ACS notes
Chapter 32: Critical Care of Patients with Acute Coronary Syndromes
Learning Outcomes
Collaborate with the interprofessional team to provide high-quality care for patients with acute coronary syndromes (ACS) that affect perfusion and cause pain.
Prioritize evidence-based care for patients with acute coronary syndromes affecting perfusion.
Teach patients about lifestyle modifications to reduce modifiable and non-modifiable risk factors for acute coronary syndromes.
Educate patients and caregivers about common medications used for treating acute coronary syndromes.
Implement nursing interventions to decrease the psychosocial impact of acute coronary events, especially myocardial infarction (MI).
Apply knowledge of anatomy and physiology to provide evidence-based nursing care for patients with stable angina, unstable angina, and MI.
Utilize clinical judgment to prioritize nursing care aimed at promoting perfusion and preventing complications in patients with chest pain.
Use laboratory data, signs, and symptoms to prioritize care for patients with acute coronary syndrome.
Develop a care plan utilizing quality improvement measures for patients requiring percutaneous or surgical coronary intervention to promote perfusion.
Concepts
Priority: Perfusion
Interrelated Concept: Pain, not a pain rating 0-10
Review of Coronary Circulation
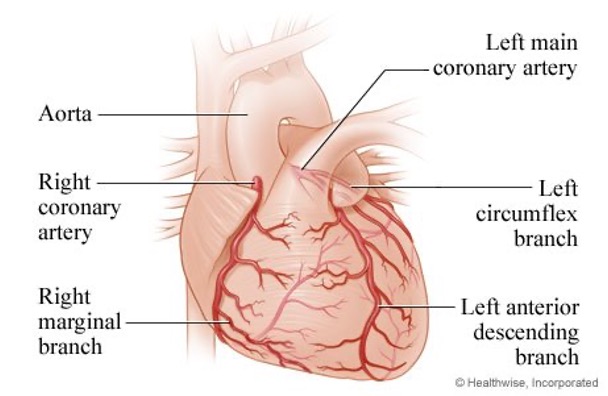
The heart perfuses itself
S/S are based on where the blockage is located
Atherosclerosis is a fat buildup that affects perfusion
Collateral circulation, arterial circulation work together to perfuse around the blockages
Patient History and Physical Examination
Assess the nature of chest pain using the OLDCARTS method:
Onset
Location
Duration
Characteristics
Aggravating factors
Relieving factors
Treatment or previous episodes
Identify potential symptoms:
Chest pain in the sternal area (described as tightness, heaviness, or pressure).
Pain may radiate to the arm, neck, jaw, shoulder, or back.
Related symptoms: Nausea, vomiting, diaphoresis, dyspnea, anxiety, fatigue, palpitations, dizziness, altered mental status.
Special attention to demographic groups (e.g., women, aging adults, diabetics)
S/S in women: indigestion, choking sensation with exertion, fatigue, SOB, anxiety
Diabetics: might have different pain, more neuropathic pain
Consider factors in the patient history:
History of coronary artery disease (CAD)
Sex/gender
Age: 17 y/o the plaque starts to build
Risk factors: diet, smoking/tobacco use, high cholesterol, lack of physical activity, HTN, diabetes
Physical Examination
Assess vital signs and cardiac rhythm.
Determine the presence of:
Jugular venous distention (JVD)
Pulmonary congestion
Heart murmurs and gallops.
Evaluate for signs of poor cardiac output or cardiogenic shock:
Hypotension, hypoperfusion (pale, diaphoresis, cyanosis)
Elevated temperature can occur with inflammation
Conduct neurologic assessment (not enough blood to the brain) and identify contraindications/allergies for antiplatelet or fibrinolytic therapy.
Obtain psychosocial assessment.
patients feed off your energy so stay calm and take deep breaths the keep you and the patient calm.
Laboratory Assessment
Troponin T or Troponin I:
Sensitive serum biomarkers for myocardial injury.
Levels rise within 2-24 hours with myocardial injury and can remain elevated for up to 14 days.
Elevations observed in myocardial infarctions, cardiac trauma, heart failure, myocarditis, and pericarditis.
Serum levels monitored every 3-6 hours up to three times to rule out myocardial infarction. Done at the bedside
Look at the rise and the fall of level to indicate an acute myocardial injury or infarction
Chronic elevated levels can be seen that is why we look at the rise and fall, not a single level.
Imaging Studies
Chest x-ray: within 30 mins and shows us the media stinum and/or lung issues
Thallium scans (nuclear stress test)
Echocardiography
Contrast-enhanced cardiovascular magnetic resonance (CMR)
CT coronary angiography (CTCA)
Other Diagnostics
ECG (EKG): priority, within 5-10 mins of arrival
Exercise tolerance test (stress test)
Cardiac catheterization (percutaneous coronary intervention)
Coronary Artery Disease (CAD): progressive
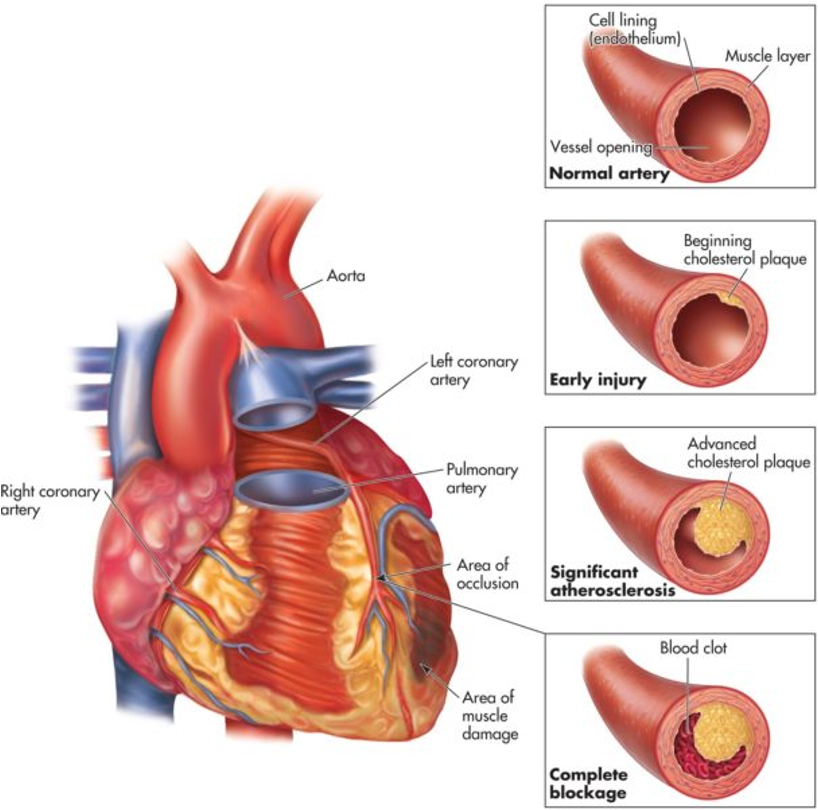
Definition: Narrowing of coronary arteries that impedes blood flow to the cardiac muscle.
Etiology: Primarily caused by atherosclerosis.
includes chronic stable angina, acute coronary syndromes.
Ischemia:
Insufficient blood/oxygen supply to meet myocardial demand.
Reversible condition.
Infarction:
Artery is significantly narrowed or completely obstructed.
Necrosis (cell death) due to lack of oxygen. Prolonged and decreased perfusion.
Irreversible condition.
Angina
Definition: "Chest pain" occurs due to a temporary imbalance between oxygen supply and heart's oxygen demand.
Precipitating Factors that increase metabolism/demand:
Physical exertion
Stress
Temperature extremes
Heavy meals
Smoking
Types of Angina
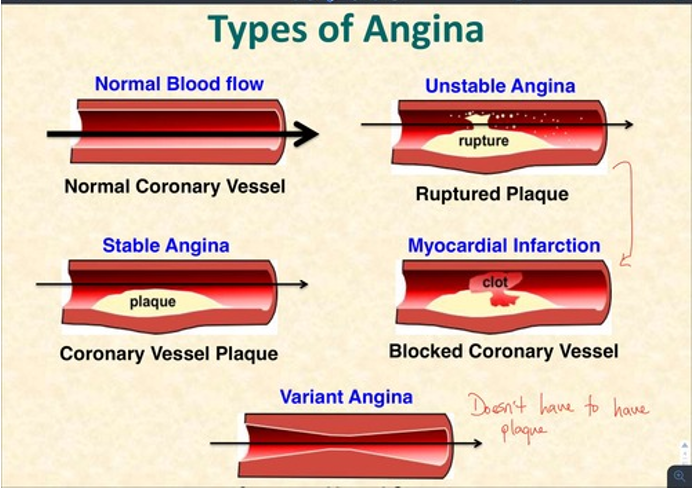
Chronic Stable Angina (CSA):
Associated with fixed (stable) atherosclerotic plaque.
Manifestations: Symptoms occur with physical activity, familiar frequency, duration, and intensity; symptoms are limited in duration (it does’t last very long).
Management: Pain relieved with rest or nitroglycerin (NTG), often managed with drug therapy such as aspirin (ASA) antiplatlet (keeps platelets from clumping together), NTG, and statins.
Acute Coronary Syndrome (ACS)
Definition: Condition resulting from the rupture of atherosclerotic plaque leading to platelet aggregation, thrombus formation, and vasoconstriction.
Types of ACS:
Unstable Angina
Acute Myocardial Infarction (AMI)
Unstable Angina
Pathophysiology: Reduced coronary perfusion due to atherosclerotic plaque rupture leading to non-occlusive (does NOT completely block the vessel) thrombus formation.
Subtypes:
New-onset angina: First episode of symptoms.
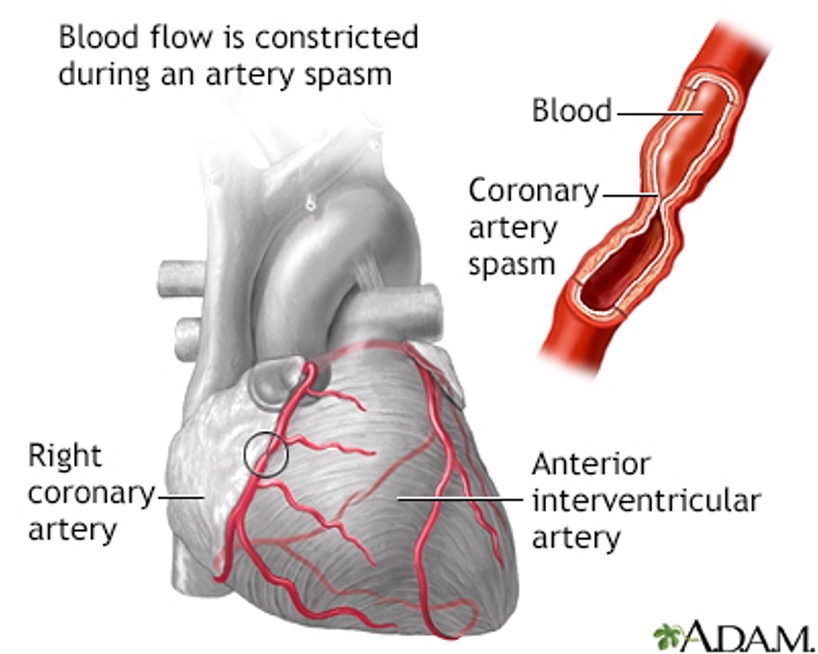
Vasospastic angina (Variant or Prinzmetal angina): Caused by vasospasm; occurs unpredictably, typically at rest.
ST segment elevation, relieved after spasm stops
Pre-infarction angina: Pain occurs days or weeks prior to a heart attack.
Manifestations can occur at rest or with exertion; the increase in episodes (attacks) correlates with greater pain intensity.
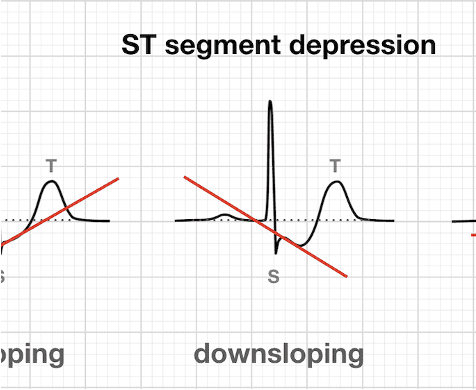
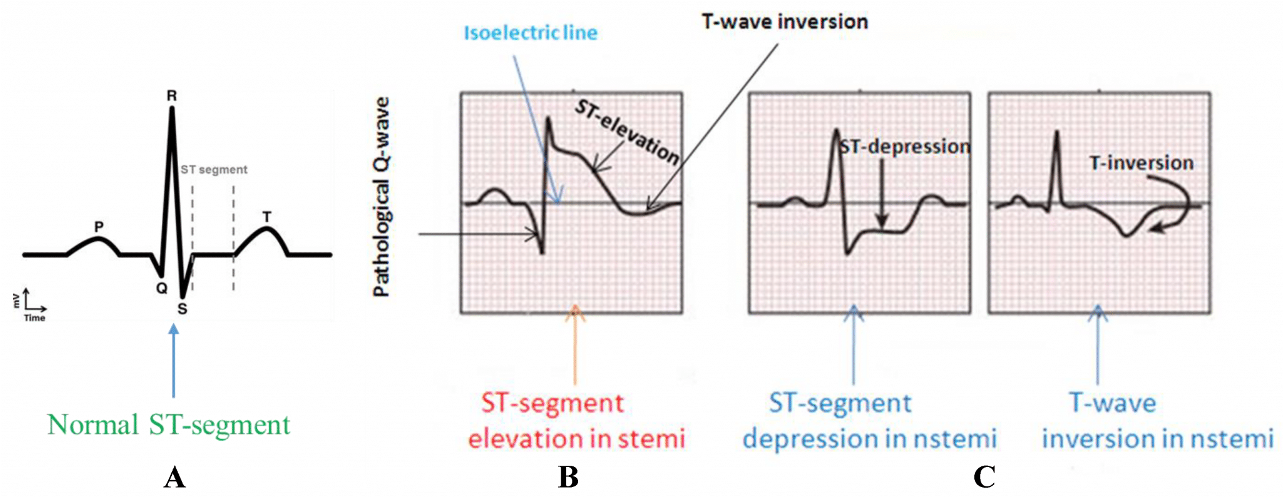
ST “changes” without elevated cardiac enzymes (troponin) present as inverted T-waves or ST segment depression.
We have ischemia showing up on the monitor
negative troponin
Myocardial Infarction (MI)
Pathophysiology: Rupture of atherosclerotic plaque results in occlusive thrombus formation leading to ischemia, injury, and then necrosis.
Types of MI:
Non-ST segment Elevation Myocardial Infarction (NSTEMI)
ST segment Elevation Myocardial Infarction (STEMI)
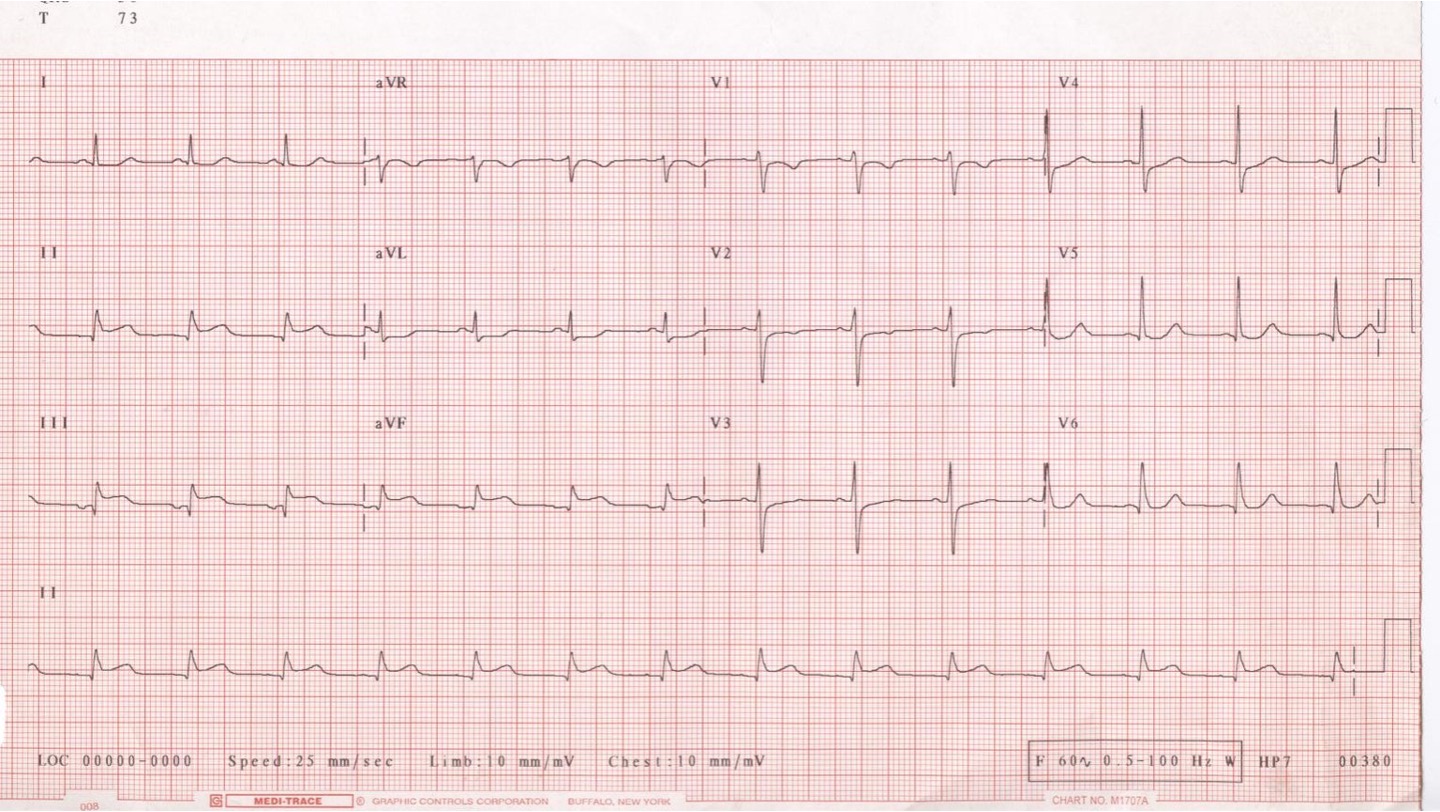
Zones of Injury:
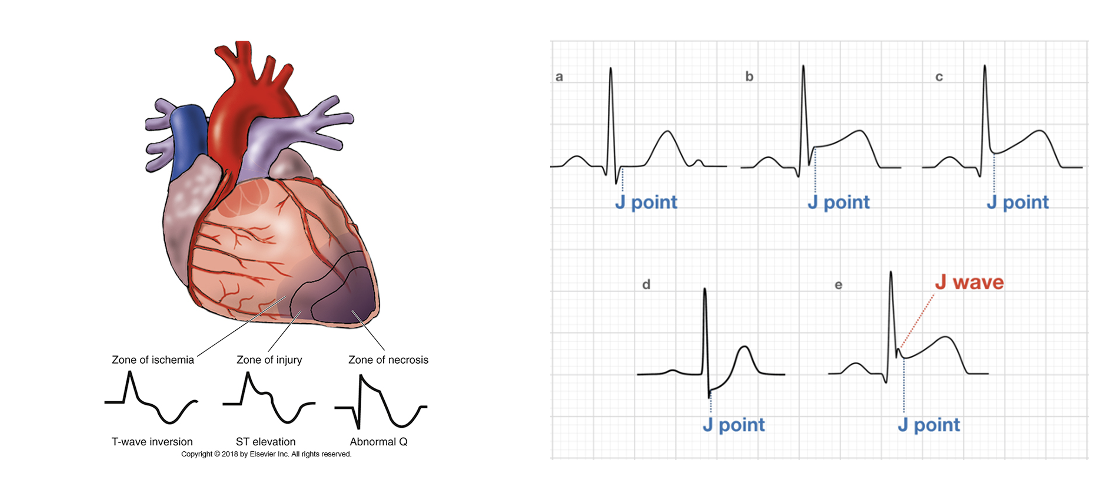
Ischemia → Infarction:
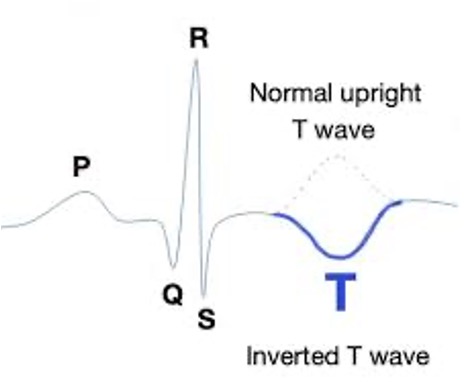
J Point: Junction between the end of the QRS complex and beginning of the ST segment.
Look at this and if it rises 1 mm it is positive for ST elevation.
ST Segment: Starts at the J point and ends at the beginning of the T wave.
T-wave: Inversion is associated with myocardial ischemia.
NSTEMI Characteristics:
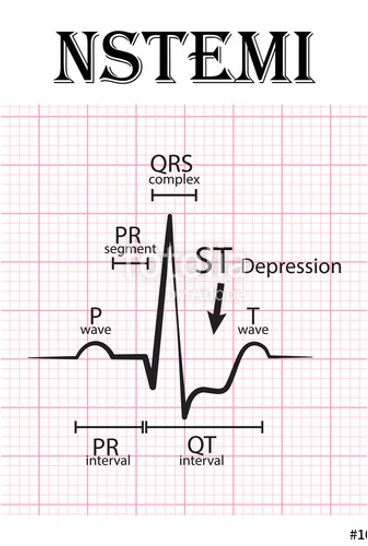
Significant sluggish blood flow or poor coronary perfusion of the myocardium
ST segment depression and/or T-wave inversion changes on 12-lead ECG.
Initial troponin levels may be normal but elevate over 3-12 hours.
The changes on ECG AND elevation in troponin indicates myocardial cell death
Myocardial damage does not extend through the ventricular wall.
STEMI Characteristics:
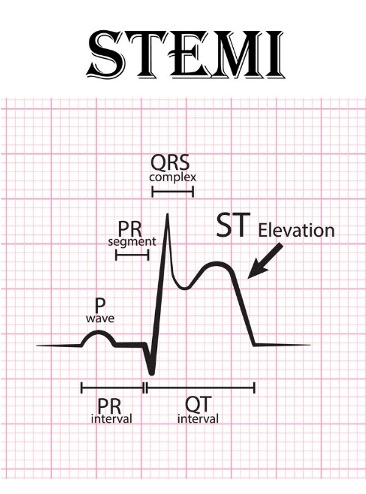
New ST elevation at the J point in at least two contiguous leads (leads that are clumped together looking at one specific part of the heart) of more than .
Elevated troponin levels; signifies 100% occlusion of coronary vessels.
full thickness of the heart muscle
MEDICAL EMRERGENCY!
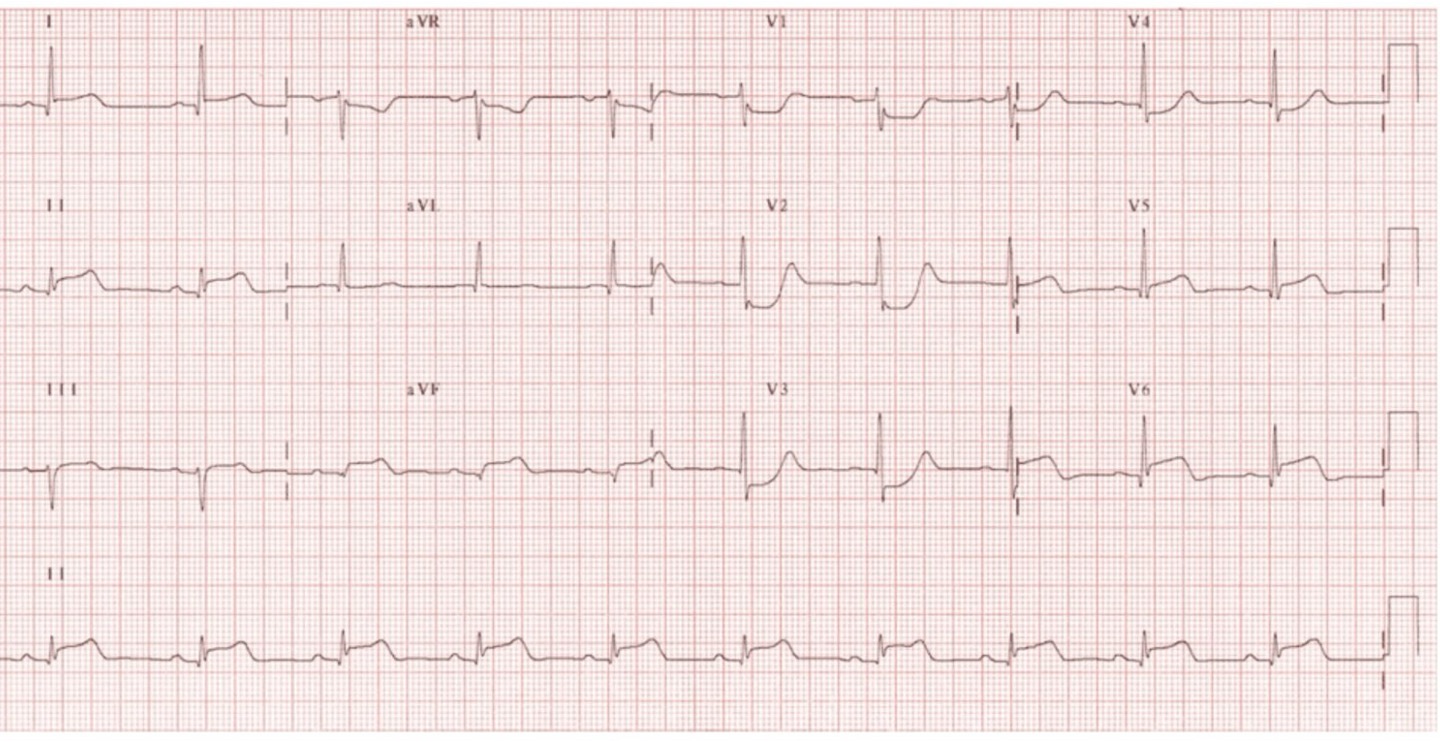
ECG Interpretation
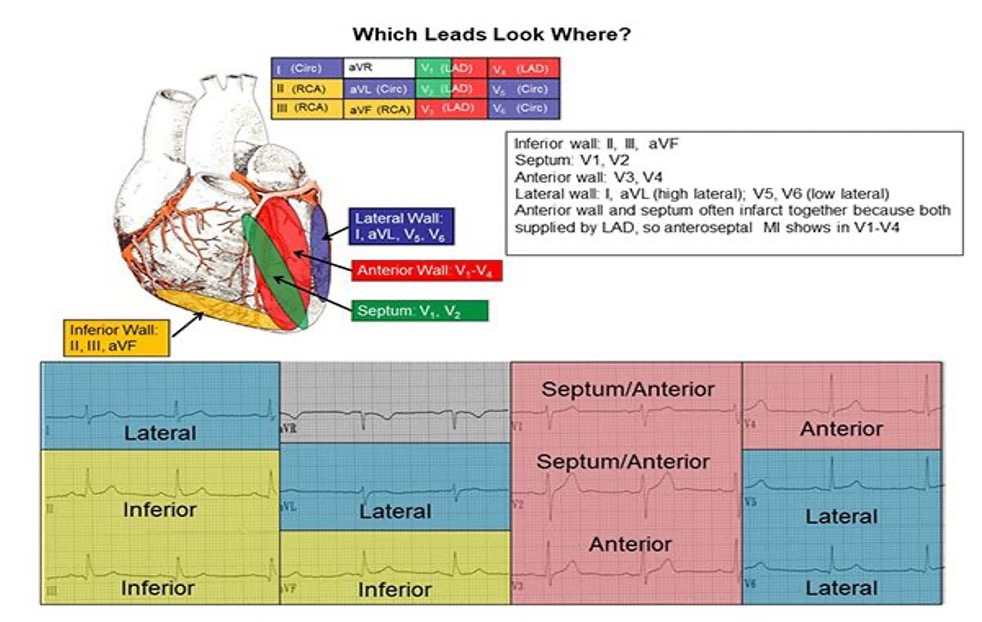
Contiguous Leads: Grouped leads that provide views of specific ischemic or infarcted sections, including:
Inferior leads: II, III, aVF
Lateral leads: I, aVL, V5, V6
Septal leads: V1, V2
Anterior leads: V1, V2, V3, V4
2 or more contiguous leads needed for positive
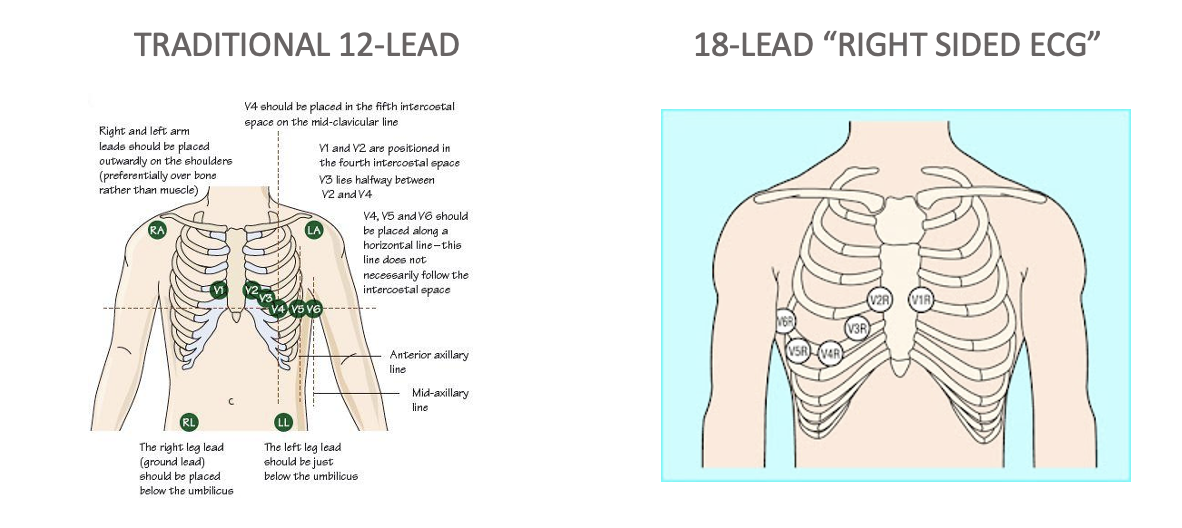
18-Lead: used to see ischemia, make sure this is labeled as such
Ventricular Remodeling Process
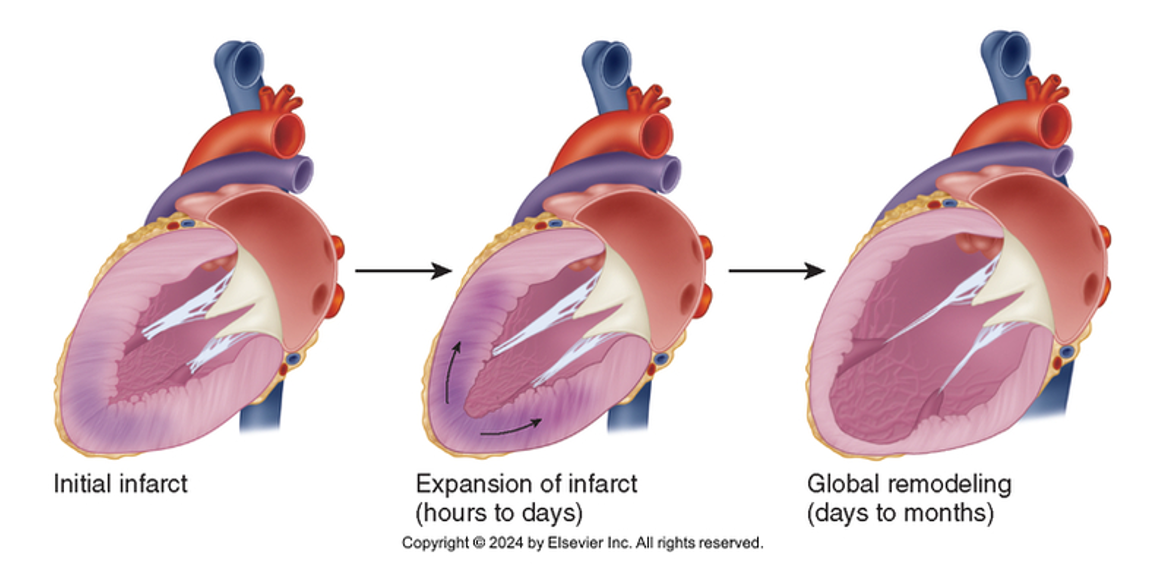
Pre-MI Stage: Healthy structure with no symptoms of heart failure (HF) but high risk factors.
Early MI Stage: Infarct expansion occurs within hours to days post-event.
Late MI Stage: Global remodeling take place.
Analysis: Hypothesis Prioritization
Acute pain related to imbalance between myocardial oxygen supply and demand.
Decreased myocardial tissue perfusion due to interruption of blood flow.
Potential for dysrhythmias due to ischemia and ventricular irritability.
Risk for heart failure due to left ventricular dysfunction.
Planning and Implementation
Managing Acute Pain
Expected Outcome: Patient verbalizes reduced pain due to improved perfusion.
Interventions:
Comfort positioning
Minimize patient movement
Provide a calm and quiet environment
Focus on decreasing pain
Decrease myocardial oxygen demand
Increase perfusion
Drug Therapy Options:
Administration of Oxygen when required (don’t give supplemental oxygen unless needed O2 sat of <90 starting at 4L titrating down)
Nitroglycerin (NTG) Sublingually:
Increases collateral blood flow, redistributes blood flow toward the subendocardium, dilates coronary arteries, and decreases myocardial oxygen demand by reducing preload and afterload.
Administration Protocol:
Assess pain and vital signs (every 5 mins); ensure adequate CO and hemodynamic stability.
HOLD if systolic is <90 or <30 below baseline, HR <50 or >100, NO pain
Ask if taken phosphodiesterase inhibitor in last 12-48 hours (contraindicated)
Administer every 3-5 minutes SL up to 3 doses ONLY
Titrate effect of NTG
Teaching: might tingle or burn, don’t put in the light, needs to be replaced every 6 months, if not relief after 3rd dose call 911, might cause dizziness or HA
Morphine IV Push:
Used if the patient is unresponsive to NTG; provides pain relief and decreases myocardial oxygen demand, also relaxes smooth muscle and reduces catecholamines (adrenaline). use caution with older/younger patients
Increasing Myocardial Tissue Perfusion
Expected Outcome: Achieve adequate cardiac output, normal sinus rhythm, and maintain vital signs within normal limits.
Interventions: Focused on restoring perfusion to the injured area of the heart;
Drug Therapy: Includes:
Antiplatelet Therapy: aspirin 325mg or 4 baby aspirin chewed up
Do NOT give with allergy or past GI bleeding (can give rectally if so)
Anticoagulation Therapy: Heparin
Antihypertensives:
Beta blockers
decreases workload of heart
reduced occurrence of ventricular dysrhythmias
ACE inhibitors or Angiotensin receptor blockers (ARBs)
given within 48hrs to ACS with evidence of HF
reduces chance of ventricular remodeling
Calcium Channel Blockers)
promotes vasodilation and myocardial perfusion
used in chronic stable angina and coronary vasospasm
Statin Therapy
Reperfusion Therapy through Fibrinolytics (Thrombolytic agents) IV:
Clot buster, lise the clot and keeps the coronary artery perfusing
used for ST elevation or MI
Includes agents like tissue plasminogen activator (tPA, alteplase), Reteplase (activase), and Tenecteplase (TNK) for STEMI patients that cannot undergo timely percutaneous coronary intervention (PCI).
PCI best option for patients
Requires administering within 12 hours of symptom onset with ST elevation AND if PCI is unavailable within 90 minutes of first medical contact.
Onset of symptoms within the prior 12 hours and ECG findings consistent with true posterior MI.
Doors to Needle time must be within 30 minutes from ED arrival or onset of chest pain.
Contraindications for Fibrinolytics (Thrombolytics)
Do not give: patients who present more than 24hrs after the onset of symptoms, ST segment depression, unless a true posterior MI is suspected, the is an absolute contraindication
Absolute Contraindications:
Prior intracranial hemorrhage
Known structural cerebral vascular lesion
Known malignant intracranial neoplasm
Ischemic stroke within 3 months except for acute ischemic stroke within 3 hours
Suspected aortic dissection
Active bleeding or bleeding disorders
Significant closed-head or facial trauma within 3 months
Relative Contraindications:
Severe uncontrolled chronic hypertension at presentation
History of chronic severe hypertension (SBP >180)
History of ischemic stroke within the past 3 months, dementia
Trauma or prolonged (>10mins) CPR recently or major surgery (within 3 weeks)
Recent (within 2-4 weeks) internal bleeding
Pregnancy
Peptic ulcer disease
Current use of anticoagulants
Noncompressible vascular puncture
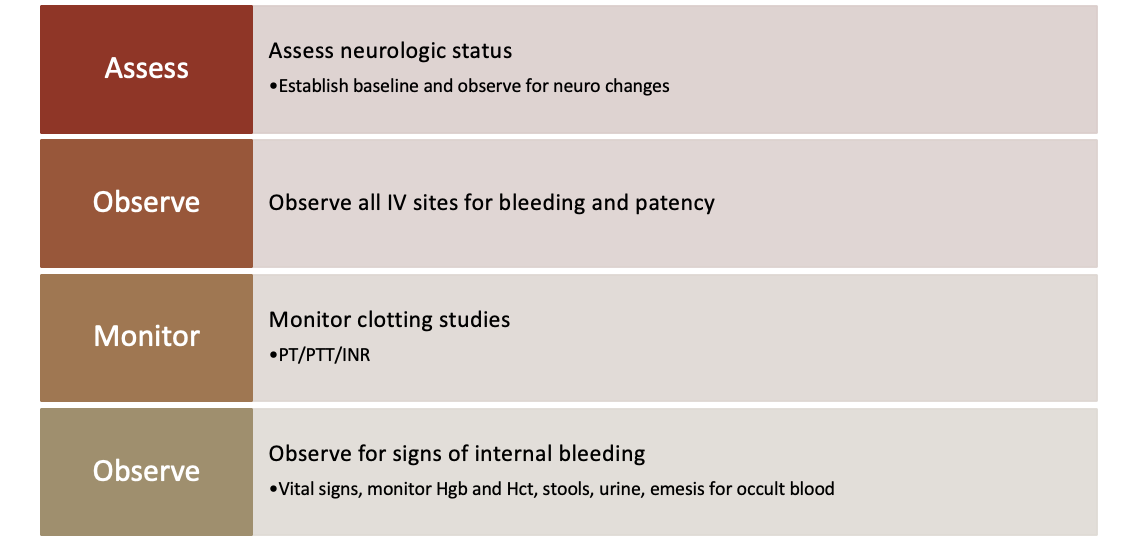
Monitor for Effectiveness of Fibrinolytic
Indications the clot has dissolved, and the artery is re-perfused
Abrupt cessation of pain or discomfort
Sudden onset of ventricular dsyrhythmias
Resolution of ST segment depression/elevation or T wave inversion
A peak at 12 hours of markers of myocardial damage
Indication of re-occlusion
Return of chest pain/discomfort or previous symptoms’
Worsening or return of ST segment elevation
Report Immediate Indications of Bleeding
Percutaneous Coronary Intervention (PCI)
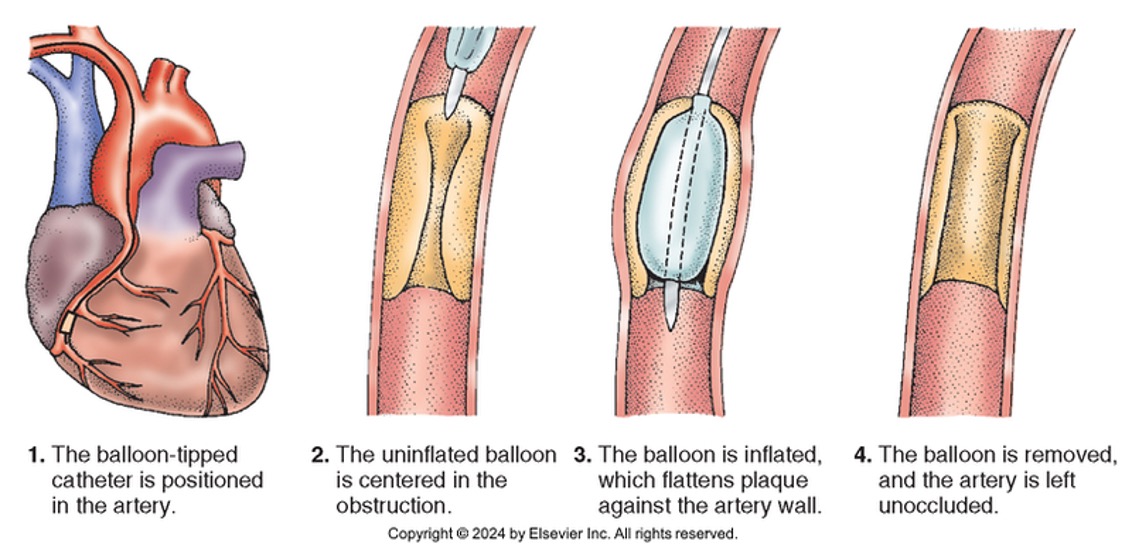
Aim to restore blood flow to obstructed areas through a percutaneous procedure.
Goals: Door to balloon time within 90 minutes for STEMI patients.
Assess (allergies, Hx)
allergy to contrast dye
kidney function
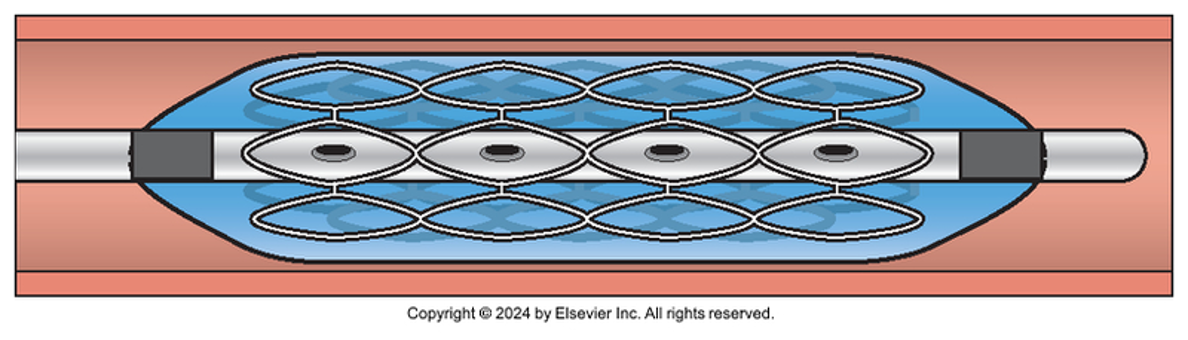
Types of interventions:
Atherectsomy
Angioplasty with stent placement
Post-Procedure Monitoring: Check for:
Acute vessel closure
Bleeding
Reactions to contrast dye
Hypotension and hypokalemia
Dysrhythmias
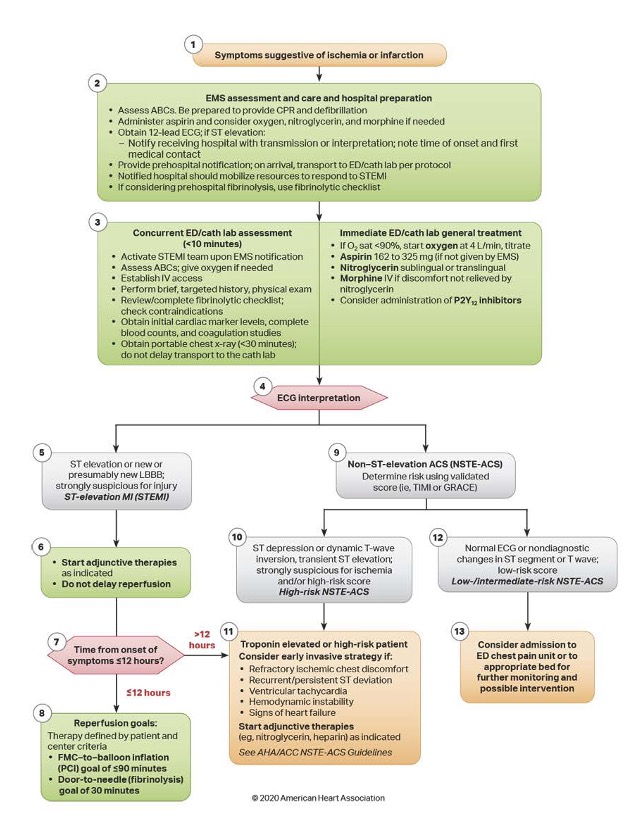
ACLS: Acute Coronary Syndrome Algorithm
Identifying and Managing Dysrhythmias
Desired Outcome: free of dysrhythmias or identify and manage early to prevent complications.
Interventions & Monitoring:
Identify dysrhythmias
bradycardias often linked to ischemia or AV node
ventricular irritability
Assess hemodynamic status
treat if compromised or if increased myocardial oxygen requirements
Evaluate for discomfort
Coronary Artery Bypass Graft (CABG) Surgery
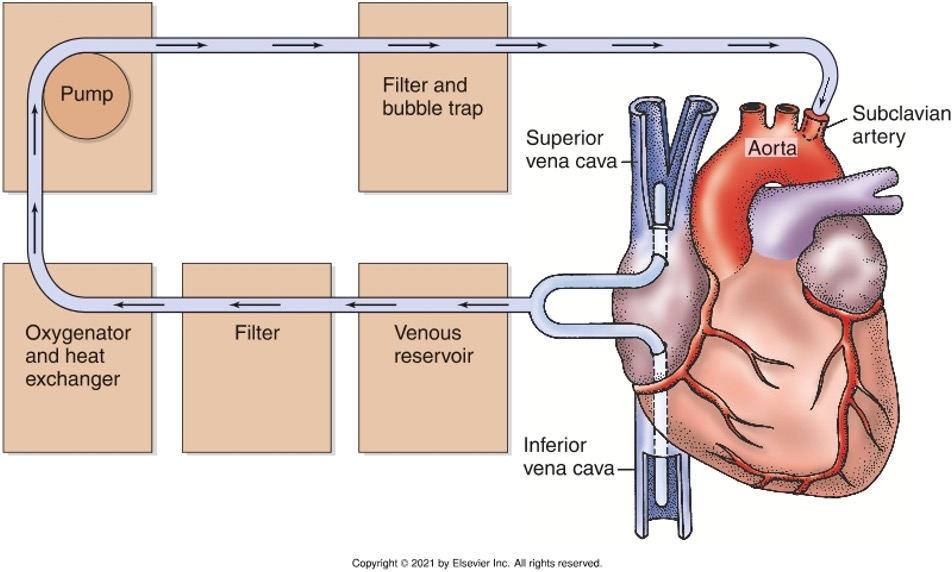
Definition: Surgical procedure where occluded coronary arteries are bypassed.
Candidates for CABG:
Angina with over 50% occlusion of the left main coronary artery that cannot be stented.
Unstable angina due to severe 2-vessel disease or occlusion.
Moderate 3-vessel or small vessel disease.
Any vessel unsuitable for PCI.
Heart failure or valve disease.
Acute MI with cardiogenic shock.
Ischemia or impending MI after angiography for PCI
Preoperative Care
Confirm allergies, perform diagnostic tests, type and cross-match blood supplies, and review medications.
Prepare for physical procedures like incisions, ETT/ventilators, chest tubes, endotracheal tubes, urinary catheters, and pacemaker wires.
Educate the patient about splinting incisions, deep breathing exercises, expected pain, and early ambulation, arms/leg exercises, anxiety id common.
Postoperative Care
Implement sterile technique for dressing changes and connect mediastinal tubes to water-seal drainage systems.
Monitor heart for signs of dysrhythmias/ pacer wires, manage them, and report any identified CABG complications such as:
Fluid and electrolyte imbalance and perform frequent checks on serum electrolytes.
edema is common
serum electrolytes may be low
check frequently
Hypotension and conditions that compromise cardiac output.
r/t collapsed coronary graft, hypovolemia, or vasodilation
report to provider if pt activity includes
decreased SBP >20
20 beats/min change in HR
c/o dyspnea, chest pain
Hypothermia management protocols at temperatures below 96.8°F.
re-warm at a rate no faster the 1.8 degrees F/hr
promotes vasoconstriction and HTN
Hypertension
SBP >140-150
promotes leakage for suture lines and increased bleeding
CABG Complications Monitoring
Bleeding: expected, measure drainage at least hourly, report if over 150mL/hr or abrupt cessation of previously heavy drainage
Cardiac Tamponade: Check for Beck's Triad symptoms including hypotension, JVD but clear lung sounds, and distant but muffled heart sounds.
Neurological Assessments: Post-anesthesia monitoring and frequent checks (every 30-60 mins) until anesthesia is warn off then every 2-4 hrs. increased transient neuro deficits in older adults.
suspected stroke if: abnormal pupillary response, failure to waken, seizures, absence of sensory or motor fucntion.
Anginal Pain: Any sternotomy-related pain is expected, but new anginal symptoms may indicate graft failure.
Sternal Wound Infection: Check for postoperative fever, bogginess, redness, and drainage from suture sites.
Care Coordination and Transition Management
Post-Discharge Considerations:
Ensure the patient has support and is not alone.
Assess availability of cardiac rehabilitation and home health services.
cardiovascular function
coping skills
functional ability
nutritional status
patient understanding of illness and treatment
Conduct education on:
Risk factor modification
Complementary and Integrative Health practices
Management of sexual activity post-CABG.
Drug therapy
Healthcare Resources: Include mentioning organizations like the AHA and Mended Hearts for patient support.
Evaluation: Expected Outcomes
Patient states that pain is alleviated.
Adequate myocardial perfusion is established.
Patient remains free of complications such as dysrhythmias and heart failure.