Obstetric Emergancies
Post partum Haemorrhage (PPH)
PPH - is blood loss of 500 mls or more and/or clinical signs of hypovolemic shock
Primary - within 24 hours
Secondary - 24 hours to 6 weeks following birth
A major PPH is blood loss of 50% of the blood volume within 3 hours of birth
Causes of haemorrhage
Tone (70%) Responsible for majority of haemorrhages
Trauma (20%) Perineal or cervical tears
Tissue (9%) Retained products (placental tissue or clots)
Thrombin (1%) Coagulopathy (haemophilia/warfarin)
Plan
Lie Flat
High flow O2 (15L)
Massage uterus - cupped hand circling on the umbilicus (expel clots and ‘rub up a contraction’)
???? Bimanual compression
Insert x 2 16G cannula – Consider 1-2 litres IV fluids.
Vital signs – Respiratory rate, pulse, BP, O2 Sats
Consider - Syntometrine, Misprostol, TXA
Transfer into Obstetric Unit or ED - consider pre alert if concerned mum's condition.
Estimate blood loss
Perineal trauma - apply external pressure directly using a pad/sanitary towel
Maternal Antepartum haemorrhage
PREGNANT AND POST-PARTUM WOMEN MAY APPEAR WELL EVEN WITH SIGNIFICANT BLOOD LOSS
Haemorrhages my be revealed or concealed
<20 weeks bleeding - miscarriage, ruptured ectopic pregnancy
>20 weeks bleeding - late miscarriage, low-lying placenta, placental abruption, uterine rupture, ruptured vasa praevia
From birth to 4 weeks - Tone, Tear, Tissue, Thrombin (Any fresh bleeding after 20
weeks, regardless of amount- RED FLAG)
Ectopic pregnancy is when an egg implants somewhere other then the uterine wall most common between 6-8 weeks gestation.
Signs and symptoms
Vaginal bleeding
Vomiting and nausea
Lower abdominal pain
Sharp cramps/one sided pain
Pain in neck, rectum or shoulder
Feeling faint/collapse
Placental abruptions - when the placenta either is partially or full detaches from the uterine wall
Symptoms include vaginal bleeding (may be no blood seen externally), constant abdominal pain and hard rigid abdomen
Placenta praevia - the placenta embeds near to or over the opening of the womb
It can cause silent bleeding - vaginal bleeding that is not associated with pain
Cord prolapse
A cord prolapse is when the cord comes before the baby
knee chest position allows gravity to help, stay in this position as long as possible then run to hospital with mum lying on her side if possible put something under her hip
Assist mum to wear knickers and a pad to hold cord in place.
If too much cord presenting, sling in hammock using a towel to carry to hospital/get to truck
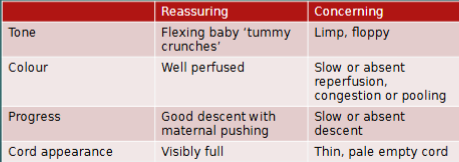
Final breech
Breech is essentially feet or buttocks presenting instead of a head
Start timer here
Encourage continuous pushing
Do NOT wait for contractions as they may have stopped.
Prepare firm, flat surface off the floor and warm the room
Call for help?
Baby needs to be fully out/born in 5 minutes if not run to hospital
you want bay bum to mum tum, if not thumps to bum fingers on femurs and rotate
if you see a foot/feet presentation run to hospital
ensure you get consent before internal monoverse
Shoulder Dystocia
shoulder dystocia is then the head is born and the shoulders get stuck behind the symphysis pubis
request HELP (CCP or more senior)
stop pushing
prep for resus
lay mum flat on her back, bring knees up to her abdomen, then push with the next contraction
if that doesn’t work suprapubic pressure
then try all 4s
NLS
Dry the baby and cover with warm dry towels and hat, if conveying warm the ambulance to the maximum prior to departure
as part of birth imminent prep for a resus
Open the airway, and assess colour, tone, breathing & heart rate
The lungs need to be cleared by some good inflation breaths. If the baby doesn’t do this by crying, give 5 using a bag-valve-mask. Reassess.
If no improvement, give 30 seconds of ventilation breaths – 1 second duration, rate 30/minute. Reassess.
If no improvement, 30 seconds 3:1 chest compressions, with oxygen. Reassess.
If no improvement, continue 3:1, consider hospital, consider drugs, consider SpO2 (right hand). Reassess every 30s