PERIODONTAL PARAMETERS AND ANATOMY
CLINICAL LANDMARKS
Gingival Margin: The edge of the gum tissue that meets the teeth.
Gingival Sulcus: The space between the tooth and the gum tissue that contains the free gingiva.
Free Gingiva: Unattached portion of the gingiva, extending from the gingival margin to the free gingival groove.
Attached Gingiva: The part of the gingiva that is firmly bound to the underlying alveolar bone.
Mucogingival Junction: The line of demarcation between the keratinized attached gingiva and the non-keratinized alveolar mucosa.
Alveolar Mucosa: The soft tissue that covers the alveolar bone.

MARGINAL / FREE GINGIVA
The marginal, unattached, free gingiva = border of the gingiva surrounding the teeth in collar like fashion
In about 50% of cases, demarcated from the attached gingiva by a shallow linear depression, the free gingival groove (forms the soft tissue wall of the gingival sulcus)
ATTACHED GINGIVA
The attached gingiva is continuous with the marginal gingiva.
It is firm, resilient, and tightly bound to the underlying periosteum of alveolar bone.
Extends to the loose and movable alveolar mucosa, demarcated by the mucogingival junction
KERATINIZED GINGIVA
Width of the keratinized gingiva on the facial aspect differs in different areas of the mouth.
Greatest width in the incisor region (3.5 to 4.5 mm in the maxilla and 3.3 to 3.9 mm in the mandible) and less in the posterior segments.
Least width in the first pre-molar area (1.9 mm in the maxilla and 1.8 mm in the mandible)
WIDTH OF KERATINIZED GINGIVA (KG) = FREE GINGIVA + ATTACHED GINGIVA
ATTACHED GINGIVA VS ALVEOLAR MUCOSA
Features | Attached Gingiva | Alveolar Mucosa |
|---|---|---|
Color | Pale pink | Brighter red hue |
Tissue Type | Firm, immobile | Movable tissue |
Attachment | Tightly attached to the underlying bone | Loosely bound to the bone |
Keratinization | Keratinized | Non-keratinized |
Elastic Fibers | No elastic fibers | Presence of elastic fibers |
Connective Tissue | Dense connective tissue | Loose connective tissue |
METHODS OF IDENTIFICATION
Clinical
Alveolar mucosa appears more red due to non keratinized thin epithelium and prominent blood vessel

Functional
using a probe move the mucosa from apical to coronal direction
roll technique

Histological
Lugol’s iodine solution stains alveolar mucosa
due to the higher glycogen content

SIGNIFICANCE OF KERATINIZED TISSUE
Helps to withstand the masticatory forces,
Sufficient width provides a good vestibular depth which facilitates optimal oral hygiene measures, thus serving to reduce inflammation
Inadequate width leads to plaque accumulation and inflammation
Gingival recession is common in sites of deficient width
GINGIVA - HISTOLOGY
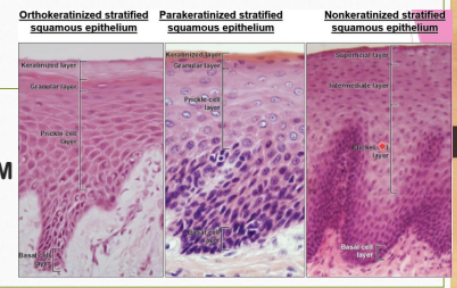
ORAL OR OUTER EPITHELIUM (OE)
The oral or outer epithelium covers the crest and outer surface of the marginal gingiva and the surface of the attached gingiva. It is usually parakeratinized.
The degree of gingival keratinization diminishes with age and the onset of menopause
SULCULAR EPITHELIUM (OSE)
The sulcular epithelium lines the gingival sulcus. It is a thin, nonkeratinized stratified squamous epithelium without rete pegs
Extends from the coronal limit of the junctional epithelium to the crest of the gingival margin

TYPES OF EPITHELIUM
GINGIVA - HISTOLOGY CONT.
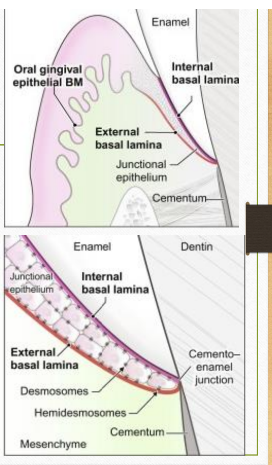
JUNCTIONAL EPITHELIUM
Consists of a collar-like band of stratified squamous nonkeratinizing epithelium.
It is three to four layers thick in early life, but the number of layers increases with age to 10 or even 20 layers.
The length of the junctional epithelium ranges from 0.25 to 1.35 mm
The junctional epithelium is attached to the tooth surface (epithelial attachment) by means of an internal basal lamina and to the gingival connective tissue by an external basal lamina
The attachment of the junctional epithelium to the tooth is reinforced by the gingival fibers, which brace the marginal gingiva against the tooth surface. For this reason, the junctional epithelium and the gingival fibers are considered a functional unit, referred to as the dentogingival unit.
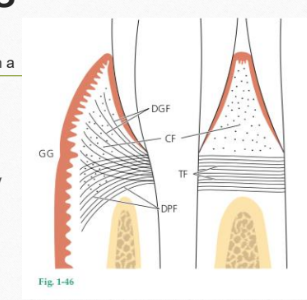
GINGIVAL FIBERS
CIRCULAR FIBERS (CF)
Fiber bundles which run their course in the free gingiva and encircle the tooth in a cuff- or ring-like fashion.
GINGIVODENTAL FIBERS
Embedded in the cementum of the supra-alveolar portion of the root and project in a fan-like configuration coronally and apically into the free gingival tissue and periosteum of the alveolar bone
TRANSSEPTAL FIBERS (TF)
The transseptal fibers run straight across the interdental septum and are embedded in the cementum of adjacent teeth
They are a remarkably constant finding and are reconstructed even after destruction of the alveolar bone has occurred in periodontal disease
CLINICAL RELEVANCE OF GINGIVAL FIBERS
The gingival fibers brace the gingiva against the tooth and provide the rigidity necessary to withstand the forces of mastication without being deflected away from the tooth surface.
Because of the high turnover rate, gingiva has remarkable healing and regenerative capacity and shows little evidence of scarring after surgical procedures.
The high proliferative capacity of junctional epithelium is the primary reason for the ‘Long Junctional epithelium’ type of healing that is normally seen after scaling and root planing.
Also the proliferative capacity necessitates the basis for epithelial exclusion, by placing a GTR membrane during periodontal regenerative procedures.
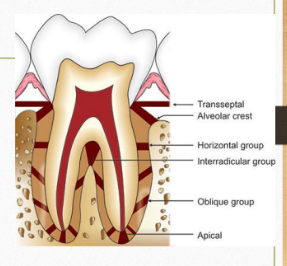
PERIODONTAL LIGAMENT FIBERS
Composition: Primarily made of Type I collagen arranged in discrete fiber groups.
ALVEOLAR CREST GROUP (ACF)
Extend obliquely from the cementum just beneath the junctional epithelium to the alveolar crest .The alveolar crest fibers prevent the extrusion of the tooth and resist lateral tooth movements.
HORIZONTAL GROUP (HF)
Horizontal fibers extend at right angles to the long axis of the tooth from the cementum to the alveolar bone
OBLIQUE GROUP (OF)
Oblique fibers, the largest group in the periodontal ligament, extend from the cementum in a coronal direction obliquely to the bone . They bear the brunt of vertical masticatory stresses and transform them into tension on the alveolar bone.
APICAL GROUP (APF)
The apical fibers radiate in a rather irregular fashion from the cementum to the bone at the apical region of the socket. They do not occur on incompletely formed roots.
INTERRADICULAR FIBERS
The interradicular fibers fan out from the cementum to the tooth in the furcation areas of multirooted teeth.
TRANSSEPTAL GROUP
Transseptal fibers extend interproximally over the alveolar bone crest and are embedded in the cementum of adjacent teeth . These fibers may be considered as belonging to the gingiva because they do not have osseous attachment.
PERIODONTAL LIGAMENT
Width: Ranges from 0.13 to 0.25 mm.
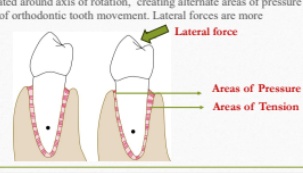
Primary function is to bear masticatory forces. When an axial force is applied to a tooth, a tendency toward a displacement of the root into the alveolus occurs. The oblique fibers alter their wavy, untensed pattern, assume their full length, and sustain the major part of the axial force. Periodontal ligament is suited best to withstand vertical (axial) forces
When lateral forces are applied, tooth is rotated around axis of rotation, creating alternate areas of pressure and tension. This forms the basic rationale of orthodontic tooth movement. Lateral forces are more damaging to the periodontal ligament.
CEMENTUM
Types of Cementum:
Acellular Afibrillar Cementum (AAC): contains neither cells nor extrinsic or intrinsic collagen fibers, and is found in coronal cementum
Acellular Extrinsic Fiber Cementum (AEFC): composed almost entirely of densely packed bundles of Sharpey's fibers and lacks cells, found in the cervical third of roots
Cellular Mixed Stratified Cementum (CMSC): is composed of extrinsic (Sharpey's) and intrinsic fibers and may contain cells, primarily in the apical third of the roots and apices and in furcation areas
Cellular Intrinsic Fiber Cementum (CIFC): contains cells but no extrinsic collagen fibers
CLINICAL RELEVANCE OF CEMENTUM
Cementum is thinnest in the coronal third of the root surface(16 to 60 m) and reaches greatest thickness in apical third and in the furcation areas(150 to 200 m).
In periodontitis, due to the inflammatory process, the coronal cementum decalcifies. Attempts at root planing may easily remove this thin layer , leading to increased root sensitivity commonly observed during and after root planing procedures.
Since acellular cementum does not contain cells, it is difficult to regenerate acellular cementum. This explains why true periodontal regeneration has never been completely predictable.
Enamel matrix proteins have been used in periodontal regenerative procedures, because it has been observed that these proteins stimulate acellular cementum formation.
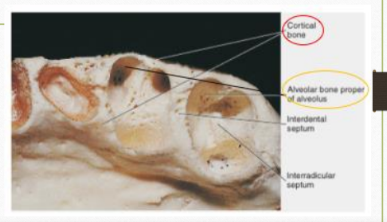
ALVEOLAR BONE
An external plate of cortical bone formed by haversian bone and compacted bone lamellae.
The inner socket wall of thin, compact bone called the alveolar bone proper. Histologically, it contains a series of openings (cribiform plate) through which neurovascular bundles link the periodontal ligament with the central component of the alveolar bone, the cancellous bone. Radiographically, it is seen as the Lamina Dura
Cancellous trabeculae, between these two compact layers, acts as supporting alveolar bone. The interdental septum consists of cancellous supporting bone enclosed within a compact border.
CLINICAL RELEVANCE OF ALVEOLAR BONE
The interdental septum is more fragile than the outer cortical plate. During extraction, while using luxators in the interdental area, it is important to apply controlled pressure to preserve the interdental bone.
The cancellous nature of the interdental bone makes it the primary site to show earliest evidence of bone loss in periodontitis.
Periodontal disease results in early loss of interdental bone whereas the outer cortical plates, which is more dense may still be preserved. This explains the crater shaped type of defect, which is the most common and forms the majority of periodontal osseous defects.
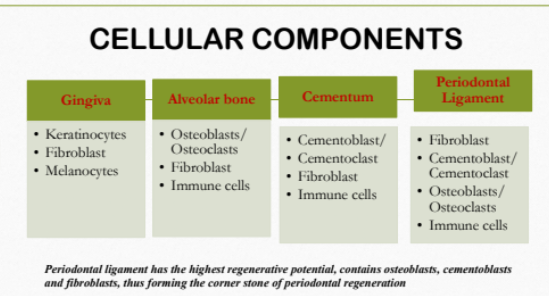
CELLULAR COMPONENTS
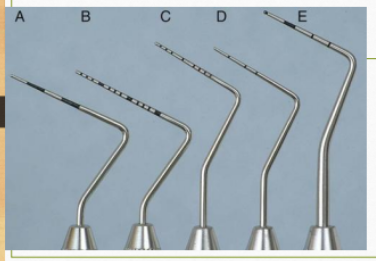
TYPES OF PERIODONTAL PROBES
Marquis Probe: Markings at 3, 6, 9, 12 mm.
UNC-15 Probe: 15 mm long with 1 mm markings.
Williams Probe: Markings at 1, 2, 3, 5, 7, 8, 9, 10 mm.
Michigan O Probe: Markings at 3, 6, 8 mm.
WHO Probe: 0.5 mm ball at the tip; markings at 3.5, 5.5, 8.5, 11.5 mm with a black band between 3.5-5.5 mm.
CLINICAL PARAMETERS
Probing Depth (PD):
Gingival margin to base of sulcus
variable
Clinical Attachment Level (CAL):
CEJ to base of sulcus
fixed reference point
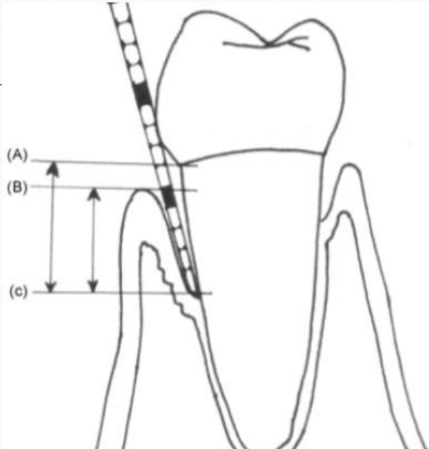
CLINICAL DETERMINATION OF PARAMETERS
Probing Depth (PD):
Distance between Free Gingival Margin and apical point of probe penetration (B-C)
Recession (REC):
Distance between CEJ and FGM (A-B)
Clinical Attachment Level (CAL):
Distance between CEJ and apical point of probe penetration (A-C)
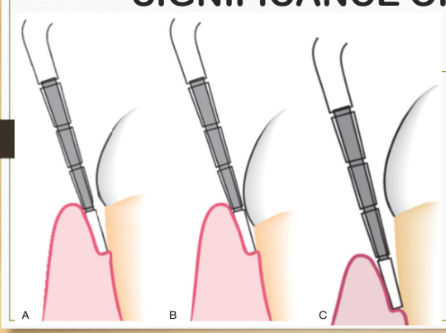
SIGNIFICANCE OF CAL
Situation A: Gingival margin at CEJ, thus probing depth equals CAL.
Situation B: Gingival margin is coronal to CEJ; CAL calculated by subtracting distance from the gingival margin to CEJ from probing depth.
Situation C: Gingival recession defect; CAL equals the sum of gingival recession measure and probing depth.
PPD VS CAL
Since gingival margin is variable (may be enlarged or may show recession), it does not help in differentiating pseudo vs true pocket.
CAL is measured from a fixed reference point, hence may provide assessment of the true attachment loss. Primarily used in diagnosis.
Periodontal therapy is aimed at restoring the gingival sulcus to a state that is easily cleansable/ maintainable. Hence probing depth is the primary determinant in treatment planning.
PROBE PENETRATION FACTORS
Influenced by
Probing force
Diameter of probe
Direction of probing
Resistance of tissue and inflammatory degree
PROBING FORCE
Optimal Probing Pressure: 0.75 N for reproducibility.
Minimal Risk for False Positives: 0.25 N as per Lang (1986).
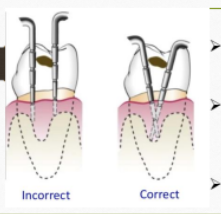
PROBING TECHNIQUE
Insert the probe at the contact point
direct towards the interproximal area.
Especially critical in posterior teeth.
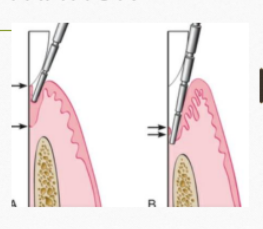
TRANSGINGIVAL PROBING / BONE SOUNDING
Probing after the site is anesthetized
Probe introduced until it reaches the bone
Done as a presurgical evaluation to assess the bone defect
FURCATION PROBING
Hamp and Lindhe Classification:
Grade I: Horizontal probing <3 mm.
Grade II: Horizontal probing ≥3 mm but not transsecting.
Grade III: Probing extends through and through.
FURCATION - CLINICAL CHALLENGES
Furcation probing measures the horizontal probing depth, while conventional probing in the furcation area measures the vertical probing depth.
Furcation involvement reduces the prognosis of the tooth.
Anatomy of furcation, along with the presence of irregularities and concavities makes it difficult to maintain.
57% of cases, furcation entrance is smaller than curette.