Update on sinonasal malignancies
Introduction to Sinonasal Tract Malignancies
Sinonasal tract malignancies are rare, making up about 1% of all human cancers and less than 5% of head and neck cancers.
They primarily occur in the maxillary sinus, nasal cavity, and ethmoid sinus.
These cancers pose diagnostic challenges due to overlapping histological features among different tumor types.
Diagnostic Challenges
Pathologists face difficulties in differentiating between various sinonasal cancers due to similarities in histology.
Accurate diagnosis is crucial because these tumors can invade adjacent structures leading to serious complications.
The adoption of functional endoscopic sinonasal surgery has improved specimen sampling and resection capabilities, aiding diagnosis.
Objective and Approach
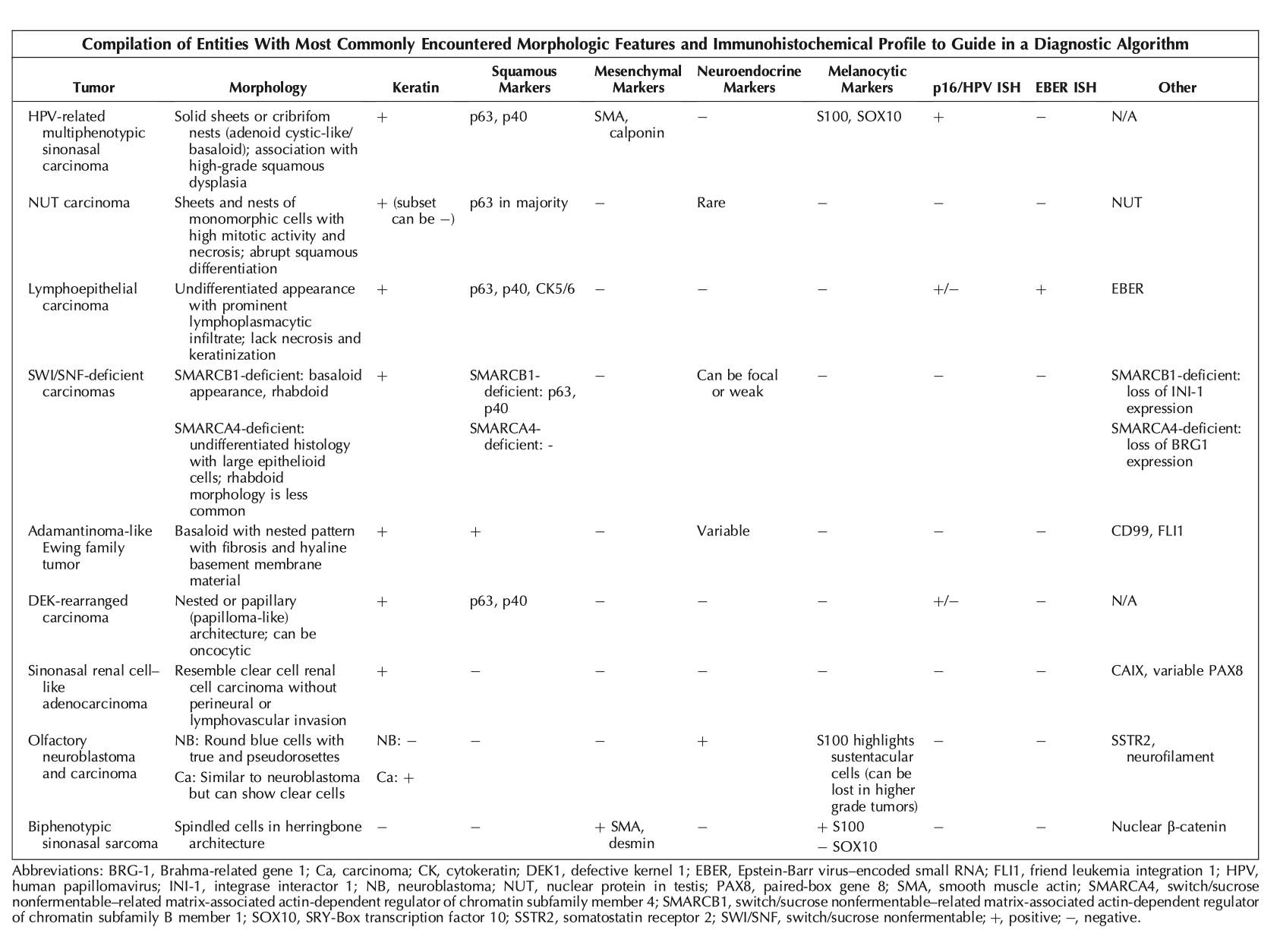
The review aims to create a streamlined algorithm to facilitate diagnosis using histological clues, immunohistochemical profiles, and molecular assays.
Distinct immunohistochemical and molecular markers can assist in differentiating cancer types despite their similar histology.
Emerging Sinonasal Tumors
HPV-Related Multiphenotypic Sinonasal Carcinoma
Previously referred to as HPV-related carcinoma with adenoid cystic features, now recognized for varied histology.
Predominantly affects females with typical symptoms of epistaxis or nasal obstruction.
High recurrence rate (35%) but no cancer-related mortality reported.
Histological features include solid sheets and cribriform nests with basaloid appearance; strong expression of p16 and positive for high-risk HPV.
NUT Carcinoma
A more aggressive tumor predominantly seen in young adults, often found in the sinonasal tract.
Symptoms include nasal obstruction, pain, and headaches; patients frequently present with metastatic disease.
Poor prognosis with a 30% survival rate; distinct histological appearance shows nests of small round blue cells and squamous differentiation features.
Lymphoepithelial Carcinoma
Associated with Epstein-Barr virus, predominantly occurs in males, especially in Southeast Asia.
Features an undifferentiated appearance with lymphoplasmacytic infiltrate.
Generally has favorable prognosis despite nodal involvement; commonly expresses p63, p40, and shows patchy p16 expression.
SWI/SNF-Deficient Carcinomas
Characterized by mutations in SWI/SNF complex, often presenting with variable histologies.
SMARCB1-deficient tumors exhibit uniquely basaloid or rhabdoid features.
Prognosis tends to be poor, with many patients dying within two years of diagnosis.
Biphenotypic Sinonasal Sarcoma
Typically found in the nasal cavity, characterized by infiltrative spindle cells.
Molecular profile shows PAX3 fusion, among others, with a relatively good prognosis over time.
Adenocarcinomas of Sinonasal Tract
Sinonasal Adenocarcinoma
Divided into intestinal and nonintestinal types, with various unique entities under nonintestinal adenocarcinomas.
Most cases show seromucinous differentiation; specific mutations and fusions have been associated with certain tumor types.
Recent emerging entities include sinonasal adenocarcinoma with ETV6::NTRK3 fusions.
Tumors of Neuroectodermal Origin
Olfactory Neuroblastoma and Carcinoma
Olfactory neuroblastoma originates from the olfactory epithelium and exhibits a round blue cell morphology with neuroendocrine differentiation.
Olfactory carcinoma shares similarities but shows varying keratin markers and distinct clinical behavior.
Treatment approaches include somatostatin receptor targeting, which has shown promise in clinical trials.
Progress in Molecular Diagnostics
Advances have led to improved classification of sinonasal tumors based on genetic alterations and methylation profiling.
IDH mutations indicate a specific tumor category with better prognostic outcomes, as opposed to IDH-wild-type tumors.
Comprehensive genetic profiling can clarify the differentiation between similar malignancies and direct targeted therapies.
Conclusion
Sinonasal malignancies exhibit a diverse array of histological features and molecular characteristics.
A systematic diagnostic approach leveraging clinical data, immunohistochemistry, and molecular assays is advised for accurate tumor classification.
Continuous research is essential for further understanding of these tumors and enhancing patient prognosis.