Week 6: Testicular Torsion
Learning Objectives
Types of Torsion:
Describe and differentiate between different types of testicular torsion.
Clinical Symptoms:
List the common clinical symptoms related to torsion.
Ultrasound Appearances:
Identify and describe the ultrasound appearances characteristic of testicular torsion.
Differentiation:
Differentiate between testicular torsion and epididymo-orchitis in patients presenting with acute scrotal pain.
Definition of Testicular Torsion
Testicular torsion occurs when the testis twists around the spermatic cord, cutting off its blood supply.
It is a surgical emergency requiring intervention within 6 hours to prevent ischemia and potential necrosis.
Initial presentation includes acute pain and swelling; twisting causes ischemia due to reduced blood flow.
Doppler Ultrasound is typically used to demonstrate decreased blood flow to the affected testis.
Types of Testicular Torsion
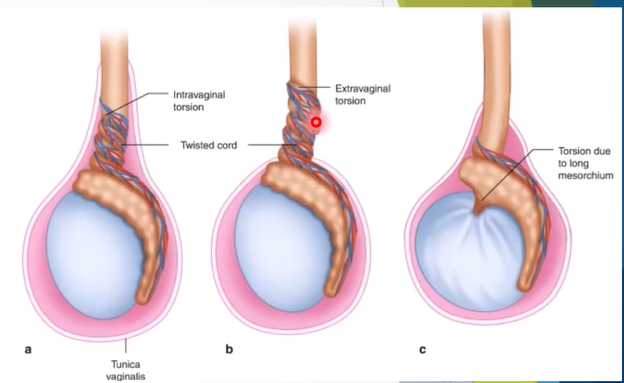
Extra-vaginal Torsion:
Occurs in neonates.
Torsion occurs at the external ring level.
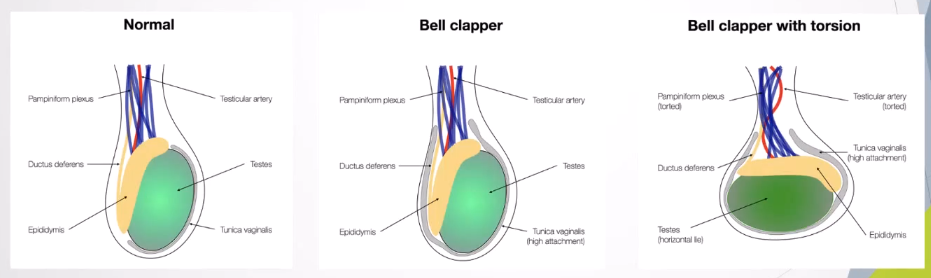
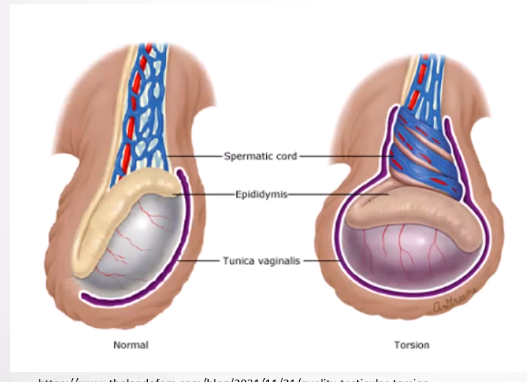
Intra-vaginal Torsion:
Most common in adolescents and young adults.
Linked to the bell-clapper deformity, enabling abnormal twisting of the spermatic cord due to high attachment of tunica vaginalis.
Cryptorchidism-related Torsion:
Associated with long mesorchium, associated with cyrtochism
Pathophysiology
Initially only venous outflow is obstructed, increasing intratesticular pressure.
With the increase in time and twisting greater than 360 degrees, arterial flow becomes impeded, leading to ischemia and potential necrosis.
Extravaginal torsion: whole hemiscrotum and its contents rotate around the spermatic cord at the level of the external ring
Intravaginal torsion: due to the bell-clapper deformity, the abnormally high attachment of the tunica vaginalis to the spermatic cord allows the testis and epididymis to move more freely, making it more likely to twist around the spermatic cord
Clinical Presentation
Onset of acute pain, often without trauma.
Physical signs include:
Swollen or red hemiscrotum.
Elevated testis.
Absence of cremasteric reflex.
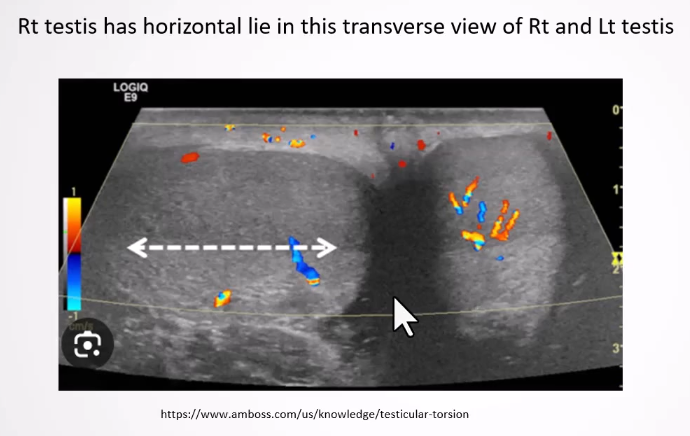
Transverse lie of the testis.
Anterior rotation of the epididymis.
Successful manual detorsion may relieve pain.
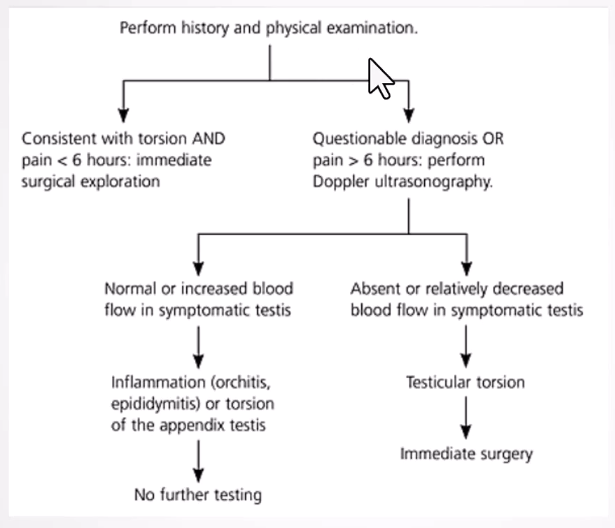
Diagnosis
Testicular torsion is a medical emergency; rapid diagnosis is crucial.
Physical examination is primary; ultrasound is used when uncertainty exists due to time constraints.
Doppler ultrasound assesses blood flow to differentiate conditions.
Treatment
Key: Rapid diagnosis and surgical intervention are critical.
Early diagnosis allows for possible de-torsion with minimal damage.
Manual detorsion may be attempted if surgery isn't immediately available.
Contralateral orchidopexy may be performed to prevent recurrence.
In cases of testicular necrosis, orchidectomy is required, potentially followed by prosthesis placement 4-6 months post-surgery.
Outcomes
Salvage rate is nearly 100% if treated within 6 hours; declines below 50% if treatment is delayed beyond 12-24 hours.
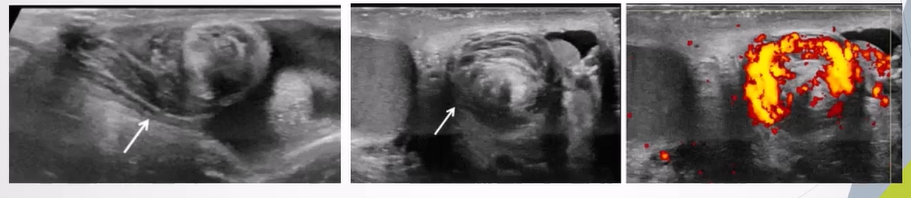
Ultrasound Appearances
Twisting of Spermatic Cord:
Identified by the "whirlpool sign" indicating torsion.
Whirlpool sign - spiral twist in the spermatic cord seen in the external inguinal ring or in the scrotal sac.
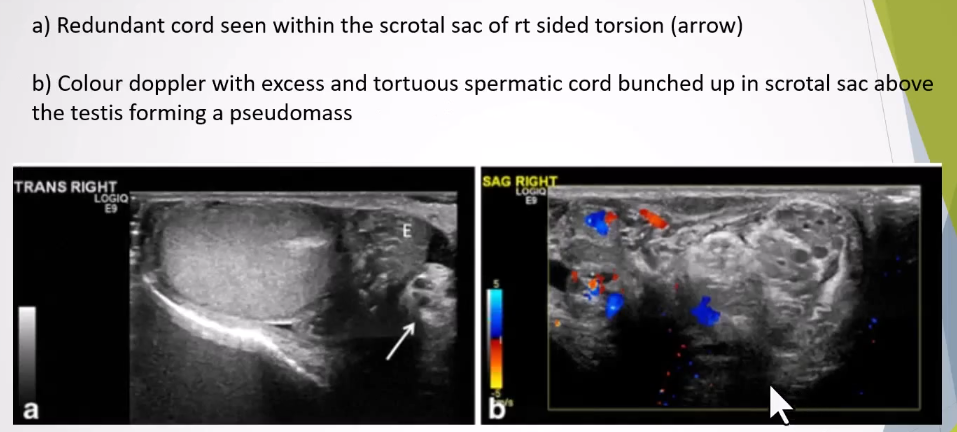
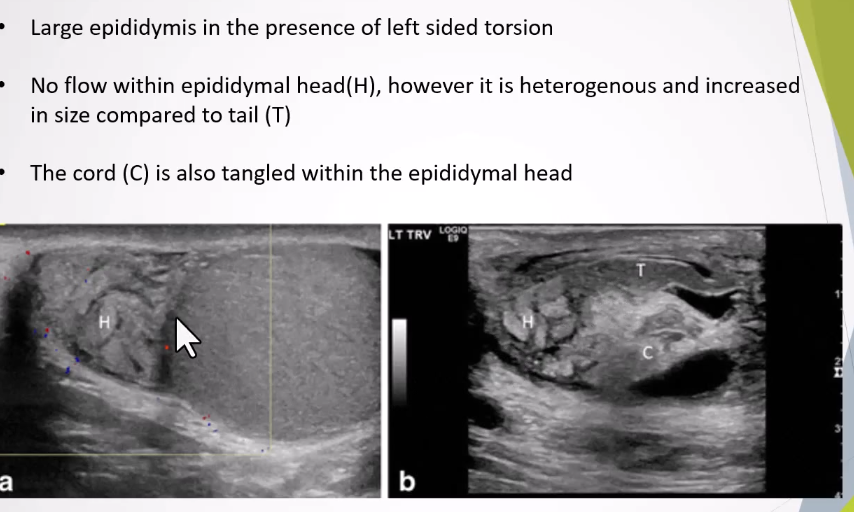
Redundant Spermatic Cord:
Presence of excess and tortuous spermatic cord in the scrotal sac is a sign for the anomalous attachment of the tunica vaginalis
Bunched up cord appears as an ovoid heterogeneous mass with excessive twisting.
Can appear to include dilated anaechoic tubules representing congested vessels within the knot or mass
Can still have flow withn if partially twisted
Horizontal or Altered Lie:
Testes typically are vertical; a horizontal or oblique lie signifies improper attachment.
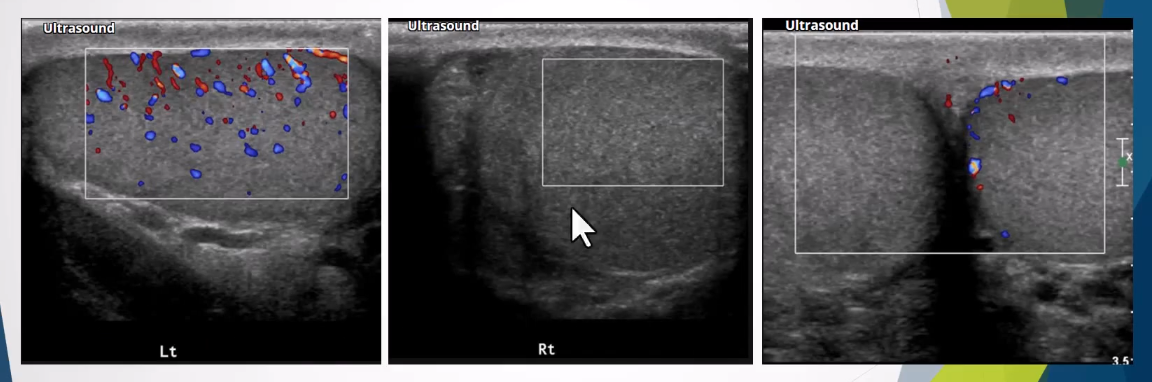
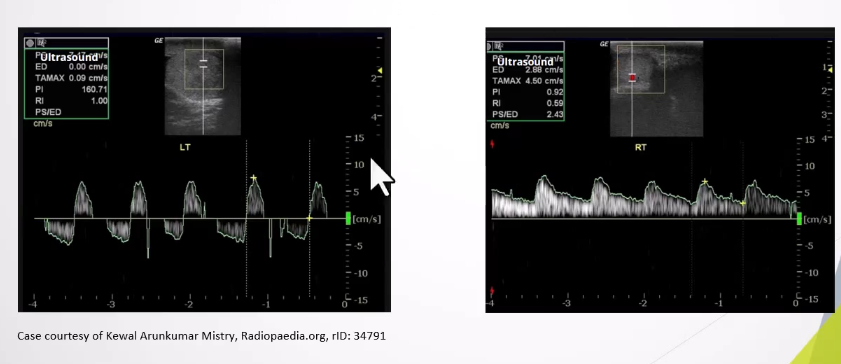
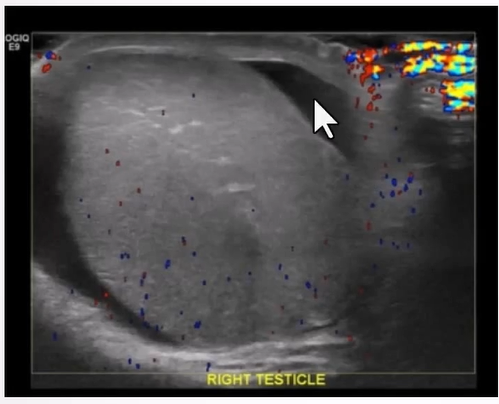
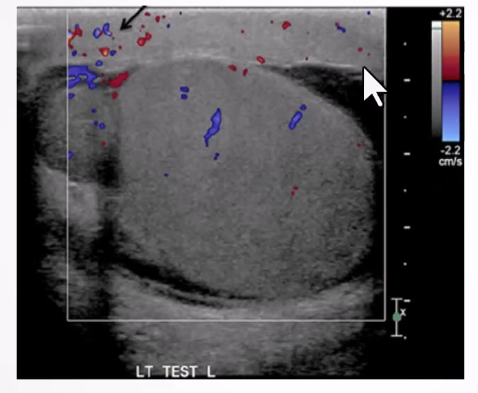
Altered Blood Flow:
Intratesticular arteries characteristically have a low resistance pattern with a mean resistive index of 0.62 (range 0.48 - 0.75)
Incomplete torsion - reversal of distolic flow and RI >0.75
Complete torsion - absence of blood flow in both the testis and epididymis
.
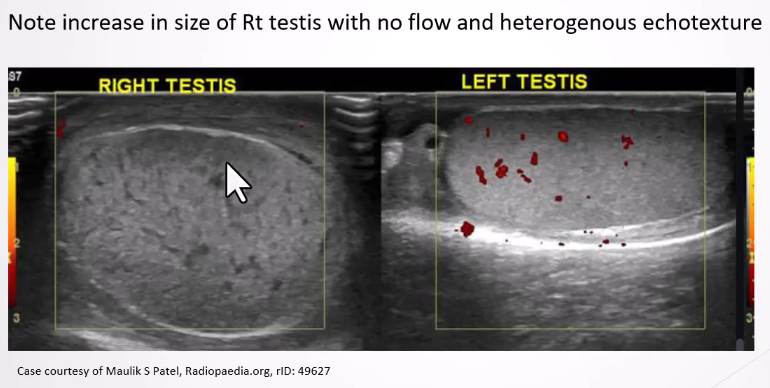
Increased Size of Testis/Epididymis:
Changes in echotexture based on timing post-torsion (homogeneous in early stage, heterogeneous after 24 hours due to necrosis).
Reactive Hydrocele
Scrotal Skin Thickening:
Reactive thickening of the scrotal skin with hyperemia and increase flow on colour doppler
Differential Diagnosis of Acute Scrotal Pain
Testicular Torsion.
Epididymo-orchitis (most common).
Incarcerated hernia.
Torsion of the appendix testis.
Summary of Differentiating Features
Testicular Torsion: Sudden onset, often high-riding and transverse alignment of the testis; absent cremasteric reflex.
Epididymitis: Gradual onset, fever common in advanced cases, typically normal alignment of the testis, present cremasteric reflex.
Appendage Torsion: Localized swelling at the testicular head, rarely high-riding, sudden or gradual pain.