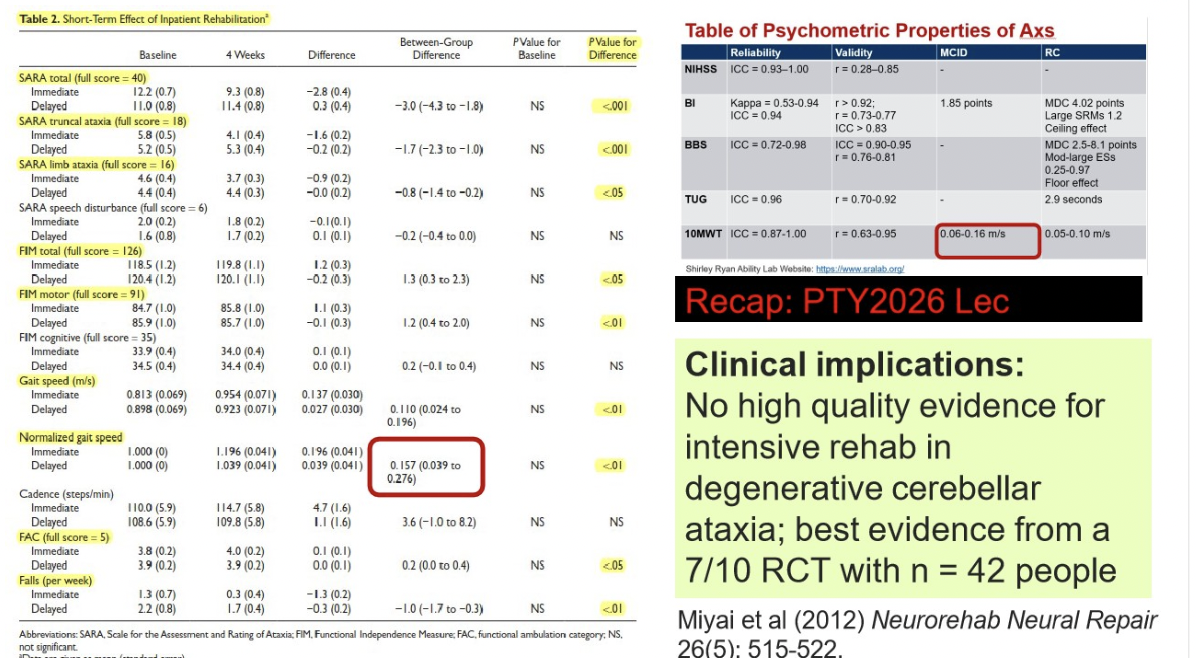
Article | Rehabilitation for individuals with genetic degenerative ataxia: a systematic review | Cerebellar ataxia rehabilitation trial in degenerative cerebellar disease |
|---|---|---|
Authors | Sarah c Milne 2017 LOUISE A CORBEN NELLIE GEORGIOU-KARISTIANIS MARTIN B DELATYCKI EPPLE M YIU | Miyai I Ito M Hattori n Mihara m Hatakenaka m Yagura h Sobue g Nishizawa m |
Population | 17 publications: 5 RCTs Degenerative ataxia Moderate to low quality studies | 42 pt with pure cerebellar degeneration |
Exposure | Rehab included coordination and balance training , multi-faceted inpatient rehab, a cycling regime, balance exercises with technology assisted biofeedback, respiratory muscle training, treadmill training 2 studies examined adjuncts | 2h inpatient physical and occupational therapy with focus on coordination, balance, ADLs on weekdays 1h on weekends 4 weeks |
Outcome | Emerging evidence (15/17) that rehab can improve gait, function, balance and/or ataxia for genetic degenerative ataxia (consistent despite quality) BUT less than half included assessment of long term outcomes and the follow up time frames varied
All except the feasibility study and compensatory OT intervention, has within group improvement in at least one outcome of gait, function, balance and/or ataxia Miyai et el: most conclusive evidence (NHMRC level 2) for between-group improvements in ataxia, function, number of falls and balance after 4 weeks of inpatient rehab for those with more pure cerebellar ataxia | Assessment and rating of ataxia
significantly greater functional gains in ataxia, gait speed, ADLs Short term benefits BUT functional status declined to baseline in 24 weeks, but gains are still maintained in more than half |