8.5 - Hepatobiliary System
LECTURE NOTES
Two lobes - falciform ligament down the middle
Blood supply by both hepatic artery and portal vein
Outflow contains bile and blood (leaves by 3 hepatic veins)
Right, middle and left hepatic vein
Two lobes of kidney divided by middle hepatic vein (which sits further left on image than the falciform ligament)
Liver is divided into segments - left has segments 1-4 and right hsa segments 5-8
Liver technically curls around your body - right posterior section is around your back
Hepatic lobule
Hexagonal structural unit
Sensor of each lobule has a central vein → connects blood from hepatic sinusoids → hepatic vein → systemic veinous system
Each lobule has numerous rows of hepatocytes - each has a sinusoid facing side and bile canaliculi-facing side
Portal triad
Branch of hepatic artery - brings oxygen rich blood into the liver to support hepatocytes increased energy demands
Branch of portal vein - mixed venous blood from GI Tract containg nutrients, bacteria and toxic and spleen containing waste products come.
Hepatocytes process nutrients, detoxift blood and excrete blood
Bile duct - bile produced by hepatocytes drains into bile canaliculi → coaelsce with cholangiocyte-lined bile ducts around lobule perimeter
Three zone model
Blood into hepatic acinus via Point A
Blood drains out of hepatic acinus via Point B
Zone 1 - high oxygen and high toxin risk
Zone 2 - medium oxygen and medium toxin risk
Zone 3 - low oxygen and low toxin risk
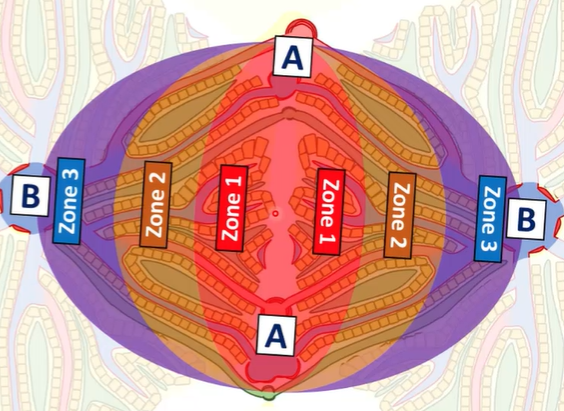
Hepatic Acinus
Functional unit of liver
Consists of two adjacenet 1/6th hepatic lobules - sharing 2x portal triads and extend into hepatic lobules as far as the central vein
Acinus ais made up of three zones…
Liver cell types
Sinusoidal endothelial cells
No basement membrane
Fenestrated - discontinuous endothelium
Allow lipids and large molecule movement to and from hepatocytes
Kuppfer cells
Sinusoidal macrophages
Attached to endothelial cells
Phagocytosis
Hepatic stellate cells
Exist in a dormant state
Essentially fibroblasts which get activated in response to liver damage
Store vitamin A in liver cytosolic droplets
Proliferate, chemotactis and deposit collagen in ECM
Hepatocytes
80% of liver mass
Cubical shaped
Syntehsise albumin, clotting factors and bile ssalts
Recieve nutrients and building blocks from sinusoids
Drug metabolism
Cholangiocytes
Secrete bicarbonate and water into bile
Hepatocyte functions - numerous including:
Metabolic and catabolic: synthesise and utilise carbs, lipids and proteins
Secretory and excretory functions: synthesis and secretion of proteins, bile and waste products
Detoxification and immunological functions: breakdown of ingested pathogens and processing of drugs
Carbohydrate metabolism: glycolysis, glycogenesis, glycogenolysis, gluconeogenesis, lipolysis and lipogenesis
Glucose undergoes glycolysis to produce pyruvate
Pyruvate enters TCA cycle to produce more ATP
Oxygen is rate-limiting and therefore pyrvate is fermented to lactate
Lactate is reconverted into pyruvate in the liver
Gluconeogenesis of pyruvate which can be metabolised
This is known as the cori cycle
Protein Synthesis
Amino acids go
Synthesis of non-essential Amino Acids
Process known as transamination
Alanine shuttled to liver and amide moved to alpha keto glutarate
Forms glutarate and pyruvate
Transamination - differnt keto acids can be converted into multiple amino acids depending on the transaminase enzyme, which are vital for the production of non-essential amino acids)
Examples…
Glucose-alanin cycle - deamination
One method of gluconeogenesis
One problem is the msucle can potentially utilise the amino acids to produce gllucose to release energy
But…
Conversion of pyruvate to glucose requires energy
Nitrogen removal as urea requires energy
Solution…. transfer problem to liver for the glucose- alanine cycle
Pyruvate from glycolysis and glutamate
Glutamate transfers amine to pyruvate
Alanine forms and is formed and shuttled to liver
At the liver alanine broken down to pyruvate
Amine transferred back to alpha ketoglutarate to form glutamate
Amine taken off to form urea
Pyruvate used to produce glucose → shuttled back to muscle cell for glycolyssi
Triglyceride metabolism
Triglyceride conversion into fatty acids
Fatty acids shuttled to liver
Beta oxidation of fatty acids to acetyl CoA
Acetyl CoA enters the TCA cycle
Lipoprotein Synthesis
Glucose taken into the liver can be converted to glycerol, fatty acids (via malnoyl coA or cholesterol by HMG CoA reductase)
Glycerol and fatty acids forms triglycerides
Add phospholipids or apoproteins or cholesterol to form lipoproteins
Lipoproteins used as VLDL to transport fatty acids to tissues
At tissues fatty acids are converted to tri-glycerides
Lipoproteins can also form HDL - which is empy and picks up excess cholesterol
LDL formed from VLDL to transport cholesterol to tissues
Hepatocyte Storage Functions
Fat soluble vitamins (A, D, E, K)
Stores sufficient 6-12 month except Vitamin K where store is small)
Vitamin K is essential for blood clotting
Storage of iron as ferritin
Available for erythropoesis
Detoxification
Anything that is not produced by the body and shouldn’t be there is removed
P450 enzymes
Phase 1 - modification - become mor hydrophilic
Phase 2 - conjugation - attach water soluble side chains to make it less reactive.
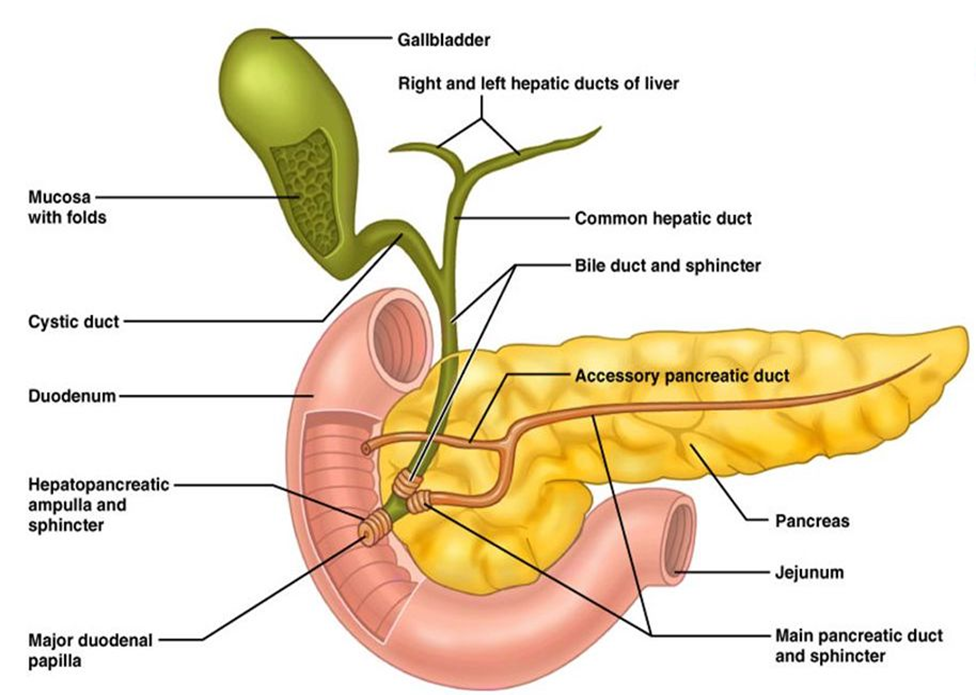
Biliary System:
Bile is mainly composed of water
Small amount of bile salts present
Uses of bile are:
Cholesterol homoeostasis
Absorption of lipids and lipid soluble vitamins
Excretions of xenobiotics, cholesterol metabolites, adenocorticoids and other steroid hormones, alkaline phosphatase
Hepatocytes secrete 60% of total bile
Primary secretion - bile secertions reflect serum concentrations
Secretion of bile salts (acids), lipids and organic ions
Cholagniocytes secrete 40% of total bile
Alteration of pH
Water drawn into bile by osmosis via paracellular junctions
Luminal glucose and organic acids reabsorbed
Bicarbonate and chloride actively secreted into bile by CFTR
IgA is exocytos
Bile flow
Biliary excretion of bile salts and toxins performed by biliary transporters
Main transporters include:
Basolateral membrane (importing)
OATPS - bile salt uptake (organic anion transporting peptide)
NTCP - bile salt uptake (sodium taurocholate-cotransporting polypeptide)
Apical surface (exporting)
Bile salt excretory pump (BSEP) - active transport of bile acids into bile
MDR related proteins (MRP2 & MRP3) - negatively charged metabolites
Products of multidrug resistance genes
MDR1→ excretion of neutral and positive xenobiotics and cytotoxins
MDR3 → phospatidylcholine
Bile salts
Main component is bile acids
Bile acids syntehsised from cholesterol
Sodium and potassium salts of bile acids connjugated in liver to glycine and taurine
2 primary bile acids are synthesised in the liver
Cholic acid and chenodeoxycholic acid
These can be converted to secondary acids by gut bacteria
Cholic → deoxycholic
Chenodeoxycholic → Lithocolic
Bile salts function
Reduce surface tension of fats
Emulsify fat prior to its digestion and absorption
Bile salts form Micelles
Steroid nucleus planar has 2x faces (amphipathic)
1x surface hydrophilic
Regulation of bile flow and secretion
Between meals sphincter of Oddi is closed
When you eat, the sphincter relaxes and it opens allowing bile to flow through
Gastric contents enter duodenum causing release of cholecytsokinin which causes gall bladder to contract
Enterohephatic circulation
95% of bile salts are reabsorbed from the terminal ileum
Na+/bile co-transport system
5% converted into secondary acids in the colon
Deoxycholic acid is reabsorbed
99% of lithocolic acid excreted in stool absorbed B. salta back to liver and re-excreted in bile.
Gall Bladder Functions
Gall bladder stores and concentrated bile and acidifies it
Gall bladder contraction is triggered by CCK
CCKA receptors and neuronal plexus of GB wall (innervated by preganglionic parasympathetic fibres of vagus nerve)
Bilirubin
Free bilirubin is insoluble and a yellow pigment
75% from haemoglobin breakdown, 22% from catabolism of other haemoproteins and 3% from ineffective BM erythropoiesis
Free Bilirubin is bound to albumin in the blood
Most dissociates in liver and enters hepatocytes
BR conjugated with 2x molecules of UDP-glucoronate → bilirubin diglucuronide
Secreted ACROSS concentration gradient into biliary canaliculi → Gastrointestinal tract
200-250mg of BR excreted into bile/day
85% in faeces
BR → urobilinogen → stercobilinogen → stercobilin
15% enters enterohepatic circulation
BR → deconjugated → lipophilic form
Urobilinogen and stercobilinogen
1% enters systemic circulation and is excreted by kidneys
Jaundice
Post-hepatic jaundice - known as obstructive jaundice