Basic X-ray
1. Basic Principles
Bones
Appear gray-white.
Heavily mineralized areas visible.
Growth plates visible in children.
Air
Appears black to dark gray.
Normal in airways & lungs, GI tract.
Air-fluid lines may be visualized.
Fluid
Appears gray.
2. Chest X-rays (CXR) / Radiographs
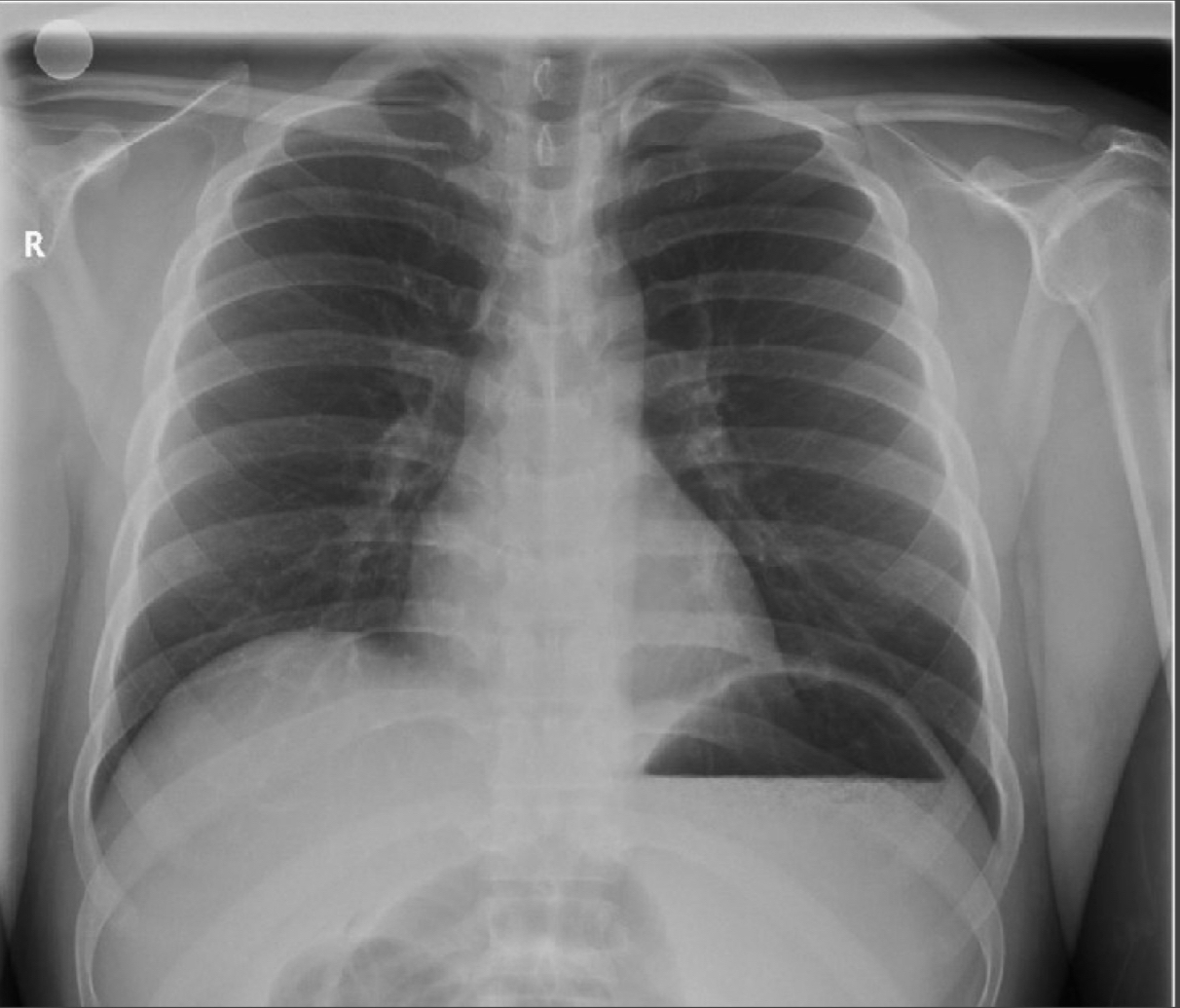
Views
PA (posterior-anterior): preferred; scapula do not obstruct lung fields.
AP (anterior-posterior): heart may appear larger.
Qualities to Assess
Rotation/Angle: twisted body or poor camera angle can distort heart size.
Inspiration:
Diaphragms should be at 9th rib on full inspiration.
Normal curve expected.
Flat diaphragms & expansion beyond 9th rib → air-trapping (asthma, COPD).
Exposure: must be adequate for clear structures.
Baseline Structures
Trachea, carina, right & left mainstem bronchi.
Lung fields, hilum, diaphragm.
Cardiac silhouette, pulmonary arteries, aortic knob.
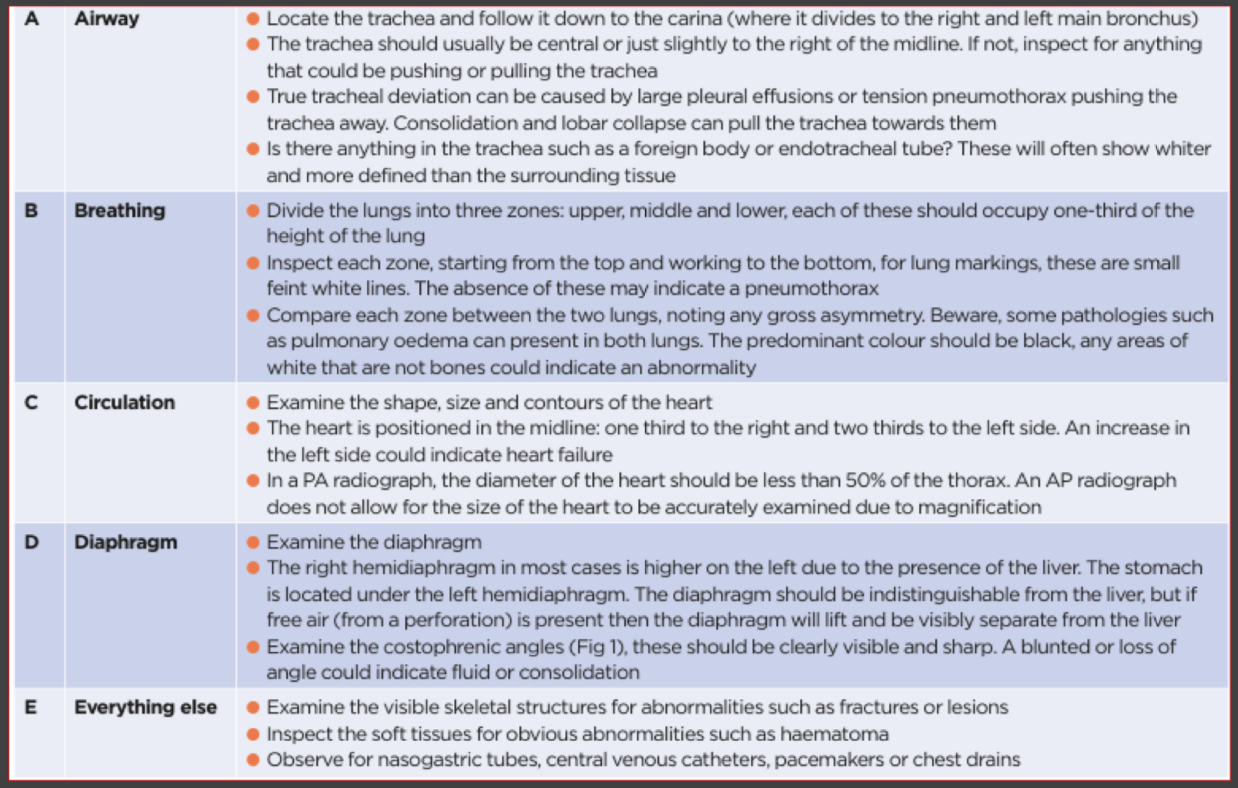
Systematic Approach
Follow a step-by-step method to interpret CXR findings.
3. Common Clinical Findings on X-rays
Tracheal Intubation
Placement visible on radiograph.
Right Mainstem Intubation
May cause atelectasis.
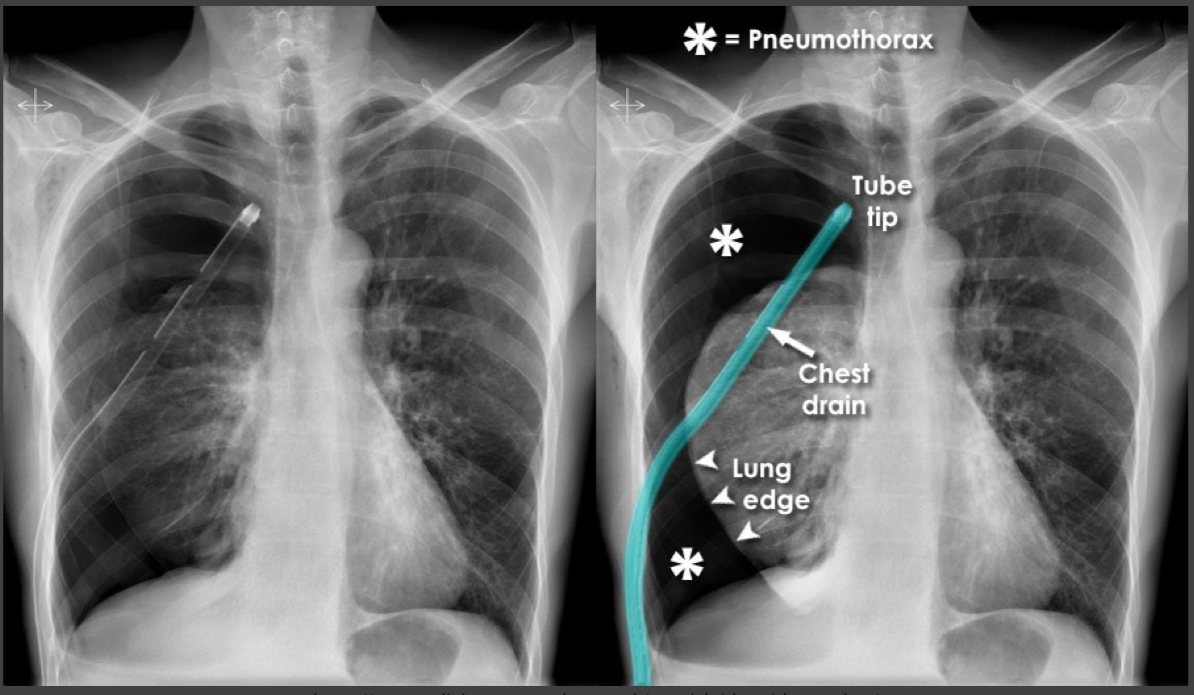
Pneumothorax
No lung markings.
Mediastinal shift with tracheal deviation.
Depressed left hemidiaphragm.
Treatment: chest tube insertion (note number of holes in tube).
ARDS (Acute Respiratory Distress Syndrome)
“Ground glass” effect.
Multifocal bilateral airspace opacities.
Perihilar & lower zone distribution.
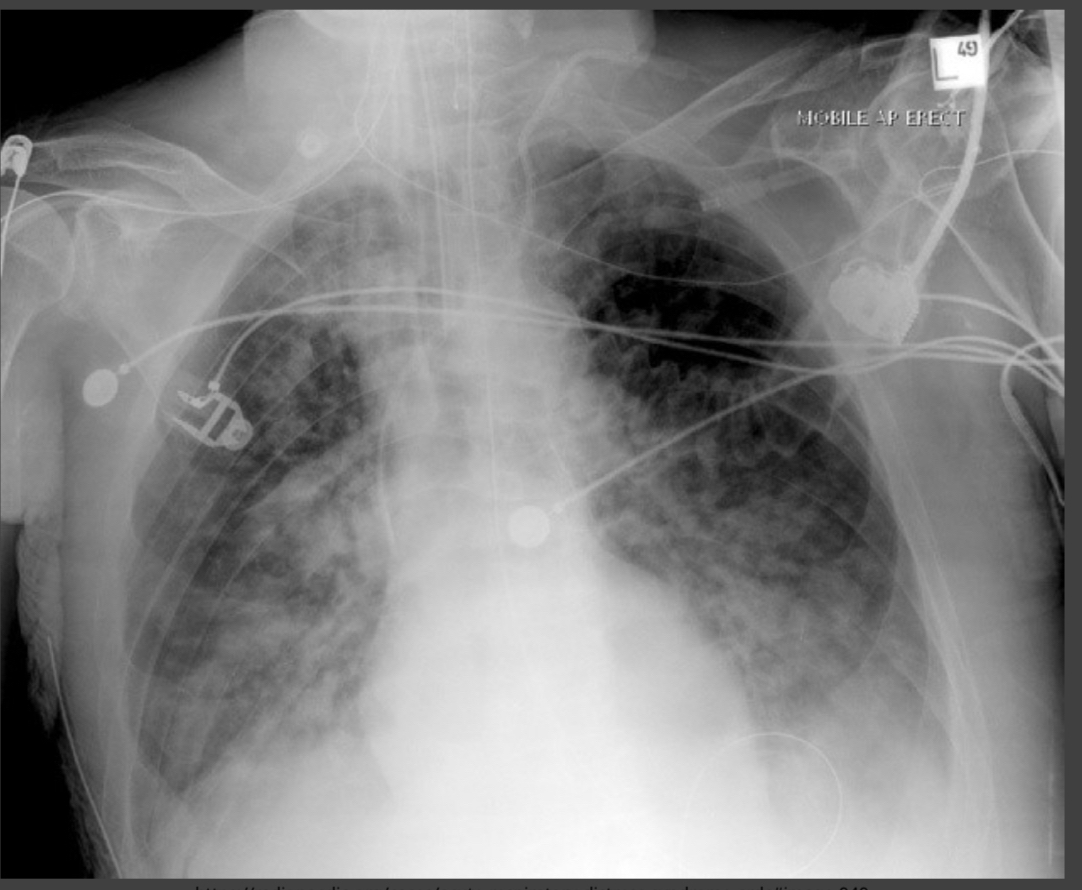
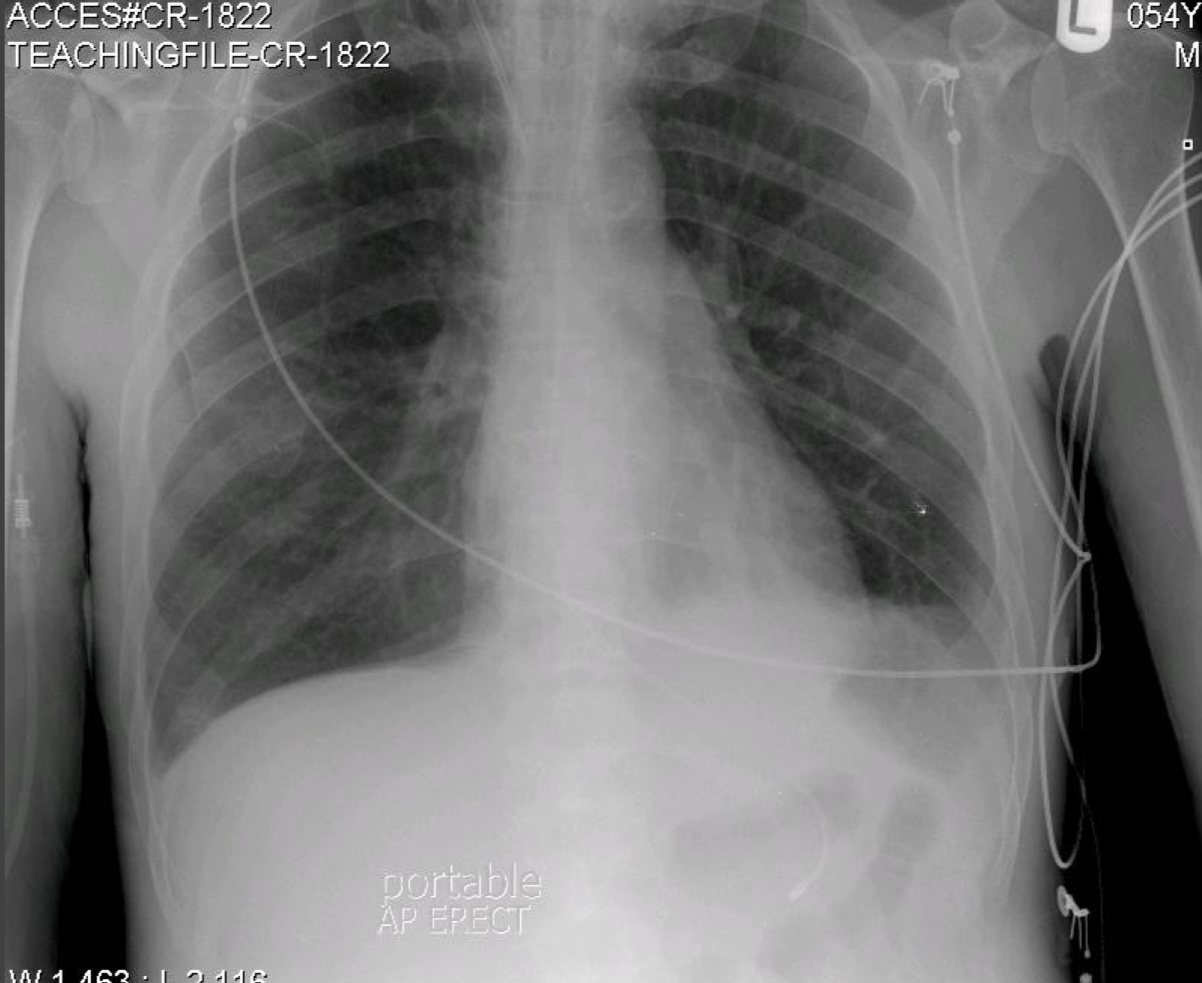
Central Venous Catheter
Ideal tip location: cavo-atrial junction.
4. Gastrointestinal & Abdominal X-ray Findings
Air-Fluid Levels
Show patient’s position.
Normal in GI tract.
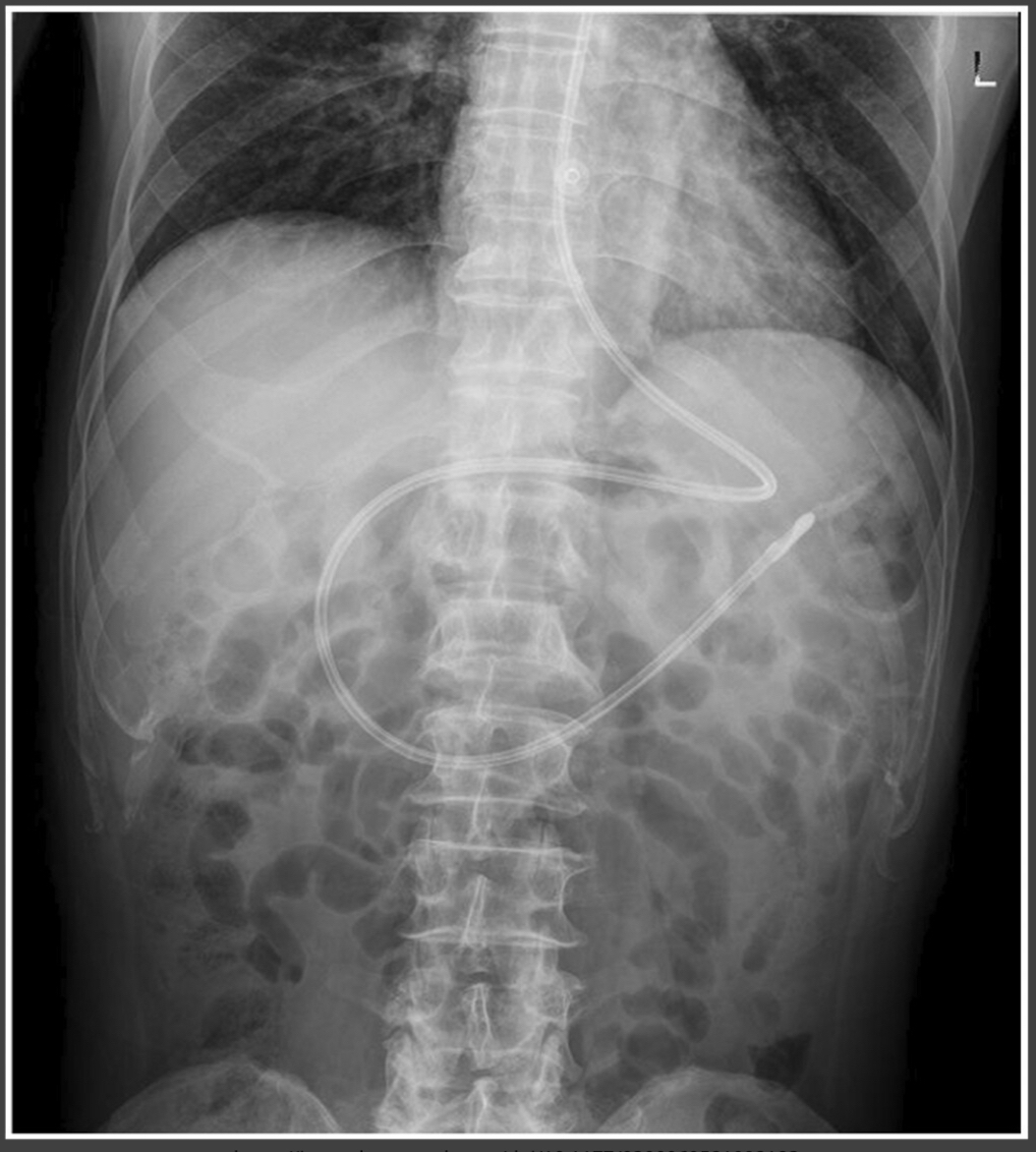
Nasogastric (NG) Tube
Tip should be below diaphragm.
Tip remains left of spine.
Nasoduodenal Tube
Crosses from left to right side of spine.
Advances toward jejunum.
Small Bowel Obstruction
“Stacked coin” appearance.
Air-fluid levels visible on erect film.
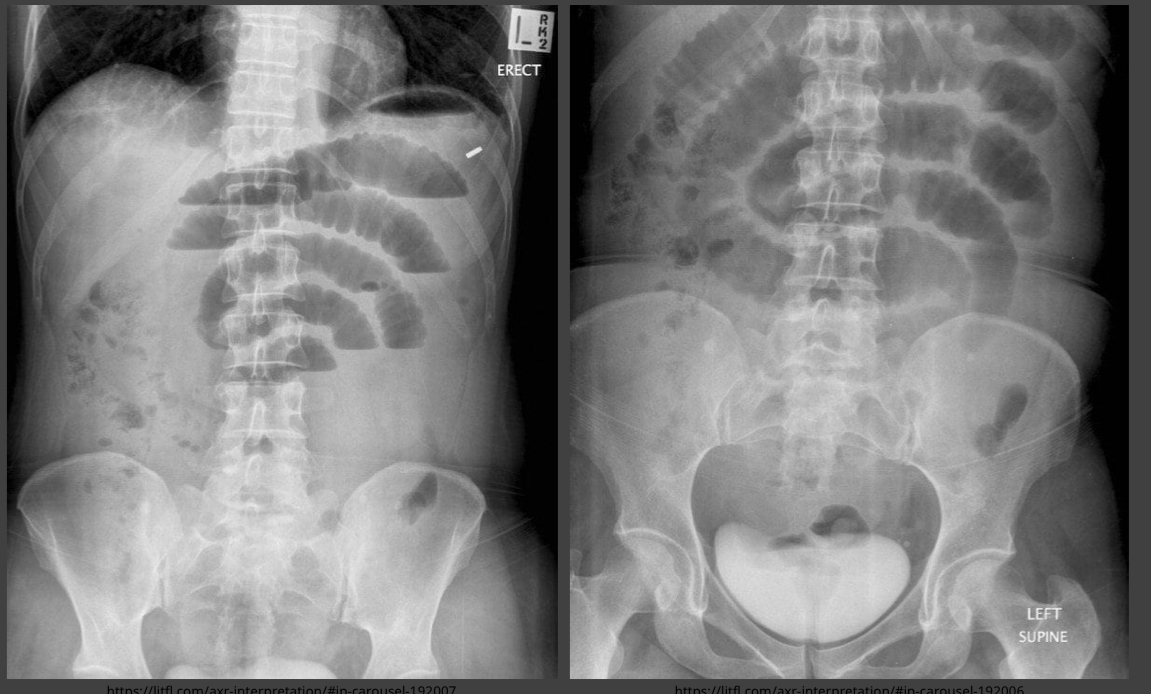
Dilated Bowel
Indicates large bowel obstruction.
