Chapter_5-_Aerosol_Therapy__1_
AEROSOL THERAPY
Introduction
Aerosol: solid or liquid particles suspended in a gas.
Common practice in respiratory and critical care: delivery of drugs in aerosolized form.
Benefits of aerosolized therapy:
Directly targets the airway, minimizing systemic side effects.
Bypasses first-pass metabolism in the gastrointestinal tract and liver.
Indications for Aerosol Therapy
Diagnostic Uses
Airway responsiveness and bronchodilator reversibility tests
Ventilation scans
Dosimetry
Therapeutic Uses
Treatment of lung diseases:
Airway and lung parenchymal diseases
Systemic diseases like diabetes mellitus
Infections
Classification of Aerosols
A) Bland Aerosols
Types: heated or cooled sterile water, saline
Uses: treatment of upper airway diseases, humidification of bypassed airways, sputum induction.
B) Medicated Aerosols
Contains: bronchodilators, steroids, mucokinetic agents, local anesthetics, antimicrobials, etc.
Uses:
Upper airway conditions (inflammation, nasal allergy, infections)
Lower airway diseases: obstructive airway disease, cystic fibrosis, ARDS, and infections.
Nasal spray applications: insulin for diabetes and vasopressin for diabetes insipidus.
Aerosol Physics
Factors affecting depth of aerosol delivery:
Size and characteristics of aerosol
Amount of aerosol
Airway anatomy and geometry
Breathing patterns
Aerosols get deposited by 3 mechanisms, namely:
Diffusion
Inertial impaction
Sedimentation
Mechanisms of Aerosol Deposition and Particle Sizes
Major mechanisms:
Inertial impaction occurs with larger (>3 µm), fast-moving particles
Gravitational sedimentation (function of mass and time)
Diffusion (Brownian motion ) occurs with particles smaller than 1 µm
Particle filter effects:
10 µm: filtered in the nose/oropharynx
5–10 µm: reach proximal lower respiratory tract
1–5 µm: reach lung periphery
Mass Median Aerodynamic Diameter (MMAD)
Clinical aerosols are heterodisperse (varied sizes).
MMAD: measures particle size in µm above and below which 50% of the mass is contained.
Higher MMAD indicates more larger particle sizes.
Size and Particle Deposition
Particle size deposition:
<0.5 µm: no deposition
0.5–2 µm: alveoli
2–5 µm: bronchi and bronchioles
5–100 µm: mouth, nose, and upper airway
100 µm: filtered by the upper respiratory tract
Size and Physical Characteristics
Important characteristics: volume/surface area ratio, MMAD, geometric standard deviation; MMAD is the most crucial.
Therapeutic aerosols: MMAD typically ranges from 0.5 to 5 microns.
Influences on aerosol size and site of impaction: density, temperature, humidity, and more.
Effect of Ventilatory Pattern on Deposition
Normal breathing flow rate: 0.5 L/s promotes aerosol delivery to bronchi/bronchioles (laminar flow).
Higher flow rates cause turbulence, aerosol fragmentation.
Optimal technique: slow, deep breathing with a 5-10 seconds breath-hold.
Airway Geometry and Aerosol Delivery
Inhalation method influences deposition: mouth inhalation improves delivery compared to nose inhalation.
Intervals (2-10 minutes) between inhaler actuation can aid in better drug delivery during subsequent doses.
Advantages and Disadvantages of Aerosol Therapy
Advantages
Smaller doses compared to systemic therapies.
Faster onset of action than oral dosing.
Direct lung delivery minimizes systemic exposure.
Less painful than injections, relatively comfortable.
Disadvantages
Low lung deposition fraction: many variables can impact delivery efficacy.
Coordination issues in using devices can hinder effectiveness.
Variability in device types can confuse users.
Hazards of Aerosol Therapy
Adverse reactions: headaches, insomnia, and potential bronchospasm from cold/high-density aerosols.
Increased drug concentration in nebulizers due to evaporation or heating.
Risk of infection from contaminated aerosol devices.
Eye irritation from medication delivered via face masks.
Methods of Aerosol Generation
Nebulizers:
Types include pneumatic, ultrasonic, and vibrating mesh nebulizers.
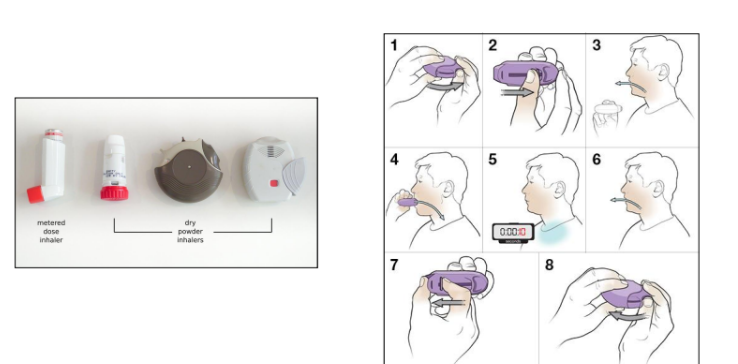
Metered Dose Inhalers (MDI):
Pressurized devices featuring a canister and holding chamber.
Dry Powder Inhalers:
Such as Rotahaler and Turbuhaler.
Nebulizers
Pneumatic/Jets Nebulizers
Function based on Bernoulli Principle.
Types: Small Volume Nebulizers (SVNs) and Large Volume Nebulizers.
Small Volume Nebulizers (SVN)
Hand-held or used in ventilation circuits.
Gas flow rates: 6-8 L/m, optimal solution volume: 4-5 ml, particle size: 1-5 µm.
Large Volume Nebulizers
Suitable for prolonged aerosol delivery, effective in upper airway edema treatment.
Ultrasonic Nebulizers
Use a piezoelectric crystal to create ultrasonic vibrations, generating aerosol.
Vibrating Mesh Nebulizers
Use mesh deformation to push liquid drug through mesh, creating inhalable droplets.
Metered Dose Inhalers (MDIs)
Portable, multi-dose devices.
Contains medication, surfactant, and propellant (HFA).
Advantages and Disadvantages of pMDI
Advantages
Compact and portable
Multiple doses with reduced infection risk
Short treatment time with reproducible doses
Disadvantages
Requires coordination between hand and breath
Challenges in determining remaining doses.
Optimal Technique for MDI Use
Important factors: coordination, breath-holding, and proper storage at 37 °C to maintain pressure and aerosol size.
Dry Powder Inhalers
Advantages: portable, no CFC hazards, no synchronization required.
Limitations: Some need assembly, affected by humidity, and high inspiratory flow rates required for efficacy.
Summary of Hazards of Aerosol Therapy
Risks for Patients
Include bronchospasm, infection, airway obstruction, and device malfunction.
Risks for Caregivers
Exposure to asthma and infections.
Environmental Risks
CFCs contribute to ozone layer depletion; HFA is less harmful.