Human Physiology BIO1220 Exam
Lecture 1: Basic Biochemistry
- Chemical reactions
- Atoms
- An atom consists of protons and neutrons (nucleus) surrounded by electrons in “shells”
- Atoms share electrons in shells
- Molecule is most stable when shell is complete
- Complete shells: N^2
- Ex) Nitrogen
- First shell: 2 x 1^2=2 electrons
- Second shell: 2 x 2^2=8 electrons
- Third shell: 2 x 3^2=18 electrons
- Ex) Nitrogen
- Elements most abundantly found in the human body
- Carbon
- Oxygen
- Nitrogen
- Hydrogen
- Carbon
- Second most abundant element
- Backbone of compounds within the body
- Nucleus: protons and neutrons
- Carbon: 4 electrons in the outer shell
- Combining atoms
- Atoms can give rise to ions, molecules, and compounds
- Ions: atoms that have a negative or positive charge because it has an unequal number of electrons and protons
- Molecules: two or more atoms that share electrons
- Compounds: contain atoms of two or more elements (H2O vs O2)
- Typically consists of 2 or more elements chemically bonded in a fixed ratio
- Free radicals and their effect on health
- An atom or molecule with an unpaired electron in its outer shell
- Unstable, highly reactive, destructive to nearby molecules
- Generation of free radicals is increased when exposed to UV light, X-rays, certain chemicals, certain metabolic processes
- Effects partially offset by “antioxidants”
- An atom or molecule with an unpaired electron in its outer shell
- Chemical bonds
- Forces that hold together the atoms of a molecule or compound
- Likelihood depends on the number of electrons in an atom’s outermost shell
- Most stable elements have 8 electrons in outermost shell
- Carbon, Oxygen, Nitrogen, and Hydrogen do not have 8 electrons in their outer shells, they form molecules by sharing electrons
- Chemical reaction
- Occurs whenever a chemical bond is formed, rearranged, or broken
- Ex) the combining of 2 hydrogen atoms to form hydrogen gas
- Reactants -> product
- Other common reactions
- 2H +O = H2O (water)
- 4H + C = CH4 (methane)
- Carbon has 4 electrons in outer shell
- Addition of 4 more from hydrogen atoms makes it complete
- Once we have methane, we can add 2 oxygen molecules
- CH4 + 2O2 = CO2 + H2O
- Ie methane breaks down into carbon dioxide and water when oxygen is added
- Energy flow in chemical reactions
- Chemical reactions either use or release energy that was present in the chemical bonds
- Exergonic: a spontaneous chemical reaction where there is a net release of free energy
- Endergonic: a nonspontaneous chemical reaction where energy is absorbed from the surroundings
- What determines whether energy is released or absorbed?
- The change in potential energy in the chemical bonds
- All chemicals in the body are either:
- Organic
- Contain carbon
- Usually very large
- Inorganic
- All others
- Water, salts, acids, bases
- Organic
- Inorganic Compounds
- Water
- Boiling point: 100C
- Freezing point: 0C
- Density: 1g/cm^3
- Water is an excellent solvent
- This is largely due to the polarity of water molecules
- Negative side associates with positive end of solute molecule
- Positive side associates with negative end of solute molecule
- This is largely due to the polarity of water molecules
- Water has unique characteristics that make it essential to life:
- High heat capacity
- Resistant to temperature change
- High heat of vapourization
- Energy required to make water boil
- High surface tension
- Water molecules stick together
- This is why salt (NaCl) dissolves so easily in water!
- Negative side associates with Na+
- Positive side associates with Cl-
- High heat capacity
- Water can also act as a cushion
- Can be very important in protecting the body’s internal structures
- Ex) Cerebrospinal fluid protecting brain is largely made up of water
- Salts
- Contain positive ions (cations) other than H+
- CATions are PAWsitive
- Cats release energy by BREAKING things
- Contain negative ions (anions) other than OH-
- Typically dissociate readily in water
- Important salts of the body:
- NaCl (sodium chloride)
- CaCO3 (calcium carbonate)
- KCl (potassium chloride)
- CaPO4 (calcium phosphate)
- Contain positive ions (cations) other than H+
- Acids and bases
- Acids release H+ ions in large amounts
- “Proton donors”
- Ex) hydrochloric acid (HCl) is an important acid found in the stomach
- H+ is the proton, Cl- is the anion
- Bases take up hydrogen ions
- “Proton acceptors”
- Ex) bicarbonate ion (HCO3-) is an important base found in blood
- HCO3- + H+ = H2CO3 (carbonic acid)
- Ex) ammonia (NH3), a common waste product is also a base
- NH3 + H+ = NH4 (ammonium)
- Acids release H+ ions in large amounts
- pH scale
- A measure of how acidic or basic a solution is
- Acidic: 0-6
- Neutral: 7
- Basic (alkaline): 8-14
- Buffers
- Living cells and tissues are very sensitive to changes in pH
- Need to maintain a constant pH of 6.5 to 7.2
- Regulation of pH is carried out by “buffers”
- Molecules that resist abrupt changes in pH
- Organic Compounds
- Organic compounds include:
- Carbohydrates
- Lipids
- Proteins
- Nucleic acids
- What makes carbon so special?
- Inorganic compounds relatively simple (salts)
- Carbon forms bonds with many other carbon atoms
- Large number of shapes and sizes
- Unique structure and function
- Carbohydrates
- Sugars and starches
- Contain carbon, hydrogen, and oxygen
- Only make up 2-3% of total body mass
- Monosaccharides: simple sugars
- General formula: (CH2O)n, where n=number of carbon atoms
- Important for health: glucose (blood sugar)
- C6H12O6
- Glucose can be absorbed directly into blood
- Does not require digestion
- Important when looking at diabetes
- Disaccharides: double sugar
- Form when 2 simple sugars combine
- Ex) glucose + fructose = sucrose
- Ex) glucose + galactose = lactose
- Ex) glucose + glucose = maltose
- Polysaccharides: many simple sugars linked together
- Form in which most carbohydrates are found
- Homopolysaccharides: many molecules of one sugar
- Glycogen, starch, cellulose, many others
- Heteropolysaccharides: most of these contain only 2 types and are associated with proteins
- Glycoproteins
- Regulating blood sugar
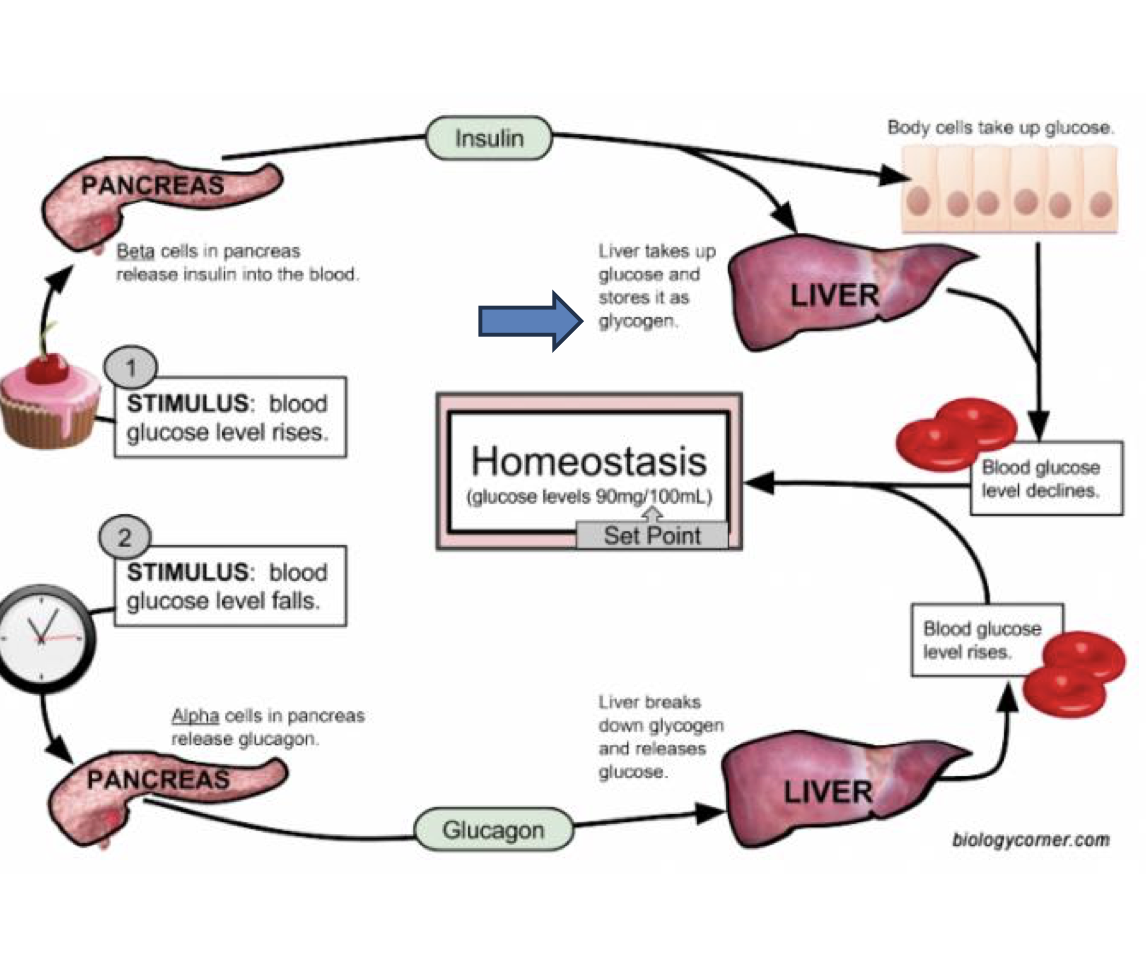
- The most important homopolysaccharides in humans is glycogen
- Used for storage of glucose
- Made and stored primarily in the liver, skeletal muscles, and cardiac muscles
- Storage varies dramatically with diet, exercise, stress
- Starch is the equivalent storage product found in plants
- The most common carbohydrate in human diets
- Large amounts in wheat, potatoes, rice, corn, etc
- Made by leaves during day, used as energy source at night
- Also used for non-food purposes
- Ex) making paper
- What do carbohydrates do?
- Main function is to provide energy
- Most important is glucose
- Used to make ATP (one glucose molecules makes 38 ATP when combined with 6O2)
- Lipids
- Also contain carbon, hydrogen, and oxygen
- Proportion of oxygen is lower
- Make up 18-25% of body mass
- Are made of fatty acid monomers
- Main types of lipids:
- Triglycerides
- Phospholipids
- Steroids and waxes
- Fatty acids
- Among the simplest lipids
- Can be broken down to produce ATP
- Triglycerides
- Neutral fats
- When solid: fat
- When liquid: oil
- Very large molecules used for storage
- Generally found just below the skin
- Phospholipids
- Modified triglycerides
- Contain phosphorus
- Most importantly found in cell membranes
- Steroids
- Structurally very different than triglycerides
- Most important: cholesterol
- Essential for human life
- What do lipids do?
- Energy storage
- Protection of body organs
- Structural components of membranes
- Chemical messengers (steroid hormones)
- Proteins
- The basic structural material of the body
- 12-18% of body mass
- All contain carbon, oxygen, hydrogen, and nitrogen
- Many also contain sulfur
- Proteins are composed of many amino acids
- 2 functional groups common to all amino acids:
- 1) amine group
- 2) organic acid group
- A 3rd functional groups makes each amino acid unique
- There are 20 common amino acids
- These link together to form peptides
- 2 amino acids: dipeptide
- 3 amino acids: tripeptide
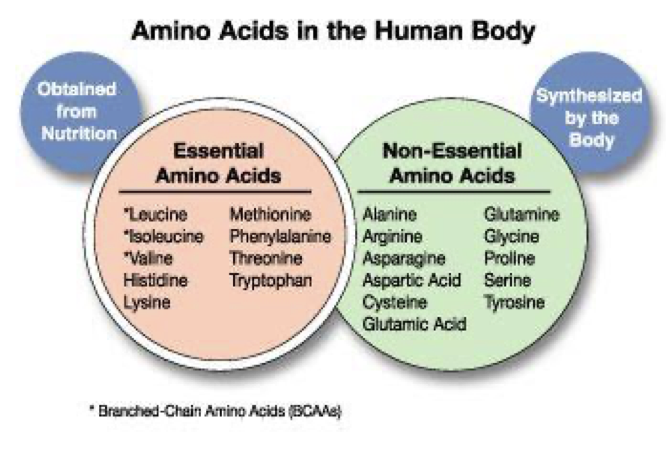
- Must memorize the amino acids! Think: PVT TIM HiLL
- Formation of a dipeptide from 2 amino acids:
- Peptide bonds
- But a protein is more than a long chain of amino acids!
- Proteins have many structural levels
- Primary
- Amino acids in polypeptide chain
- Secondary
- Polypeptide chains form spirals or sheets
- Tertiary
- Spirals or sheets fold up
- Quaternary
- 2 or more chains combine to form functional protein
- Primary
- Proteins have many structural levels
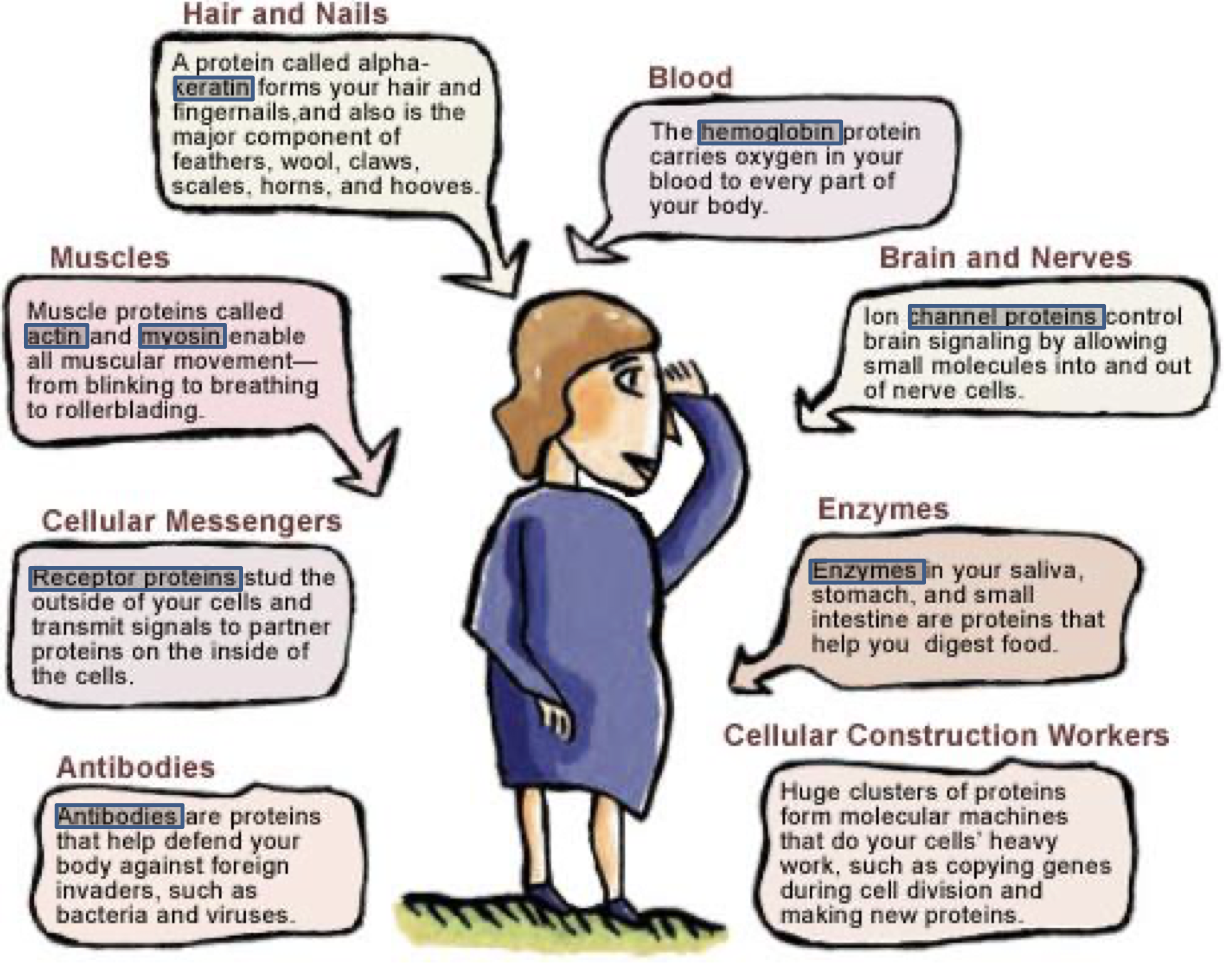
- There are many kinds of proteins with many different functions
- One important group that you must know:
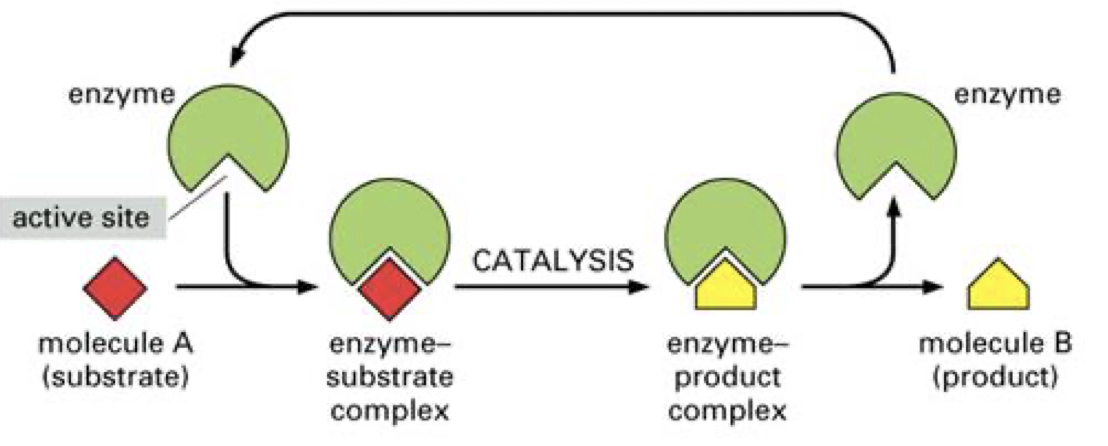
- Enzymes: proteins that act as catalysts
- Catalysts speed up biochemical reactions
- Not used during these reactions
- Reduce the energy needed to start the reaction
- Enzymes: proteins that act as catalysts
- One important group that you must know:
- How do enzymes work?
- Some other important proteins:
- Nucleic acids
- The largest molecules in the body
- Composed of:
- Carbon, oxygen, hydrogen, nitrogen, phosphorous
- 2 classes are:
- DNA (deoxyribonucleic acid)
- RNA (ribonucleic acid)
- The structural unit of nucleic acids are nucleotides
- There are 5 of these:
- Adenine (A)
- Guanine (G)
- These 2 are the purines (2 ring bases)
- Cytosine (C)
- Thymidine (T)
- Uracil (U)
- These 3 are pyrimidines (one ring bases)
- There are 5 of these:
- DNA and RNA are both composed of nucleotides
- DNA
- Found in the nucleus
- 2 main roles:
- Replicate itself so it is found in nearly all cells
- Provide information for building all proteins
- Double helix
- RNA
- Found outside the nucleus (usually)
- Works for DNA
- Carries out orders for protein synthesis
- Different types of RNA carry out different parts of the building process
- Single strands of nucleic acids
- T replaced with U
- DNA
- Base pairing
- G with C
- A with T
- A nucleotide is composed of a phosphate, sugar, and base
- Adenosine Triphosphate (ATP)
- Earlier we said that glucose is used to make ATP
- ATP provides the energy that is used by cells directly
- Earlier we said that glucose is used to make ATP
- Cellular respiration
- An important exergonic reaction that takes place in the human body all the time
- C6H12O6 + 6O2 -> 6CO2 + 6H2O + energy (ATP)
- Glucose + oxygen -> carbon dioxide + water + energy (ATP)
Lecture 2: Cell Anatomy and Physiology
- Overview of Cells
- Cells overview
- The cell is the basic unit of life
- The activity of the organism depends on the activities of the cells
- The activities of cells depend on their shape, form, and internal structures
- New cells arise from previously existing cells
- There are about 200 cell types in the body
- Classified based on structure and function
- Thus, not all cells have the same components
- However, most cells have 3 major divisions:
- Plasma membrane: outer boundary
- Cytoplasm: fluid and organelles
- Nucleus: controls activities
- The plasma membrane
- Plasma membrane
- Many differences in cell types due to subtle differences in membranes
- Allow cells to interact differently with same ECF (extracellular fluid)
- Many differences in cell types due to subtle differences in membranes
- Structure of plasma membrane
- Cell membranes contain 2 key components
- 1) Double layer of phospholipids
- Relatively impervious to water
- 2) Protein molecules
- Permit movement of specific chemicals
- Serve as signaling functions
- 1) Double layer of phospholipids
- Cell membranes contain 2 key components
- Phospholipid bilayer
- Hydrophilic (water-loving) head
- Hydrophobic (water-fearing) tail
- Arranged in a lipid bilayer
- Tails always pointing towards each other
- Also find: cholesterol
- Is not a rigid structure, but fluid in nature
- Phospholipids not held together by strong bonds
- Can twirl about
- Can move within their own half of the layer
- Cholesterol contributes to fluidity
- Tucked between phospholipid molecules
- Prevents crystallization
- Provides stability
- Phospholipids not held together by strong bonds
- Thus, the phospholipid bilayer serves 3 important functions:
- 1) Forms structure of membrane
- 2) Forms a barrier to passage of water soluble substances between ECF and ICF
- 3) Responsible for fluidity of membrane
- Some cells constantly change shape
- Membrane proteins
- Attached to or inserted within lipid bilayer
- Plasma membrane contains approximately 50 times as many lipid molecules
- However, protein’s molecules make up almost half the membrane’s mass
- 2 main groups of proteins:
- Integral proteins: embedded in the membrane
- Peripheral proteins: attached to one surface
- Types of membrane proteins:
- Glycoprotein: protein with an attached carbohydrate
- Peripheral protein: anchored to only one side of the membrane
- Integral protein: permanently embedded within a membrane
- Proteins in the cell membrane can serve a variety of purposes:
- Structural support
- Transport of molecules across the membrane
- Enzymatic control of chemical reactions at cell surface
- Receptors for certain molecules (ex= hormones)
- Markers (ex=antigens) that identify the cell (and individual)
- In addition to lipid and proteins, cell membrane also contains carbohydrates
- Primarily attached to outer surface of membrane
- Are negatively charged
- Affects activity of regulatory molecules and interactions between cells
- Ex) help keep red blood cells apart
- Affects activity of regulatory molecules and interactions between cells
- Cilia and flagella
- Cilia propel fluids across surfaces of cells that are firmly attached in place
- Ex) cells of the respiratory tract
- Flagella have similar structure but generally move entire cell
- Also, are much longer
- Ex) Sperm cell
- Also, are much longer
- Cilia propel fluids across surfaces of cells that are firmly attached in place
- Cell to cell adhesion
- Plasma membranes serve not only as outer boundaries of cells but also participate in cell to cell adhesions
- 3 kinds of cell junctions assist in binding cells together
- 1) Tight junctions
- 2) Desmosomes
- 3) Gap junctions
- Tight junctions
- Integral proteins in adjacent cells fuse together
- Very difficult for anything to pass between adjacent cells
- Found primarily in sheets of epithelial tissue
- Highly selective barriers
- Separate compartments having different chemical composition
- Passage across epithelial barrier must take place through cells
- Desmosomes
- Act like a zipper to hold cells together (adhering junctions)
- Important in cells where there is mechanical stress (ex= muscle, skin, uterus)
- Keratin filaments inside of cell may extend to desmosome on opposite side
- Provide increased tensile strength
- Gap junctions
- Used to communicate between adjacent cells
- Permit passage of small signaling molecules
- Provides one mechanism of cooperative cell activity
- Connexins made up of 6 proteins arranged in hollow tube-like structure
- 2 connexins join end to end
- Especially abundant in cardiac and smooth muscle
- Used to communicate between adjacent cells
- Membrane transport
- Tissues consist of cells embedded in an extracellular matrix (ECM)
- ECM components differ for each type of tissue
- Provide different local environments
- Anything that passes between the cell and the surrounding ECM must be able to penetrate the plasma membrane
- Plasma membrane is selectively permeable
- Allow certain substances to pass through
- Tissues consist of cells embedded in an extracellular matrix (ECM)
- 2 properties of the particles determine whether they can permeate the plasma membrane without assistance
- 1) Solubility in lipid
- Highly lipid-soluble particles can dissolve in lipid bilayer
- Includes uncharged or nonpolar molecules (ex= O2, CO2, fatty acids)
- 2) Size
- Water soluble particles must be small enough to fit through specific channels
- 1) Solubility in lipid
- Even if a particle can permeate membrane because of its lipid solubility or ability to fit through a channel, some force is needed
- 2 ways of doing this:
- 1) Unassisted membrane transport
- Down concentration gradients
- 2) assisted membrane transport
- Carrier-mediated and vesicular transport
- 1) Unassisted membrane transport
- 2 ways of doing this:
- Unassisted membrane transport
- Molecules that can penetrate the plasma membrane on their own can be driven by diffusion down a gradient
- Diffusion
- Movement of solutes down the concentration gradient (high to low concentration)
- Molecules have a tendency to become evenly spaced if allowed to
- How fast do molecules move?
- Temperature is directionally proportional to movement
- Substances diffuse faster at higher temperatures
- Size is inversely proportional to movement speed
- Larger molecules diffuse more slowly
- What happens if plasma membrane separates areas having different concentrations of substances?
- Does not matter if there is a barrier as long as it’s permeable to substance!
- The difference in concentration between adjacent areas is the concentration gradient
- An example of an important biological process that relies on diffusion
- Oxygen diffuses out of lungs, into bloodstream
- Then diffuses out of bloodstream, into tissues
- Passive diffusion of ions
- So far, have examined the flow of substances down a concentration gradient
- Substance can also diffuse along an electrical gradient
- Oppositely charged ions attract each other
- Both of these processes often work together
- If both electrical and concentration gradients act on an ion, the result is an:
- Electrochemical gradient!!
- If both electrical and concentration gradients act on an ion, the result is an:
- So far, have examined the flow of substances down a concentration gradient
- Osmosis
- Water can readily permeate the plasma membrane
- Small enough to slip between lipid bilayer (slowly!)
- Some cells have aquaporins to facilitate this movement
- About a billion molecules of H2O can pass through aquaporin every second
- However, the driving force is the same:
- The concentration gradient of H2O
- Water can readily permeate the plasma membrane
- A bit confusing…
- The concentration of a solution refers to the density of solute in a given volume of water
- In general, one molecule of solute will displace one molecule of water
- As the [solute] increases, the [water] decreases
- So water flows to areas of higher solute concentration
- This is osmosis!
- The concentration of a solution refers to the density of solute in a given volume of water
- But what happens to the solute concentration?
- It depends on whether it can get through the membrane
- If it can: both water and solute move through membrane until both are evenly distributed
- If it cannot: solute cannot pass through membrane but water can
- As a result of water movement, volume of one side increases
- Eventually, solute concentrations on both sides become equal
- Osmosis is the major force responsible for the net movement of water into and out of cells
- Depends on concentration of solutes in extracellular fluid (tonicity)
- Isotonic solution
- Same solute/water concentration on inside and outside of cell
- Water moves both into and out of cell
- No change in cell shape
- Hypertonic solution
- Higher concentration of solutes outside the cell
- Water flows out of cell
- Cells shrink
- Hypotonic solution
- Lower concentration of solutes outside cell
- Water flows into cell
- Cells expand and burst (lyse)
- Assisted membrane transport
- There are 3 cases in which molecules must be helped across the plasma membrane:
- Poorly lipid soluble molecules
- Small ions going against concentration gradient
- substances/molecules that are very large
- To transport these molecules, must use:
- carrier-mediated transport
- Vesicular transport
- There are 3 cases in which molecules must be helped across the plasma membrane:
- Carrier-mediated transport
- Carrier proteins span the plasma membrane
- Can have binding sites at either side (ECF or ICF)
- These proteins display 3 important properties:
- 1. Specificity: carry one substance (or a few)
- 2. Saturation: limited number of binding sites
- 3. Competition: several closely related compounds may compete for a ride
- Can take 2 forms:
- Facilitated diffusion
- Active transport
- Facilitated diffusion:
- Uses a carrier to assist the transport of a substance downhill from high to low concentration
- Ex) glucose into cells
- Important source of fuel
- Higher concentration in blood than tissues
- However, cannot cross cell membrane on its own
- Active transport
- Similar but goes against concentration gradient
- Requires energy in the form of ATP
- Ex) Uptake of iodine by thyroid
- 99% of iodine is concentrated in thyroid gland
- To move iodine from blood (where concentration is low) to thyroid requires energy
- The best example of active transport is the sodium-potassium pump
- Carrier protein transports sodium ions out of the cell, concentrating it in ECF
- Potassium picked up on outside of cell and transported to ICF
- A single nerve cell contains about a million Na+-K+ pumps that transport about 200 million ions per second
- Sodium-potassium pump: keeps cell at a state where neurons are ready to fire
- 1) 3 cytoplasmic Na+ bind to the pump
- 2) ATP donates a phosphate group for energy
- 3) The protein changes its shape, expelling Na+ to the outside
- 4) 2 extracellular K+ bind to the pump, releasing the phosphate
- 5) The pump resumes its original shape
- 6) K+ is released inside
- Passive transport vs active transport
- Passive: diffusion and facilitated diffusion
- Active: use of ATP
- Vesicular transport
- We have looked at substances that can diffuse through the plasma membrane or through channels in the membrane
- What about substances that cannot cross the membrane?
- Ex) large polar molecules, ingestion of invading bacteria
- Too big for channels, no carriers exist
- These are wrapped in a membrane-enclosed vesicle
- Energy required
- What about substances that cannot cross the membrane?
- We have looked at substances that can diffuse through the plasma membrane or through channels in the membrane
- Certain substances need to move into or out of cell
- Endocytosis: moving substance into the cell
- Exocytosis: moving substances out of the cell
- Endocytosis
- Phagocytosis
- Large molecules internalized
- Only done by a few cell types
- Phagocytes
- Most notable are certain types of white blood cells
- Good for getting rid of diffuse debris or bacteria
- Once in safety of vesicle, can be broken down
- Pinocytosis
- A small droplet of extracellular fluid internalized
- Plasma membrane infolds, captures fluid, and membrane seals at surface
- Can be carried out by most body cells
- Also a good way of getting rid of extra plasma membrane!
- Receptor-mediated endocytosis
- Highly selective
- Unlike pinocytosis which is nonselective
- Enables cells to import specific large molecules needed by the cell
- Ex) cholesterol complexes, vitamin B12, insulin, iron
- Can be exploited by certain viruses!
- Highly selective
- Phagocytosis
- Exocytosis
- Almost the reverse of endocytosis
- Can be used for secreting large molecules
- Highly specific
- Ex) hormones, neurotransmitters
- Also used to add components to plasma membrane
- Carriers, channels, receptors
- The cytoplasm and nucleus
- Cytoplasm
- Consists of 2 components
- Cytosol
- Semitransparent fluid
- Mostly water with proteins, salts, sugars, etc
- Organelles
- Each carries out specific functions
- Cytosol
- Consists of 2 components
- Some important organelles
- Mitochondria: energy production
- Smooth endoplasmic reticulum: lipid production, detoxification
- Rough endoplasmic reticulum: protein production
- Golgi apparatus: protein modification and export
- Lysosome: protein destruction
- Nucleus
- Control centre of the cell
- Provides instructions, particularly for building proteins
- Most cells have one nucleus
- A few have more than one (skeletal muscle)
- One type (red blood cells) has none
- The membrane around the nucleus, like the plasma membrane, is selectively permeable
- Punctuated with nuclear pores
- Allows some control over what goes in and out
Lecture 3: Communication and Integration
- Cell to cell communication
- Need to convey a huge amount of information very quickly
- 2 basic types of physiological signals
- Electrical: change in cell’s membrane potential
- Chemical: molecules secreted into extracellular fluid
- 2 basic types of physiological signals
- Local communication
- There are 3 ways that cells can communicate over short distances
- Gap junctions
- Cell-to-cell contact
- Paracrine and autocrine signals’
- There are 3 ways that cells can communicate over short distances
- Gap junctions
- Simplest way of transferring information is through cytoplasmic bridges created by gap junctions
- Connexions provide channels
- Good for ions and small molecules
- No good for large molecules
- Found in nearly all cell types
- Cell-to-cell contact
- Some communication requires that surface molecules on one cell bind to those on another
- Contact-dependent signaling
- Important during growth and development
- Ex) nerve cells send out long extensions to reach distal ends of limbs
- Multiple cells involved
- Paracrine and autocrine signals
- Paracrine signal: acts in immediate vicinity of cell that secreted signal
- Autocrine signal: acts on cell that secreted it
- In some cases, a molecule may act as both
- Diffuse through interstitial fluid
- Several important classes of molecules act as local signals
- Histamine: an example of paracrine signal
- Stored in certain cells of immune system
- Released in response to allergic reactions, injury, or infection
- Causes blood vessels to dilate and capillaries to become more permeable
- Releases white blood cells and antibodies
- Mast cells detect injury to nearby cells and release histamine, initiating inflammatory response. Histamine increases blood flow to the wound sites, bringing other immune cells that neutralize pathogens. The blood influx causes the wound to swell, redden, and become warm and painful
- Histamine effects
- Blot clots
- Gastric acid secretion
- Blood vessels to dilate
- Bronchoconstriction
- Increases the permeability of capillaries
- Adrenaline is released
- Swelling and inflammation
- Frequent heartbeat
- Long distance communication
- May be electrical or chemical
- Endocrine cell uses hormones
- Chemical signals secreted into blood and are distributed throughout body
- Nervous system uses a combination of electrical and chemical signals
- Neurotransmitters diffuse across narrow extracellular space and have rapid effect
- Neurohormones released into blood and affects cells farther away
- Occurs in synaptic cleft
- Signal pathways
- Why do some cells respond to a chemical signal and other cells ignore it?
- Target cell receptor proteins
- If a cell has a receptor for the signal molecule, response initiated
- Signaling path features:
- Signal molecule is a ligand
- Binds to receptor molecule
- Ligand-receptor complex activated
- Activated receptor activated intracellular molecule(s)
- Response initiated
- Signal molecule is a ligand
- How do antihistamines work?
- The antihistamine molecules compete for binding sites with the histamine molecules
- The result is a reduced response
- Good when histamine response is more severe than necessary
- Pathways can be very complex!
- Generally a lot of steps before a response is initiated
- Most physiological processes use some variation of these pathways
- Many drugs/illnesses work by influencing these pathways
- Modulation of Signal Pathways
- Different cells may respond differently to one kind of signal molecule
- Response depends on the receptor and its associated pathways
- One ligand, multiple receptos
- Ex) Epinephrine
- Dilates blood vessels in skeletal muscle
- Constricts blood vessels in intestine
- How does one chemical have opposite effects?
- The response depends on the receptor, not the ligand, alpha vs beta receptor
- Alpha receptor in intestinal blood vessel
- Binding of ligand initiates chain of events that terminates in cell constriction
- Beta-receptor in skeletal muscle blood vessel
- Binding results in cell dilation
- The response depends on the receptor, not the ligand, alpha vs beta receptor
- Ex) Epinephrine
- Specificity and competition
- Different ligand molecules with similar structures may be able to bind with the same receptor
- Ex) Norepinephrine and epinephrine (adrenaline):
- Both bind to class of receptors called adrenergic receptors
- Demonstrates specificity of receptors since they can’t bind with anything else
- Both can bind to alpha and beta receptors
- But they have slightly different affinities
- Both bind to class of receptors called adrenergic receptors
- Agonists and antagonists
- 2 things can happen when a ligand binds with a receptor:
- 1) Ligand activates receptor
- Elicits a response
- Agonist
- 2) Ligand occupies binding site
- Prevents a response
- Antagonist
- 1) Ligand activates receptor
- 2 things can happen when a ligand binds with a receptor:
- Pharmacologists often use this principle to design drugs
- Depending on the similarity of the drug molecule to the ligand molecule, get different effects
- Can modify effects of certain cells
- Naloxone
- Brand name= Narcan
- Used to treat life threatening opioid overdose or suspected opioid overdose
- Naloxone works by blocking the opioid receptor, it acts as an opioid antagonist
- Sometimes we are exposed to similar substances without wanting to be!
- Ex) hormone disruptors
- Can mimic particular hormone (ex= estrogen)
- Results in increased cellular response
- Can block particular hormone
- Results in decreased cellular response
- Can mimic particular hormone (ex= estrogen)
- Ex) hormone disruptors
- BPA is an example of a hormone disruptor
- It can bind to estrogen receptors or androgen receptor
- BPA= Bisphenol A
- Has effects on metabolism, tumor growth, and male fertility
- Homeostatic reflex pathways
- Homeostatic reflex pathway
- Cellular signaling systems responsible for maintaining homeostasis
- Long distance reflex pathways involve 2 control systems
- Nervous system
- Endocrine system
- Involve 7 steps:
- Stimulus, sensor, input signal, integrating centre, output signal, target, response
- Stimulus
- Disturbance or change that sets pathway in motion
- Ex) change in temperature, blood pressure, oxygen concentration, etc
- Sensor
- A multicellular receptor that responds to changes in the environment
- Ex) eyes, ears, mouth, nose
- Skin is covered in less complex receptors to detect changes in temperature, touch, vibration, pain
- Many internal sensors for body position, blood pressure, oxygen levels
- Input signal
- Varies depending on type of reflex
- Not found in endocrine reflex since stimulus acts directly on endocrine cell
- Serves as both sensor and integrating centre
- Integration centre
- In neural reflexes, integrating centre lies within central nervous system
- Interpret and initiate a response
- Output signal
- Nervous system: electrical and chemical signals transmitted by a neuron
- Endocrine system: hormones that travel in blood
- Target
- Cells or tissues that carry out the response
- Neural pathway: muscles, glands, adipose tissue
- Endocrine pathway: cells having proper receptor
- Response
- Cellular response that takes place in target cell
- Systemic response is the overall change in the organism
- Examples of neuronal and endocrine homeostatic control mechanisms
- 1) Neural reflex
- Dim light
- Signal received from sympathetic nervous system
- Pupils dilate
- Bright light
- Signal received from parasympathetic nervous system
- Pupils constrict
- Dim light
- 2) Endocrine reflex
- The endocrine cell acts as the sensor and integrating centre
- Low blood concentration of calcium leads to release of parathyroid hormone
- Stimulates release of calcium into blood
- 1) Neural reflex
Lecture 4: The Nervous System - impulses and neurotransmitters
- Overview of the nervous system
- Nervous system overview
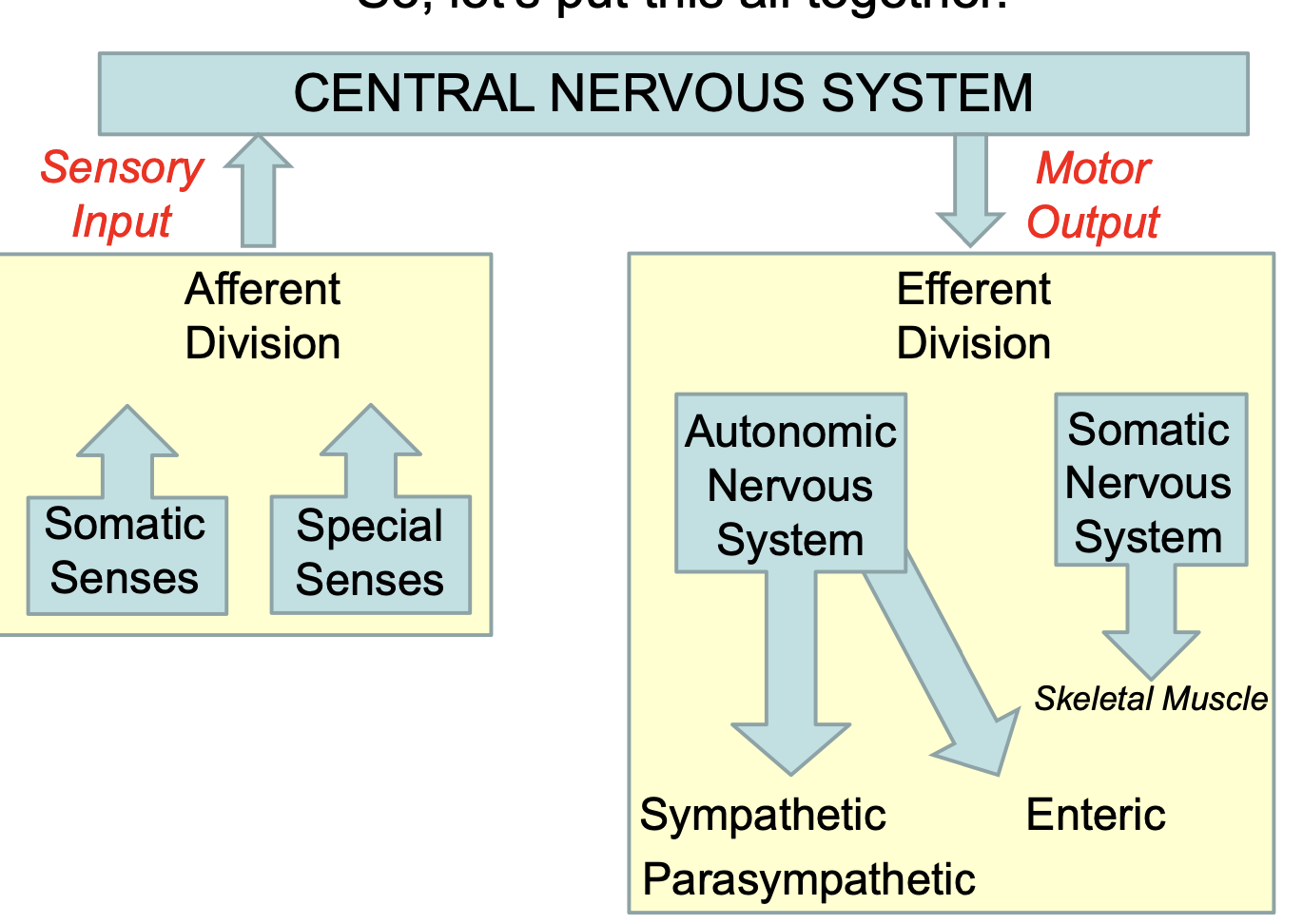
- Structurally, the NS is divided into:
- 1) Central nervous system
- Brain
- Spinal cord
- 2) Peripheral nervous system
- Neural tissue outside of CNS
- Sensory and motor neurons
- 1) Central nervous system
- Functionally, the nervous system is divided into:
- 1) Sensory nervous system
- Contains receptors
- Transmits information from receptors to CNS
- 2) Motor nervous system
- Transmits information from CNS to rest of body
- Sends motor information to effectors
- 1) Sensory nervous system
- You will also hear:
- Somatic (nerves)
- Usually to skeletal muscle
- Voluntary
- Autonomic (nerves)
- Usually to smooth muscle of body organs or glands
- Involuntary
- Somatic (nerves)
- Structurally, the NS is divided into:
- Fortunately, the CNS is well organized when it comes to sensory and motor nerves
- Sensory= afferent (to)
- Motor= efferent (away/exit)
- Have somatic and autonomic
- Central nervous system
- Neurons and glial cells
- The neuron
- Reception, transmission, and processing of stimuli
- Nerve cells are extremely variable in shape and size
- 3 main categories:
- Multipolar
- Have more than 2 processes
- One axon, many dendrites
- Most neurons
- Bipolar
- One axon, one dendrite
- Cochlear and vestibular ganglion, retina, olfactory mucosa
- Pseudounipolar
- Single process, close to cell body
- Divides into 2 branches
- Nerve impulse bypasses cell body
- Spinal and cranial ganglia
- Multipolar
- 3 main categories:
- Damaged neurons: limited capacity for repair
- Nervous system exhibits a great deal of plasticity
- New dendrites, new proteins, new contacts
- However, very little powers of regeneration
- If cells of PNS damaged, can be repaired if cell body is intact and Schwann cell is still functional
- If cells of CNS damaged, little chance of repair
- Olfactory epithelium long known to regenerate
- More recent evidence suggests other parts of brain may be able to undergo neurogenesis
- Nervous system exhibits a great deal of plasticity
- Glial cells
- Several types of cells that support and protect neurons
- About 10 times more abundant in mammalian brain than neurons
- Surround cell bodies, axons, and dendrites
- Occupy interneuronal spaces
- 1) Oligodendrocytes
- Produce myelin sheath that provides electrical insulation of neurons of central nervous system
- Have long processes that wrap around axons
- Produce myelin sheath that provides electrical insulation of neurons of central nervous system
- 2) Schwann cells
- Have the same function as oligodendrocytes but are located in the peripheral nervous system
- One Schwann cell forms myelin around a segment of one axon
- Spaces between adjacent cells are nodes of Ranvier
- Nerve fibers consist of axons enveloped by a special sheath
- Exhibit differences related to weather they belong to central or peripheral nervous system
- PNS= Schwann cells
- CNS= oligodendrocytes
- Axons of small diameter usually unmyelinated
- Thicker axons have increasingly numerous concentric sheath around them
- Myelinated fibers
- Exhibit differences related to weather they belong to central or peripheral nervous system
- Difference between unmyelinated and myelinated cells of the PNS
- Myelinated: faster conduction of the action potential as it jumps between nodes
- Multiple Sclerosis
- Results from the destruction of myelin
- Can be in brain or spinal cord
- Range of symptoms depending on what nerves are affected
- Cause unknown
- Treatments designed to prevents attacks and improve function
- Results from the destruction of myelin
- 3) Astrocytes
- Star-shaped cells with radiating processes
- Bind to capillaries (and elsewhere)
- Protoplasmic astrocytes
- Shorter, more numerous processes
- Found in gray matter
- Fibrous astrocytes
- Long processes
- Found in white matter
- Are the most numerous glial cells
- Provide structural support for neurons
- Help regulate ionic and chemical environment of neurons
- Important in blood-brain barrier
- Involved in repair processes
- 4) Ependymal cells
- Columnar epithelial cells that line the ventricles of brain and canal of spinal cord
- Involved in the production of cerebrospinal fluid in ventricles of brain
- Cilia on apical end used for moving cerebrospinal fluid around elsewhere
- May also serve as a reservoir for new neurons
- Also serve as first line of defense against viral infection
- 5) Microglial cells
- Found throughout brain and spinal cord
- Make up 10-15% of all cells in CNS
- Small, elongated cells with short processes
- Phagocytic cells derived from precursors from bone marrow
- Involved in inflammation and repair of the CNS
- Membrane and Action Potentials
- Membrane potential
- All eukaryotic cells have a difference in electrical charge between the inside and outside of the cell
- This is potential energy that can be used
- Outside of cell is positive
- Cytoplasm is negative
- Can measure the difference in charge
- All eukaryotic cells have a difference in electrical charge between the inside and outside of the cell
- Why the difference?
- Due largely to the sodium-potassium pump that moves Na+ and K+ against their concentration gradients
- 1) a Na/K pump pushes 3 sodium ions out of the cell for every 2 potassium ions going in
- 2) some K+ leaks out passively down concentration difference
- Due largely to the sodium-potassium pump that moves Na+ and K+ against their concentration gradients
- But there are positive ions inside and outside the cell!
- However, there are more positive ions outside the cell
- This means that the ICF is MORE NEGATIVE than the ECF
- Membrane resting potential refers to the voltage across a cell membrane when that cell is “at rest”/not engaged in any activity other than the normal maintenance of the cell
- Membrane potential
- The difference in electrical potential between the inside and outside of a cell
- Inside the cell is usually more negative (-40mV to -80mV)
- Due (partially) to the accumulation of more Na+ ions outside
- Result of sodium-potassium pump
- Action potentials
- What happens when a small area of the axon membrane is stimulated?
- Certain stimuli (mechanical or chemical) will activate sodium gates in the membrane
- Facilitated diffusion of Na+ into the cell
- Reduces resting potential (the ICF becomes more positive)
- If resting potential is reduced from -70mV to -50mV or -55mV, then an action potential is generated!
- 1) Na+ flow into cell through Na+ channels
- Depolarization
- 2) Polarity is reversed
- Interior of cell becomes more positive than outside in that region of the cell (or axon)
- 3) Membrane potential reaches +30mV
- Na+ channels close, K+ channels open
- K+ rushes out of the cell (down concentration gradient)
- Repolarization
- 4) Action potential completed
- Na+/K+ pumps extrude any extra sodium and recover potassium
- Membrane potential re-established
- Three things to note about action potentials
- 1) occurs very quickly as it occurs over a very small part of the membrane
- 2) Active transport processes not involved in the production of an action potential
- Simply the result of sodium and potassium flowing down concentration/electrical gradients
- Na+/K+ pumps still needed to maintain membrane potential
- 3) It’s an all-or-none process
- Gates are open for a fixed period of time
- Amplitudes of action potentials always the same
- Conduction of nerve impulses
- Nerve impulse conduction
- Depolarization of membrane opens up sodium channels in adjacent parts of membrane
- Wave of depolarization along the cell (axon)
- Nerve impulse
- Conduction in an unmyelinated axon
- Every patch of membrane that has Na+ and K+ gates can produce ATP
- Action potentials must be produced at every micrometer along axon
- Conduction relatively slow
- Conduction in a myelinated axon
- Myelinated sheath prevents Na+ and K+ from crossing membrane
- Gaps in sheath called nodes of Ranvier
- Have to be short distance apart
- Action potentials leap from node to node
- Signals travel much faster
- Synapses and Neurotransmitters
- Synapse
- Is responsible for the unidirectional transmission of nerve impulses
- In the CNS this is another neuron
- In the PNS this is another neuron, a muscle cell, or a glandular cell
- Can make contact with cell bodies, dendrites, or other axons (less frequently)
- Is responsible for the unidirectional transmission of nerve impulses
- Early in the 20th century, transmission thought to be electrical
- Nerve appeared to touch second cell
- Transmission very fast
- With improved techniques, gap between cells was observed
- Now know to be (mostly) chemical
- What happens at the synapse?
- Chemicals released at presynaptic endings
- Synaptic cleft between cells so arrow can only be observed with electron microscope
- Neurotransmitter molecules enclosed within synaptic vesicles
- These fuse with the membrane and are released
- Number that fuse depends on number of action potentials
- In more detail…
- Action potential arrives at synapse
- Calcium (Ca2+) gates open, Ca2+ enters cell
- Calcium ions cause neurotransmitter vesicles to fuse with membrane
- Release contents by exocytosis
- Neurotransmitter moves across short space (synaptic cleft) to post synaptic cell
- Neurotransmitter binds to membrane of next cell
- Causes sodium channels to open
- Sodium flows in
- If threshold reached, AP initiated
- Neurotransmitters usually broken down in synaptic cleft quickly
- Actions don’t last long
- 2 types of synapses
- Neurotransmitters may either move postsynaptic membrane potential closer or farther away from an action potential
- Excitatory synapses
- This is what we’ve been looking at so far
- Normally due to the flow of positive ions into postsynaptic cell (usually sodium)
- Inhibitory synapses
- Usually due to the opening of potassium or chloride channels
- K+ ions leak out of the cell or Cl- leaks into the cell
- Drop in negative membrane potential
- Decreases the likelihood of an action potential
- Sum of excitatory and inhibitory inputs determines if AP generated
- Neurotransmitters
- They are the brain chemicals that relay signals between nerve cells
- More than 50 different kinds
- Can be excitatory or inhibitory, or both
- Depends on the receptor
- Tell your heart to beat, your lungs to breathe, and your stomach to digest
- Can also affect mood, sleep, concentration, weight
- Some important neurotransmitters
- Acetylcholine
- Released at all neuromuscular junctions
- Triggers muscle contraction
- Also stimulates release of certain hormones
- Excitatory at neuromuscular junctions in skeletal muscle
- Inhibitory in cardiac muscle (autonomic nervous system)
- Dopamine
- Both an inhibitory and excitatory neurotransmitter
- Vital roles in movement, cognition, pleasure, motivation
- Plays a central role in positive reinforcement and motivation
- GABA
- Inhibitory neurotransmitter that is widely distributed in the brain
- Contributes to motor control, vision, and many other cortical functions
- Major inhibitory/calming neurotransmitter
- Serotonin
- Contributes to regulating body temperature, sleep, mood, appetite, and pain
- Affects most cells of brain
- Low levels are often associated with anxiety, panic attacks, obesity, insomnia, and fibromyalgia
- Norepinephrine
- Important for attentiveness, emotions, sleeping, dreaming, and learning
- Also released as a hormone where it causes blood vessels to contact and heart rate to increase
- Acetylcholine
Lecture 5: The Central Nervous System
- Overview of the CNS
- Central nervous system overview
- Consists of brain and spinal cord
- About ⅔ of the brain is made up of the cerebral hemispheres
- Higher functions like thought and memory
- Medulla oblongata is the hindmost part
- More routine functions like respiration and cardiovascular function
- The spinal cord extends from medulla oblongata to second lumbar vertebrae
- 2 enlargements:
- 1) Cervical: at base of neck, control of upper limb
- 2) Lumbosacral: control of lower limb
- Spinal cord ends at lower back
- Nerve fibers below that are called the cauda equina
- 2 enlargements:
- Internally, we can distinguish between white and grey matter in both the spinal cord and the brain
- Gray matter: dendrites and cell bodies of neurons, unmyelinated axons, and glial cells
- White matter: myelinated axons
- Grey matter forms the cortex which covers most of the surface of the brain
- White matter lies deep to the grey matter (white matter inside)
- In the spinal cord, grey matter is interior to white
- Position switches around the region of the medulla
- Protective structures
- The brain and spinal cord are protected by 3 different sets of tissue
- 1) Axial skeleton
- Both the brain and spinal cord are protected by bone
- The cranium and vertebral column
- 2) Ventricles and Cerebrospinal fluid
- Brain has hollow, fluid-filled cavities called ventricles
- Inside ventricles is choroid plexus
- Makes cerebrospinal fluid (CSF)
- CSF circulates around brain and spinal cord
- Helps cushion them from injury
- 3) Meninges
- 3 layers of connective tissue that surround spinal cord and brain
- Pia mater: innermost layer, adheres to surface, many blood vessels
- Arachnoid mater: weblike, avascular
- Dura mater: dense, irregular connective tissue
- 1) Axial skeleton
- Between the:
- Vertebral column and dura mater: epidural space
- Blood vessels, fat, and connective tissue
- Arachnoid mater and dura mater: subdural space
- Interstitial fluid
- Pia and arachnoid mater: subarachnoid space
- Cerebrospinal fluid
- Vertebral column and dura mater: epidural space
- The brain and spinal cord are protected by 3 different sets of tissue
- Epidural vs subdural hematoma
- Epidural hematoma: rapidly expanding with arterial blood
- Subdural hematoma: slowly expanding with venous blood
- The Brain
- 1) Forebrain
- a) Cerebrum
- Location of conscious thought processes and the origin of intellectual functions
- Accounts for about 80% of brain’s mass
- Ridges of cerebral tissue are called:
- Gyri (cingulate= gyrus)
- Sulci (cingulate= sulcus) are larger grooves between 5 lobes
- a) Cerebrum
- Cerebral hemispheres
- The cerebrum is composed of 2 halves called left and right cerebral hemispheres
- Corpus callosum
- The largest tract and the main tract that connects the 2 hemispheres
- There are an estimated 300 million neuronal axons traveling between the hemispheres
- Cerebral cortex
- Each hemisphere is composed of a thin outer shell
- Cerebral cortex
- Grey matter: “hardware” or cell bodies
- Covers a thick central core
- White matter: “wires” or axons
- The cerebrum is divided into 5 lobes, 4 of which are visible from the surface
- Parietal, occipital, frontal, temporal
- The insular lobe is covered by portions of the frontal, parietal, and temporal lobes
- Although the lobes can be distinguished anatomically, they do not always correspond to specific functional areas
- Some regions exhibit several different functions
- Some functions, such as memory or consciousness cannot be assigned to a particular region
- Each hemisphere is composed of a thin outer shell
- Parietal lobes
- Touch, pressure, heat, cold, pain (somesthetic sensations)
- Transmitted to somatosensory cortex located in parietal lobes
- Also, awareness of body position (proprioceptors)
- Frontal lobes
- Adjacent to somatosensory cortex is primary motor cortex
- Long axons of neurons go down spinal tract and synapse with peripheral nerves going to skeletal muscle
- Can make maps of sensory and motor homunculi
- Temporal lobes
- Auditory centers
- Receive sensory fibers from cochlea of each ear
- Involved in interpretation of visual and acoustic information
- Occipital lobes
- Main area responsible for vision
- Coordination of eye movements
- Insula lobes
- Interpretation of olfactory information
- Integration of sensations of pain with visceral responses
- Language
- Information about language regions comes mostly through study of aphasias
- Unlike sensory and motor information, areas responsible for language ability are found only in the left hemisphere
- Two important regions are:
- Broca’s area
- Speaking ability
- Located in left frontal lobe
- Wernicke’s area
- Language comprehension
- Located at junction of parietal, temporal, and frontal lobes
- Broca’s area
- Information about language regions comes mostly through study of aphasias
- Emotion and motivation
- Most important for emotional states is the hypothalamus (which we’ll deal with shortly) and the limbic system
- Limbic system forms a ring around the brainstem
- Aggression
- Fear
- Sex
- Goal-directed behaviour
- Most important for emotional states is the hypothalamus (which we’ll deal with shortly) and the limbic system
- Memory
- Involves several different brain regions
- Hippocampus, prefrontal lobe, mid-temporal lobe, cerebellum
- Different types of memory
- Short term, long term
- Cerebral cortex thought to store factual information
- Verbal memories in left hemisphere
- Visuospatial memories in right hemisphere
- Much of our information about memory comes from brain damage studies
- Involves several different brain regions
- Electroencephalograms
- Electric potential produced at synapses
- Can be measured by electrodes on scalp
- Deviations from normal used to detect abnormal states
- Electric potential produced at synapses
- Delta waves
- <4Hz
- Needed for rest and repair
- Common during deeper sleep
- Presence while awake in adult indicative of brain damage
- Theta waves
- 4-7Hz
- Temporal and occipital lobes
- Common in newborn infants
- Associated with drowsiness or light sleep in adults
- Alpha waves
- 8-13 Hz
- Best recorded from parietal and occipital lobes with eyes closed
- Awake and relaxed
- Beta waves
- 14-30Hz
- Strongest in frontal lobes
- Produced by visual and mental activity
- One more thing about EEGs…
- Can be used to distinguish various stages of sleep
- Resting sleep
- High amplitude, low frequency waves
- Rapid eye movement
- When dreams occur
- Lower frequency, high oscillation
- Resting sleep
- Can be used to distinguish various stages of sleep
- Sleep cycles
- Typically progress through each stage in one cycle
- About 90 minutes
- 4 or 5 cycles per night
- b) thalamus, hypothalamus, and epithalamus
- Thalamus consists of paired masses of grey matter
- Acts primarily as a relay center
- All sensory information (except smell) passes through on way to cerebrum
- The epithalamus lies above/behind thalamus
- Contains choroid plexus
- Makes cerebrospinal fluid
- Contains pineal gland
- Secretes hormone melatonin
- Major regulator of circadian rhythms
- Contains choroid plexus
- Hypothalamus is a link between the autonomic nervous and endocrine systems
- Controls or affects:
- Body temperature
- Thirst and urine output
- Food intake (hunger)
- Sleep cycles
- Anterior pituitary hormone secretion
- Production of posterior pituitary hormones
- Uterine contractions and milk ejection
- Smooth and cardiac muscle; exocrine glands
- Social and behavioral patterns
- Hypothalamus is the brain area most involved in regulating internal environment
- Ex) if body is cold, hypothalamus acts to:
- Increase heat production (shivering)
- Decrease heat loss (Constricting surface blood vessels)
- Typical homeostatic mechanism
- Negative feedback loop
- Ex) if body is cold, hypothalamus acts to:
- Controls or affects:
- Thalamus consists of paired masses of grey matter
- 2) Midbrain
- Located between hypothalamus and pons
- Has 4 round elevations on dorsal surface
- Corpora quadrigemina
- Two upper: visual reflexes
- Two lower: auditory reflexes
- Mediate reflex acts to visual and auditory stimuli
- Ex) flash of light or gunshot
- Mediate reflex acts to visual and auditory stimuli
- 3) Hindbrain
- Consists of 2 regions
- Pons and cerebellum
- Medulla oblongata
- Consists of 2 regions
- Pons
- Contains sensory and motor tracts that connect to the midbrain and medulla
- Several nuclei associated with cranial nerves
- Cooperates with medulla oblongata to regulate breathing
- Cerebellum
- Second largest structure of brain
- Outer grey matter, inner white matter
- More neurons than in the rest of the brain
- Important for:
- Maintaining balance and coordinating eye movements
- Fine motor movement
- Planning and initiating voluntary activity
- Medulla oblongata
- Last portion of brain before spinal cord
- About 3 cm long
- All ascending and descending tracts pass through
- Here they cross to other side
- Left side of brain receives/sends information from/to right side of body and vice versa
- Important in the regulation of breathing and cardiovascular responses
- What is the brain stem?
- Some sources argue the brain consists of 4 major parts: cerebrum, diencephalon, cerebellum, brainstem
- The brain stem is continuous with the spinal cord and consists of:
- Medulla oblongata
- Pons
- Midbrain
- The spinal cord
- Neurons, nerves, nerve tracts
- Looked at the structure of a neuron earlier
- A nerve is a group of axons
- Information can be going in both directions
- Sensory to CNS, motor to PNS
- Nerve tract is a group of nerve fibers
- Service the same of similar structures
- Nerve tracts
- Sensory information from most of the inside and outside of the body passes up ascending tracts of the spinal cord to the brain
- Motor activities, directed in the brain, pass down descending tracts of the spinal cord
- Remember:
- Grey matter on inside and white matter on outside
- All the tracts are located in the white matter
- The white matter of the vertebral column is separated into 3 columns:
- Dorsal white column
- Lateral white column
- Ventral white column
- The name of a tract often indicates its position as well as where it begins and ends
- Ex) ventral corticospinal tract
- Last part of name is where it ends
- Ex) ventral corticospinal tract
- Ascending tracts (sensory information)
- Sensory information from cutaneous receptors, proprioceptors (muscles and joints), and visceral receptors
- Most of the sensory information crosses over
- Analyzed by opposite side of brain
- Sensory information proceeds up the spinal tract along 3 main tracts:
- 1) Dorsal columns
- Touch, pressure, vibration, proprioception
- 2) Spinothalamic tracts
- Pain, temperature, ith
- 3) Spinocerebral tracts
- Proprioception
- 1) Dorsal columns
- Descending tracts (motor information)
- 1) Pyramidal (corticospinal)
- Descend directly, without synapses, from cerebrum to spinal cord
- Cross over
- Fine movements
- Voluntary muscular movements
- 2) Extrapyramidal
- Originate in mid/hindbrain
- Many synapses
- Involuntary movement
- Maintains posture
- Parkinson’s and ALS
- 1) Pyramidal (corticospinal)
Lecture 6: The Peripheral and Autonomic Nervous Systems
- Cranial and Spinal Nerves
- Cranial and spinal nerves
- Includes 12 pairs of cranial nerves and 31 pairs of spinal nerves
- Certain cranial nerves are purely sensory
- Most cranial nerves are both sensory and motor
- Motor only
- Trochlear, abducens, accessory, and hypoglossal nerves
- All spinal nerves are both
- Cranial nerves
- Of the 12 pairs, 2 originate in forebrain and ten in the midbrain and hindbrain
- Numbering system (Roman numerals) refers to the position order (front to back)
- Name often indicates structure(s) innervation or principal function
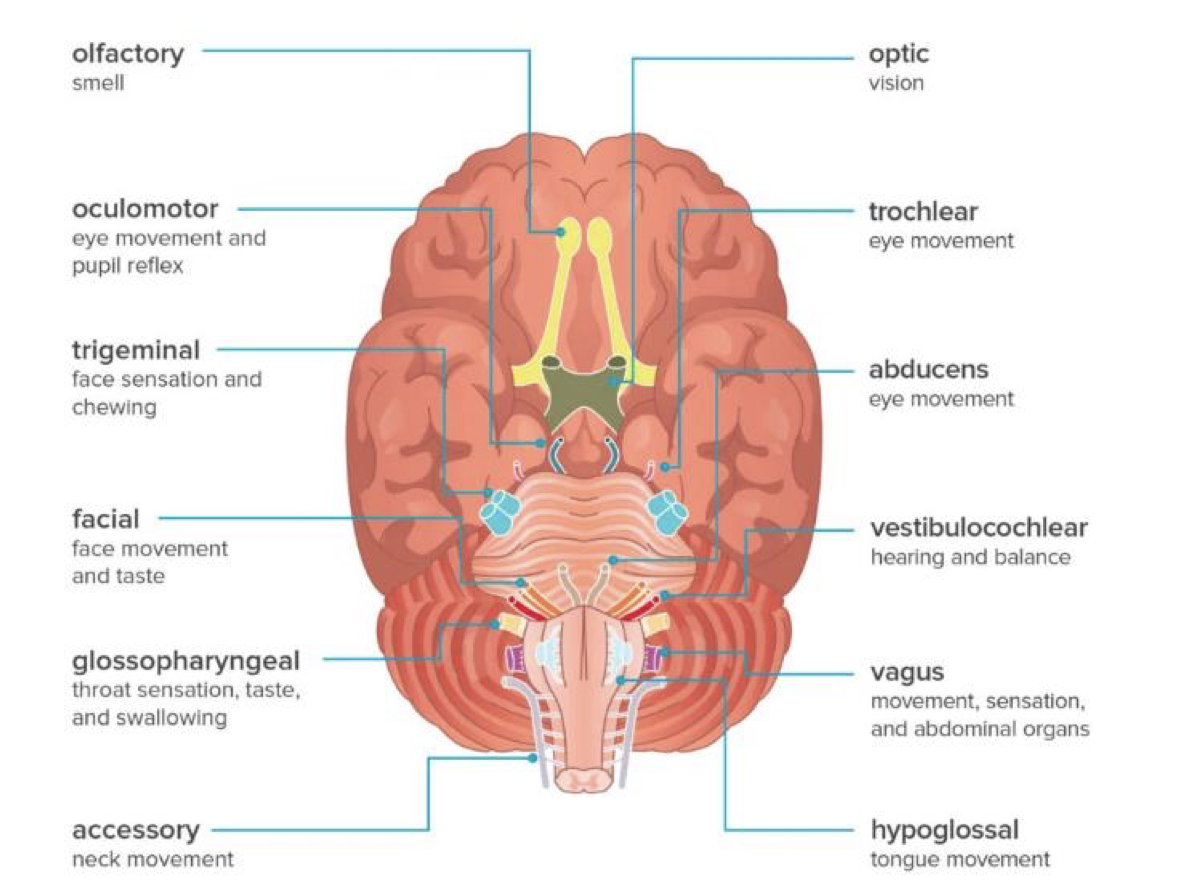
- Cranial nerves order
- Think “oh oh oh to touch and feel very good velvet ah”
- Olfactory
- Optic
- Oculomotor
- Trochlear
- Trigeminal
- Abducens
- Facial
- Vestibulocochlear
- Glossopharyngeal
- Vagus
- Accessory
- Hypoglossal
- Clinical significance
- Often part of a neurological exam
- Series of tests that checks the functionality of each nerve
- Eye movement, taste, hearing, smell, etc
- A number of things can affect them including:
- Compression
- Results from a number of causes
- inhibits/prohibits neural transmission
- Stroke
- Symptoms may indicate where occlusion of blood vessels occurred
- Inflammation
- May impair function of any of the cranial nerves
- Compression
- Often part of a neurological exam
- Spinal nerves: come out of each vertebrae
- The 31 spinal nerves are grouped into:
- 8 cervical
- 12 thoracic
- 5 lumbar
- 5 sacral
- 1 coccygeal
- The 31 spinal nerves are grouped into:
- Let’s take a closer look at a spinal nerve:
- After they emerge, spinal nerves branch to form network of peripheral nerves
- The posterior branch of each spinal nerve services the skin and musculature of the posterior trunk
- The anterior branch of each spinal nerve services the upper and lower limbs plus the abdomen
- Reflex arcs
- The functions of the sensory input and motor output of the sensory nerves is best illustrated by a reflex arc
- Unconscious motor response to sensory stimulus
- Ex) stretch reflex
- Sensory receptors move information along sensory neurons to the spinal cord. An interneuron sends motor information along motor neurons to the muscle
- The functions of the sensory input and motor output of the sensory nerves is best illustrated by a reflex arc
- The Autonomic Nervous System
- ANS
- Helps regulate activity of cardiac and smooth muscle, glands
- Involuntary
- The autonomic nervous system was originally thought to function “autonomously”
- Operates without conscious control
- Probably can’t consciously slow down heart, but deep breathing or anxiety will change rate
- Subconsciously regulated
- For this reason, a number of autonomic responses form the basis for polygraphs (lie detector tests)
- Operates without conscious control
- Autonomic neurons
- ANS is purely a motor system
- Leave CNS (mainly spinal cord) with somatic motor neurons
- Difference is that 2 neurons are involved
- Preganglionic and postganglionic neuron
- Visceral effector organs
- The autonomic nervous system is integral to maintaining homeostasis in the body
- Involved in endocrine regulation, smooth muscle function, circulation, heart function, digestion, and many other systems
- Smooth muscle maintains resting tone in absence of nerve stimulation
- Denervation hypersensitivity
- Damage will make target more sensitive to stimulating agents
- The autonomic nervous system is integral to maintaining homeostasis in the body
- In addition to their “built in” muscle tone, cardiac and many smooth muscles are stimulated by the muscles themselves
- Contract rhythmically
- ANS simply increases or decreases intrinsic activity
- Ex) stimulation by the ANS can either increase or decrease the heart rate
- Divisions of the ANS
- Sympathetic
- Originate in thoracic and lumbar regions of spinal cord
- Preganglionic fibers tend to be short
- Ganglia lie in sympathetic ganglion chain
- Long postganglionic fibers
- Parasympathetic
- Originate in cranial (brain) and sacral regions (spinal cord)
- Preganglionic fibers tend to be longer
- Ganglia lie near effector organs
- Short postganglionic fibers
- Sympathetic
- Fight-flight or rest-digest
- Sympathetic: fight-flight
- Parasympathetic: rest-digest
- Neurotransmitters
- Acetylcholine released from all preganglionic fibers AND all parasympathetic postganglionic fibers
- Cholinergic fibers
- Noradrenaline released from most sympathetic postganglionic fibers
- Adrenergic fibers
- Acetylcholine released from all preganglionic fibers AND all parasympathetic postganglionic fibers
- Responses to cholinergic stimulation
- Release acetylcholine as neurotransmitter
- Cholinergic responses of somatic motor neurons and preganglionic autonomic neurons are always excitatory
- Cholinergic responses of postganglionic autonomic neurons are usually excitatory
- Parasympathetic fibers innervating heart cause slowing of heart rate
- Responses to adrenergic stimulation
- By epinephrine in the blood and norepinephrine from sympathetic nerve endings
- Has both excitatory and inhibitory responses
- Heart, smooth muscles of many blood vessels: contract
- Bronchioles, some blood vessel: dilate
- Different responses depend on receptors on cells
- Drugs developed take advantage of this
- Can either promote or inhibit effects
- Many illnesses act by affecting the release of these neurotransmitters
- Black widow venom
- Triggers explosive release of ACh at all cholinergic sites
- Prolonged depolarization of diaphragm results in respiratory failure
- Botulism
- Blocks release of ACh
- Prevents muscles from responding to nerve impulses
- Death due to respiratory failure
- Curare
- Blocks effect of release ACh
- Paralysis
- Death due to respiratory failure
- Black widow venom
- The sympathetic and parasympathetic systems affect most of the visceral organs
- Effects are usually opposite to each other
- Ex) Sympathetic stimulation increases HR, parasympathetic decreases it
- Ex) Sympathetic slows down digestion, parasympathetic speeds it up
- In general, sympathetic system promotes responses that prepare the body for strenuous activity
- Emergency or stressful situations
- Often called “fight or flight”
- Parasympathetic system allows body to focus on its own housekeeping duties
- Quiet and restful situations
- Often referred to as the rest-and-digest response
- Enteric nervous system (ENS)
- 3rd branch, often overlooked
- Millions of neurons in plexes that extend the length of the GI tract
- Part of the ANS that actually includes sensory neurons
- Provide information (such as stretching) to motor neurons
- Despite sensory function, considered to be part of the “motor only” ANS
- What does the ENS do?
- Controls movement: peristalsis and segmentation
- Fluid exchange: between gut lumen and tissue fluid compartments
- Gastric and pancreatic secretion: regulated by both neurons and hormones
- Defense reactions: diarrhea and vomiting
- Control of ANS
- Visceral functions largely regulated by autonomic reflexes
- Sensory input transmitted to brain, information integrated, preganglionic autonomic neurons
- What neural centers of the brain control the activity of autonomic neurons?
- Medulla oblongata - almost all responses initiated here
- Centers for control of cardiovascular, pulmonary, urinary, reproductive, and digestive systems
- Hypothalamus
- Medulla itself is responsive to higher brain centers
- Most important is the hypothalamus
- Body temperature, hunger, thirst
- Limbic system
- Forms ring around brain stem
- Controls visceral responses related to many emotional states
- Blushing, pallor, fainting, breaking out in cold sweat, racing heartbeat, “butterflies”
- Cerebellum
- Causes motion sickness
- Nausea, sweating, cardiovascular changes
- Medulla oblongata - almost all responses initiated here
- Visceral functions largely regulated by autonomic reflexes
Lecture 7: Sensory Systems
- General properties
- General properties of sensory systems
- Each sensory receptor responds to an environmental stimulus by causing an action potential in a sensory neuron
- Receptors change different forms of energy into energy that can be interpreted by the brain
- Thus, vision and sound stimulate regions of the brain the same way even though they are interpreted differently
- Sensory receptors are categorized by the type of energy they convert
- Chemoreceptors
- Respond to chemicals
- External: taste and smell
- Internal: O2, CO2, pH, glucose, etc
- Mechanoreceptors
- Respond to stimuli that deform plasma membrane of receptor
- Pressure, vibration, acceleration, sound
- Ex) cochlea head about 16000 mechanoreceptors
- Photoreceptors
- Respond to photons of light
- Rods and cones
- Ex) eyes has about 126 million photoreceptors
- Thermoreceptors
- Respond to varying degrees of heat
- Most of these are found in the skin
- Some found internally to regulate body temperature
- Chemoreceptors
- Sensory adaptation
- Receptors response with a burst of energy when stimulus is first applied
- Some quickly decrease firing rate - phasic receptors
- Cease paying attention to constant stimuli
- Ex) odor, touch, temperature (think: noseblind)
- Others don’t
- Tonic receptors (such as pain)
- Skin
- Skin: sensory receptors
- There are several types of sensory receptors in the skin
- Each designed to be maximally sensitive to one type of sensation
- Touch, pressure, heat, cold, pain
- In some cases, sensations picked up by free nerve endings
- In other cases nerve endings are encapsulated
- There are several types of sensory receptors in the skin
- Free nerve endings
- Temperature sensed by thermoreceptors in top part of dermis
- 2 kinds: heat and cold receptors
- Many more cold receptors, fewer heat receptors
- Pain receptors activated above 45C
- Cold receptors not activated below 5C
- Numb
- Many more cold receptors, fewer heat receptors
- Nociceptors
- Free sensory dendrites
- Activated by a variety of noxious stimuli
- Chemical, mechanical, thermal
- Have the potential to cause tissue damage
- Often referred to as pain receptors
- But pain is a perception, not a stimulus!
- Also “itching” sensation activated by the receptors
- Can be myelinated (pin prick- fast response) or unmyelinated (dull ache - slow response)
- Found not only in skin, also in muscles, joints, almost everywhere in the body except the brain!
- Triggered by injury
- Internally, are more frequent in hollow organs
- GI tract, bladder, etc
- More likely to come into contact with noxious substances
- Touch and pressure
- Free nerve endings around hair follicles
- 1) Ruffini endings
- Heavy pressure
- Adapt slowly to stretching
- 2) Merkel’s discs
- Sustained pressure or light touch
- Adapt slowly
- 3) Meissner’s corpuscles
- Fine touch, quick adapting
- Also called tactile receptors
- 4) Pacinian corpuscles
- Quick adapting
- Deeper, pressure
- Different types of receptors work in concert
- Very refined sense of touch
- Nociceptors located near surface
- Merkel’s discs and Meissner’s corpuscles in upper layers
- Can localize gentle touch
- Pacinian corpuscles, Ruffini endings in lower layers
- Respond to deeper touch
- Density of mechanoreceptors
- Some types of receptors have wide receptive fields
- Less precise reception
- Some have smaller ones
- Much denser, more sensitive
- Ex) fingertips have many receptors and small receptive fields, back of legs have fewer receptors and wider receptive fields
- Some types of receptors have wide receptive fields
- Muscles and Joints: Proprioceptors
- Muscles and Joints: proprioceptors
- Receptors in muscles, joints, tendons, ligaments
- Provide sense of body position
- Allow fine control of body positions
- Information about stretching, contraction and position
- All sensory input from the proprioceptors goes to the cerebellum
- Proprioceptors are one of 2 types:
- Muscle spindles
- Detects changes in muscle length
- Small sensory organs that are enclosed within a capsule
- Found throughout the body of a muscle
- Stretching of muscle fibers triggers action potential
- Golgi tendon organs
- Located in tendons that connect muscle to bone
- Interwoven with collagen fibers
- Provides information on tension
- Muscle contraction better stimulus for Golgi tendon organ
- Muscle spindles
- Taste and Smell: Chemoreceptors
- Taste and smell: chemoreceptors
- Internal environment: interoceptors
- External environment: exteroceptors
- Smell and taste both involve chemoreceptors
- One of the oldest senses (chemoreception) from an evolutionary perspective
- Smell: gaseous molecules in the air
- Taste: chemicals dissolved in food and drink
- Distinction is arbitrary: both must be dissolved in water
- Taste
- Receptor cells clustered together in taste buds
- Primarily on surface of tongue
- Sour: presence of H+
- Salty: presence of Na+
- Sweet and umami: organic molecules associated with nutritious food
- Bitter: organic molecules associated with toxic effects
- Each taste cell is a non-neural epithelial cell
- Can become depolarized under appropriate stimulation
- Microvilli project from surface
- Bathed in saliva
- Release neurotransmitters that stimulate associated sensory neurons
- Taste buds innervate one of 2 cranial nerves: facial and glossopharyngeal
- Smell
- Receptors responsible for smell consist of dendrites of several million bipolar sensory neurons
- Axons form the first cranial nerve (olfactory nerve)
- Olfactory bulb synapses with secondary neurons in olfactory bulb
- Leads to olfactory tract and olfactory cortex
- Unique among neurons of an adult
- Replace themselves every 1-2 months
- Each sensory neuron has multiple cilia
- Odorant molecules bind to receptors on these cilia
- About 400 different receptors
- By combining information, humans can detect about 10000 smells
- The olfactory bulb is part of the limbic system
- Important role in generating emotions and in memory
- Amygdala is particularly important in generating emotional responses to smell
- Hippocampus stores memories associated with a particular smell
- Equilibrium and Hearing: Mechanoreceptors
- Equilibrium
- Sense of equilibrium provided by vestibular apparatus of inner ear
- Otolith organs (utricle and saccule)
- Ampullae of semicircular canals
- Sensory cells are located within these
- Hair cells
- Hair cells
- Modified epithelial cells
- About 50 hair-like extensions
- All but one are stereocilia
- Larger one is a kinocilium
- Stereocilia bend in direction of kinocilium, cell membrane depolarizes, neurotransmitter released, stimulates dendrites of vestibulocochlear nerve
- Stereocilia bend away from kinocilium, cell membrane hyperpolarizes, less neurotransmitters, less stimulation
- Utricle and saccule
- Each has a patch of specialized epithelium
- Macula
- Hair cells and support cells
- Hair cells embedded in otolithic membrane
- Contains microscopic crystals (otoliths)
- Utricle: horizontal movements
- Saccule: vertical movements
- Each has a patch of specialized epithelium
- Semicircular canals
- 3 semicircular canals project at different angles
- At the base of each is an ampulla
- These are where the sensory hairs are located
- Embedded in a gelatinous membrane
- Cupula contains hair cells
- Hairs can be pushed in both directions
- Semicircular canals: rotational movements
- Hearing
- Sound causes vibrations of the tympanic membrane
- These produce movements of the inner ear ossicles
- Press against oval window of cochlea
- Pressure waves in cochlea cause movements of basilar membrane
- Sensory cells located here
- Cross-section of the cochlea
- Sound waves at oval window displace fluid in Scala vestibuli
- The fluid wave then travels from Scala vestibuli to Scala tympani
- Sound frequencies are picked up in different regions of the cochlea
- If the sound frequency (pitch) is low
- Pressure waves travel a long way
- Up the scala vestibuli and back down the scala tympani
- If the sound frequency high
- Transmitted through vestibular membrane and basilar membrane to scala tympani
- If the sound frequency (pitch) is low
- Movement of basilar membrane central to pitch discrimination
- Sounds of higher frequency cause maximum vibrations of basilar membrane closer to the oval window
- Organs of Corti
- Sensory hairs are located on the basilar membrane
- Hairs project into cochlear duct
- Embedded in tectorial membrane
- This is the functional unit of hearing and is called the Organ of Corti
- The greater the displacement of the basilar membrane, the greater the neurotransmitter release by the hair cells
- Sensory hairs are located on the basilar membrane
- Vision: Photoreceptors
- Vision: photoreceptors
- Light from observed object is focused on photoreceptive retina at back of eye
- What do we see?
- The sensory cells in the retina convert electromagnetic energy into nerve impulses
- Light of longer wavelengths (IR) insufficient energy to excite receptors
- Lights of shorter wavelengths (UV) filtered out by lens
- Can be seen by many animals
- The lens focuses the image
- Rays of light are refracted to a point on the retina
- Ability to keep objects at different distances focused is called accommodation
- Results from contraction of ciliary muscle
- Like a sphincter
- When object is far away
- Ciliary muscle is relaxed
- Tension on suspensory ligaments increases
- Lens pulled taut
- As object gets closer, muscles of ciliary body contract
- Tension on suspensory ligaments decreases
- The retina contains the photoreceptive cells
- 2 types of photoreceptive neurons:
- Rods: black-and-white vision under low intensity light
- Cones: sharp color vision when light intensities greater
- The retina consists of rod and cones and well as other neuron layers
- Objects usually fall of fovea
- Contains only cones
- 2 types of photoreceptive neurons:
- Effect of light on rods
- Rods contain a purple pigment
- Rhodopsin
- Dissociates into 2 components when stimulated by light
- Initiates changes in cell membrane permeability
- Ultimately results in production of nerve impulses
- Rods contain a purple pigment
- Effect of light on cones
- Less sensitive to light but provide color vision and greater visual acuity
- 3 types of cones
- Each contains proteins called photopsins
- Red, green, blue
- Each absorbed different wavelengths
- Less sensitive to light but provide color vision and greater visual acuity
- Neural pathways
- Approximately 120 million rods, 6 million cones in each retina, 20:1 ratio
- Only about 1.2 million nerve fibers
- Therefore, there are about 105 photoreceptors for each nerve cell
- Cones adapt quickly to changes in light
- In fovea, visual acuity is highest, all cones
- In the eyes, the lens focuses the light on the retina
- Rods and/or cones activated
- Signal sent through bipolar cells to ganglion cells
- It is the axons of the ganglion cells that make up the optic nerve
- The right visual field goes to left side of both retinas
- These both get the same image
- This image crosses over to the left thalamus from the right eye
- Goes directly to the left thalamus from the left eye
- Left geniculate nucleus (in thalamus) therefore receives input from both eyes that relates to right half of visual field
- About 80% of axons from retina continue on to visual cortex in occipital lobe of brain
- Interpretation of information
- What is it?
- The other 20% go to optic tectum of midbrain
- Where is it?
- Interpretation of information
- Approximately 120 million rods, 6 million cones in each retina, 20:1 ratio
- Interoceptors
- Have been looking at exteroceptors (except proprioceptors!)
- Sensory receptors that provide information about exterior environment
- There are also many interoceptors
- Provide information about the internal environment
- Temperature, chemicals, pressure, etc
- Important for homeostasis
- Have been looking at exteroceptors (except proprioceptors!)
Topic 8: Muscle Function
A. Types and Structure of Muscle
- There are 3 types of muscle:
- Skeletal
- Striated
- Multinucleate (fused cells)
- Nuclei against cell membrane
- One cell= one fibre
- Cardiac
- Striated
- One nucleus in each cell
- Branched
- Intercalated discs
- Smooth
- Nonstriated
- Spindle-shaped cells
- One central nucleus
- Skeletal
- Let’s look at striated skeletal muscle in more detail…
- It makes up all the voluntary muscle and represents the greatest amount
- Cardiac muscle only associated with heart
- Most smooth muscle found in layers in digestive and circulatory vessels
- Let’s start with a whole muscle
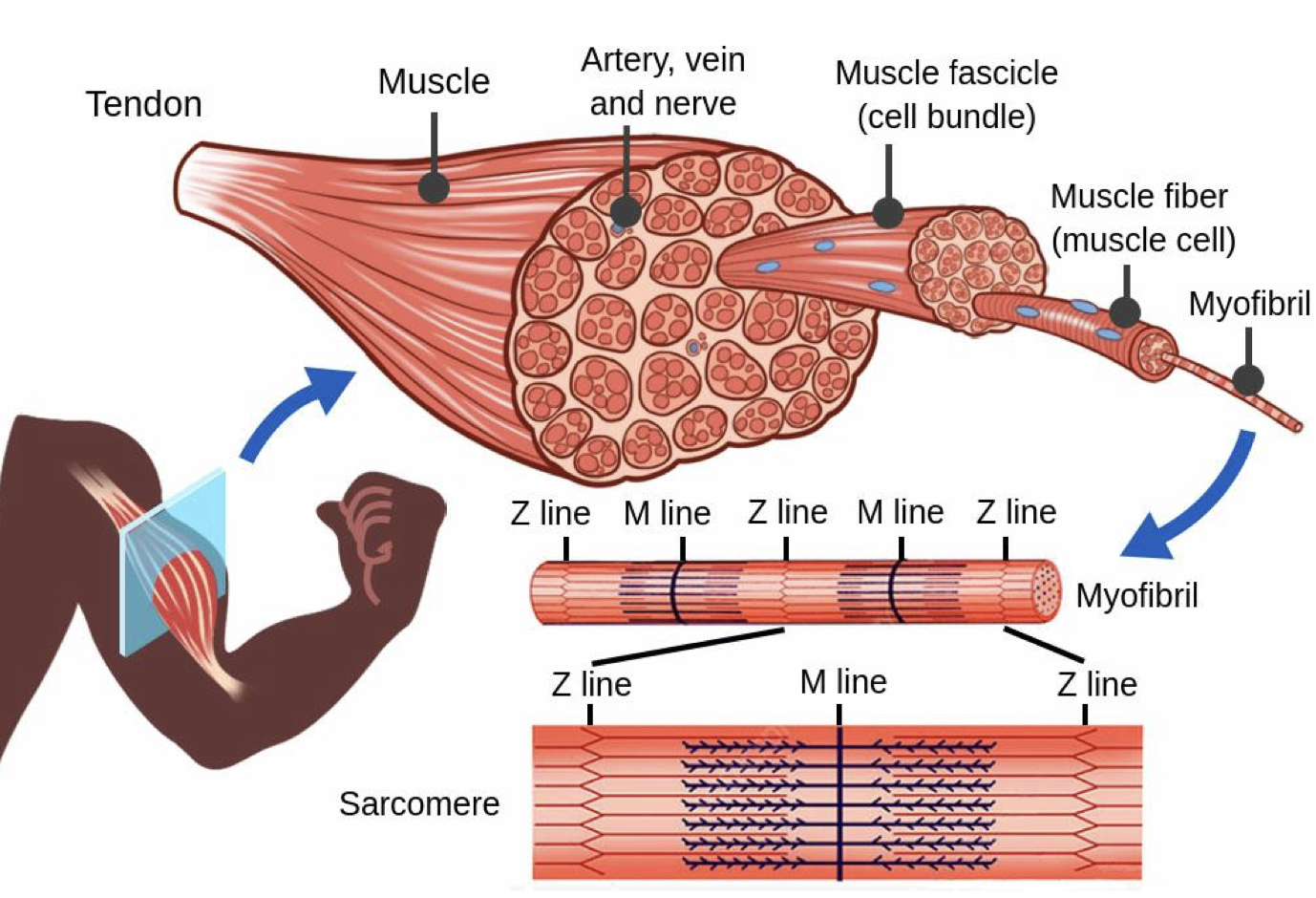
- Individual muscle fibers are very long cells
- Dozens of cm in long muscles
- Composed of many fused cells
- Many nuclei
- Each muscle fiber has many sarcomeres
- Sarcomeres are the basic unit of contraction
- Boundaries of sarcomeres make up the striations
- The way that the actin (thin filaments) and myosin (thick filaments) are arranged gives the skeletal muscle it’s striated appearance
- A bands are dark because myosin is thick
- I bands are lighter because actin is thin
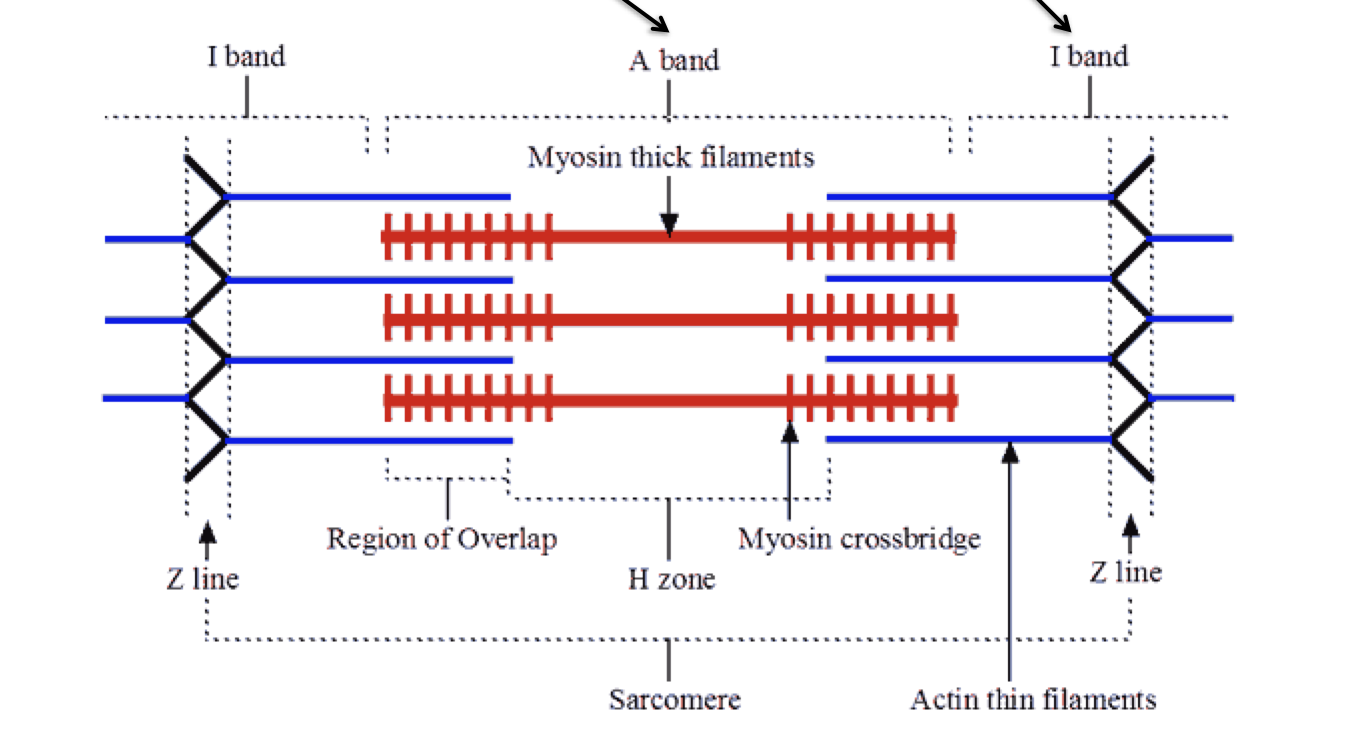
- Individual muscle fibers are very long cells
B. Skeletal Muscle Contraction
- What happens during muscle contraction?
- Actin filaments slide over myosin
- Muscle shortens
- Let’s take it right from the beginning
- Begin with a nerve impulse traveling down an axon
- How does this nerve impulse initiate muscle contraction? The neuromuscular junction
- The neuromuscular junction
- Site at which axon of a motor neuron contacts the muscle fiber that it innervates
- Synaptic bulb contains synaptic vesicles
- Filled with acetylcholine (ACh)
- When action potential reaches axon terminal:
- Molecules of ACh released into synaptic cleft
- Bind to receptors on the muscle membrane (the motor end plate)
- The binding of ACh to receptors activates sodium channels
- Na+ enters cell
- Produces local depolarization
- Initiates electrical signal in muscle
- This electrical signal then passes to the t-tubule of the muscle
- Signal passes to inside of muscle along T-tubules
- T-tubules are extensions of sarcoplasmic reticulum
- Results in calcium channels opening
- This calcium is released to interact with actin and myosin fibers
- So, how does Ca2+ initiate contraction? We need to look at myosin and actin in more detail and how they interact
- Myosin
- Each myosin filament has a tail and a head
- Each myosin head has 2 active regions:
- 1) Actin binding site
- 2) ATP binding site
- Actin
- Actin has 2 other proteins bound to it
- Tropomyosin
- Troponin
- The calcium ions are going to enable the actin and myosin to bind together and initiate the contraction of the sarcomere
- Actin has 2 other proteins bound to it
- Muscle relaxation/contraction
- Muscle is relaxed:
- Actin and myosin remain unattached
- Tropomyosin prevents attachment to myosin
- Muscle contracts:
- Calcium binds to troponin
- Tropomyosin moves out of the way
- Head of myosin attaches to actin (cross bridge)
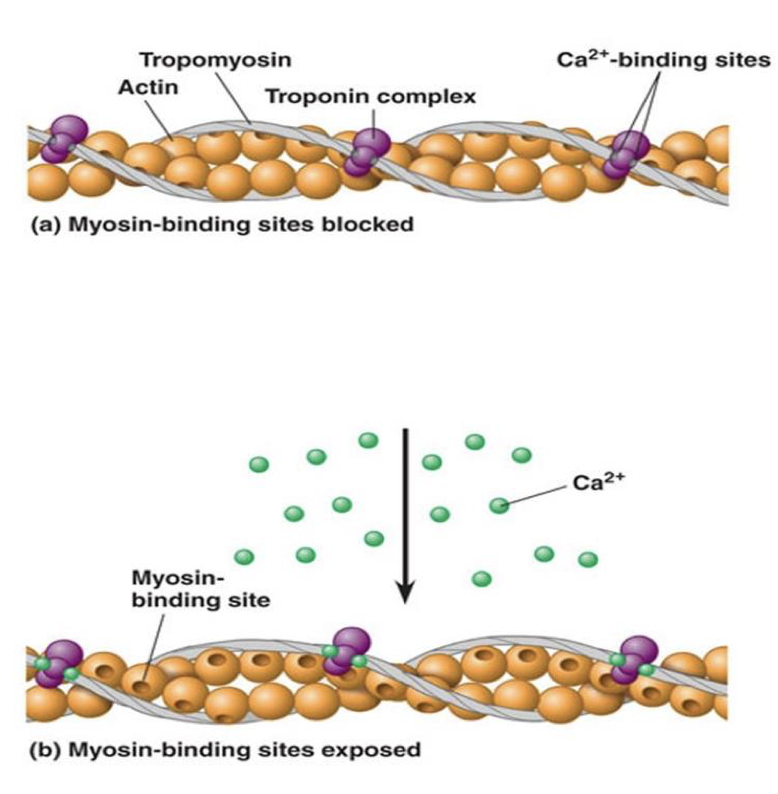
- Muscle is relaxed:
- Now that myosin and actin are attached, what happens?
- The attachment of myosin head to actin causes bending of myosin to center of sarcomere
- Shortens the sarcomere segment
- Often referred to as the “power stroke”
- Cross bridges are like little arms that pull thin filaments over thick ones
- But one power stroke can’t pull actin filaments very far
- Like “tug-of-war”
- What happens when the power stroke is over?
- Muscle has only shortened by 1%
- Muscles can shorten up to 60%
- Cross bridges have a “cross-bridge cycle”
- Once power stroke is over, ATP binds to myosin head
- Myosin head detaches from actin
- New power stroke begins
- Therefore, one ATP is required for the breaking up of the cross bridges after the power stroke
- The attachment of myosin head to actin causes bending of myosin to center of sarcomere
- The cross-bridge cycle
- 1) cross bridges formed between myosin and actin and myofilament
- 2) once the crossbridge forms, the myosin performs a power stroke pulling the actin myofilament
- ADP and Pi are released
- 3) New ATP attaches to myosin head and cross bridge detaches
- 4) Myosin uses ATP to return to its erect state
- Sarcomere contraction
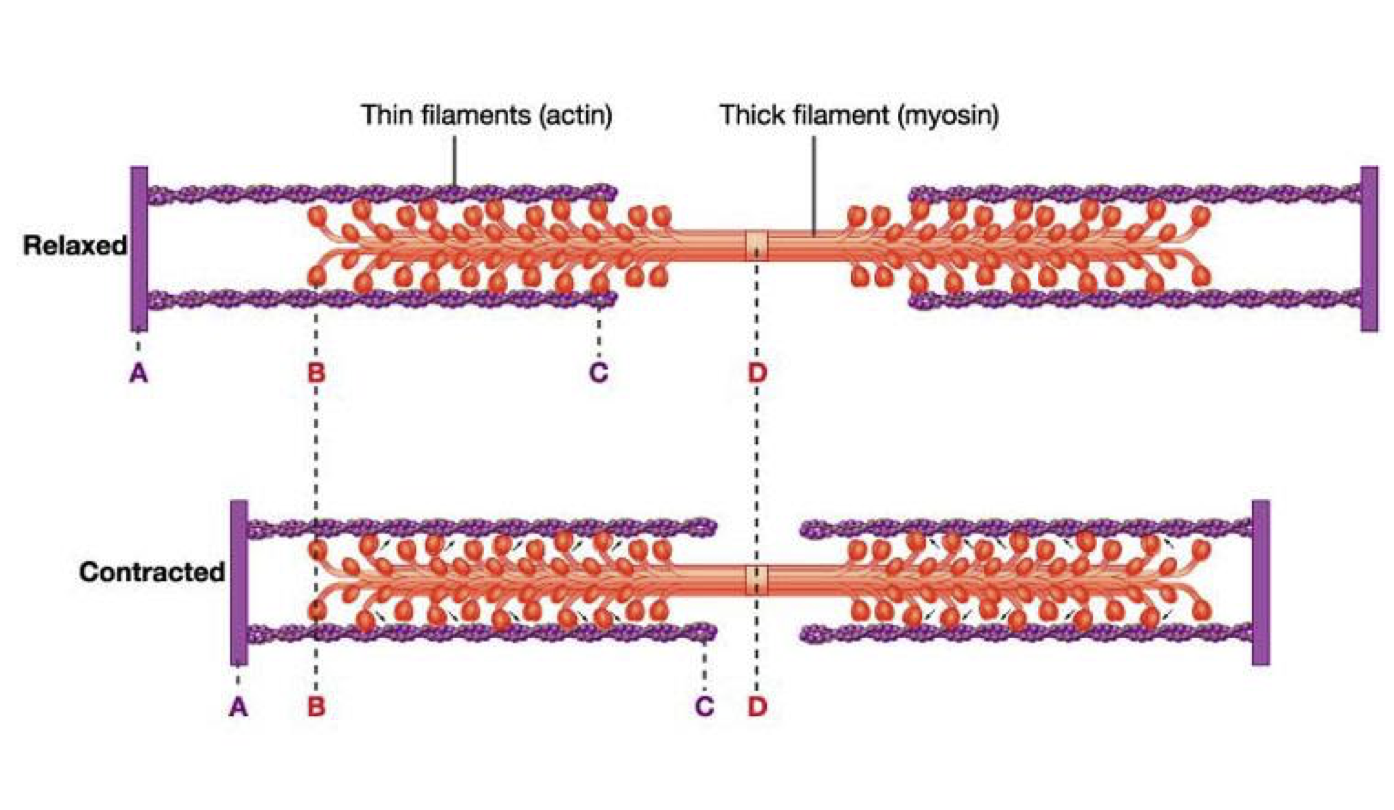
- Muscle contraction: Step by step
- 1) nervous system stimulates muscle fiber
- Calcium released by sarcoplasmic reticulum
- 2) due to conformational change caused by Ca+ myosin heads connect to actin
- Cross-bridge formed
- 3) head pulls actin fiber over myosin fiber; cross bridge broken
- Cost of detachment = 1 ATP
- 4) attachment sites form and break many times during a contraction
- Cross-bridge recycles
- 5) occurs at the same time in all sarcomeres in the cell
- 6) muscle cell shortens, entire muscle shortens
- 1) nervous system stimulates muscle fiber
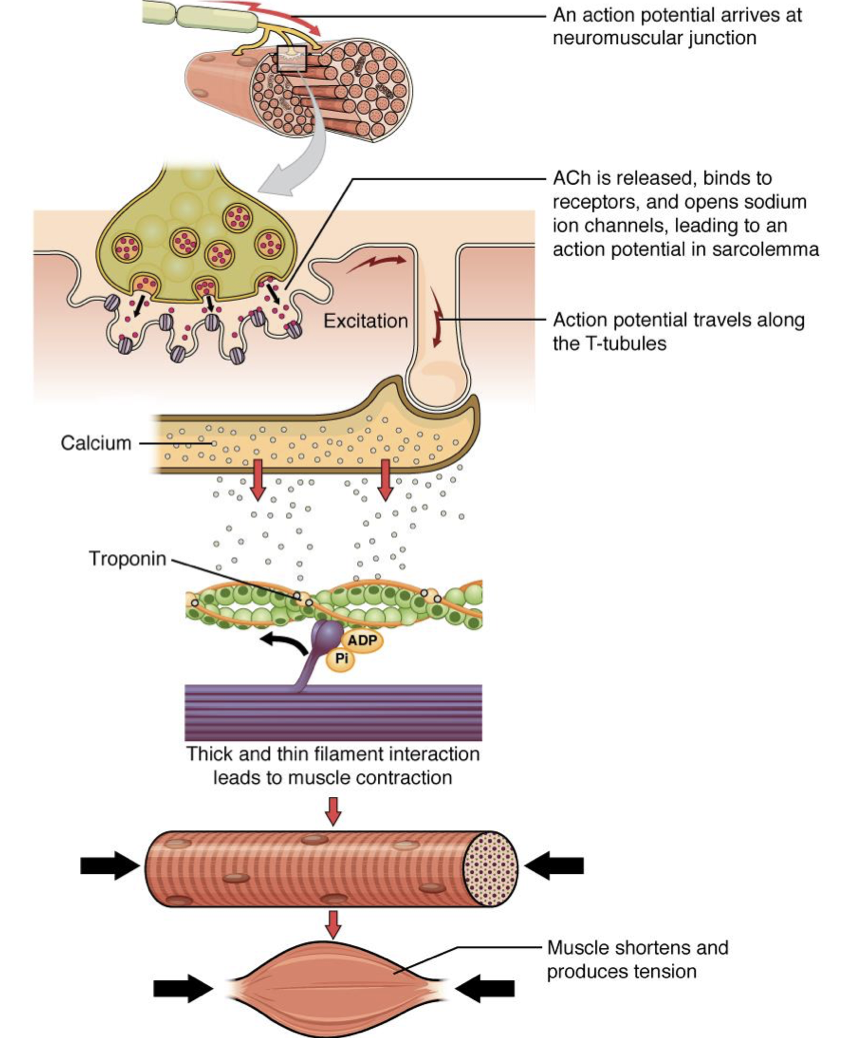
- Rigor mortis
- ATP is required to remove the head of the myosin from the actin molecule
- After death, ATP synthesis stops
- Therefore, myosin and actin cannot separate
- Causes the muscles to become stiff
- Breakdown of myosin heads eventually leads to flaccidity again
C. Stimulation and Strength of Contraction
- Muscle stimulation/strength of contraction
- Contraction of muscles must vary in strength and duration
- However, all muscle contractions are built on the simple muscle twitch
- The muscle twitch is “all-or-none”
- But rarely, if ever, get a single cell activated
- The muscle twitch is “all-or-none”
- Motor unit
- Consists of one neuron and all the muscle fibers that to which it connects
- A signal from that neuron will result in all fibers contracting
- Several hundred or very few muscle fibers may be stimulated by one nerve
- Fewer muscle fibers=more control over movement
- Consists of one neuron and all the muscle fibers that to which it connects
- What happens when a signal is sent?
- Latent period:
- 1st few milliseconds
- Connections between actin and myosin begin to form
- Contraction:
- Actin slides over myosin
- Muscle shorten
- Relaxation:
- Muscle returns to initial length
- This is highly reproducible!
- Latent period:
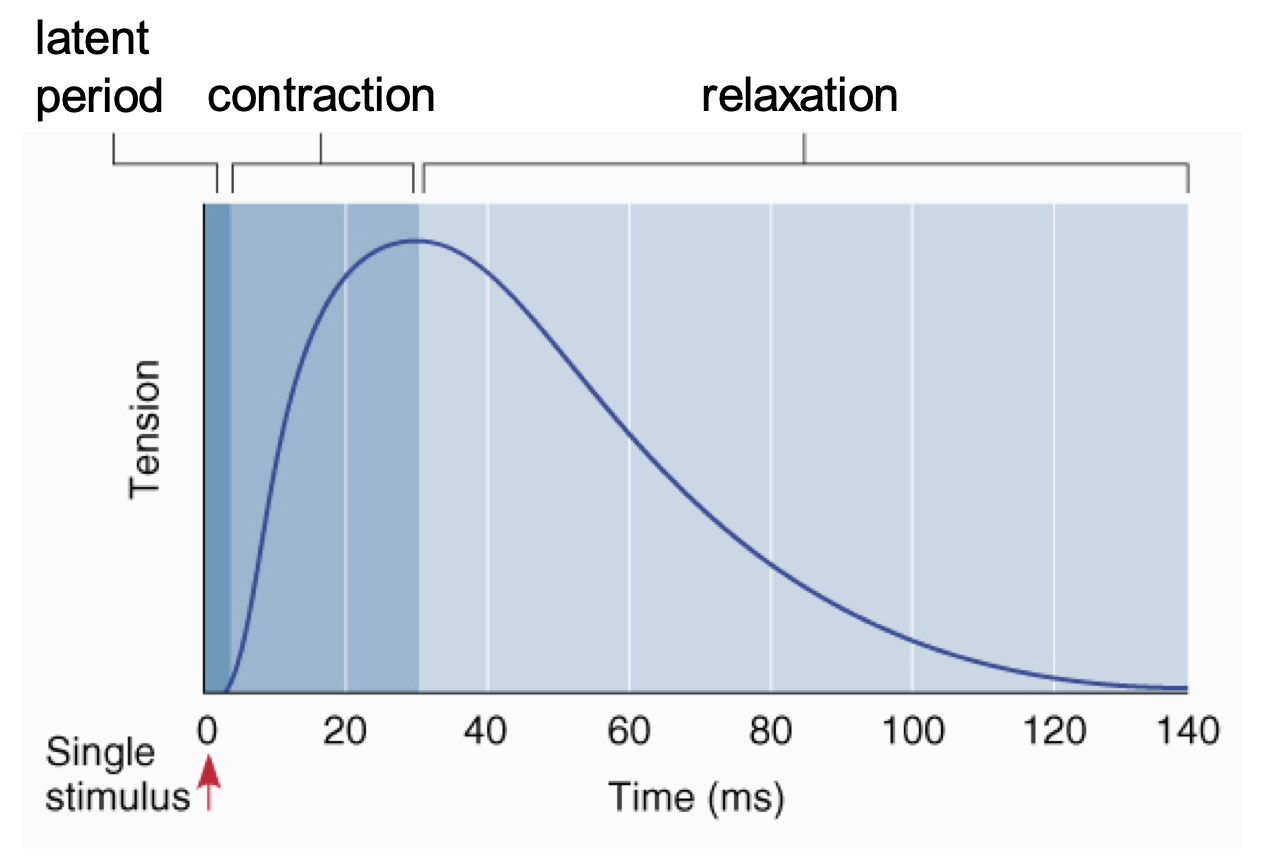
- Although twitches are reproducible for any given muscle fiber, they may still vary
- One reason: muscle fibers with a larger diameter are stronger
- Another reason: some fibers vary in the speed in which they can achieve peak force
- Slow and fast twitch fibers
- Despite these differences, if that’s all that happened, we’d be very twitchy
- Need to better control our muscle contractions
- There are 3 important factors that modify muscle contraction
- Isometric vs isotonic contractions
- The frequency of stimulation
- The strength of stimulation
- Isometric vs isotonic contractions
- Do not differ in how force is generated but rather if the muscle gets shorter
- Isotonic: muscle gets shorter
- Same tension, changing length
- Isometric: muscle stays the same length
- Same length, changing tension
- Isotonic: muscle gets shorter
- If the muscle contracts isometrically, sarcomeres still shorten
- Whole muscle does not
- Force transmitted through certain cellular components and tendons
- Good for maintaining posture, etc
- Do not differ in how force is generated but rather if the muscle gets shorter
- The frequency of stimulation
- Muscle twitches reproducible only if a muscle is stimulated at low frequency
- By increasing the frequency of signals sent to the muscle, get a stronger response
- Second signal added to the first signal
- More calcium=more myosin binding sites=more cross bridges=more tension generated
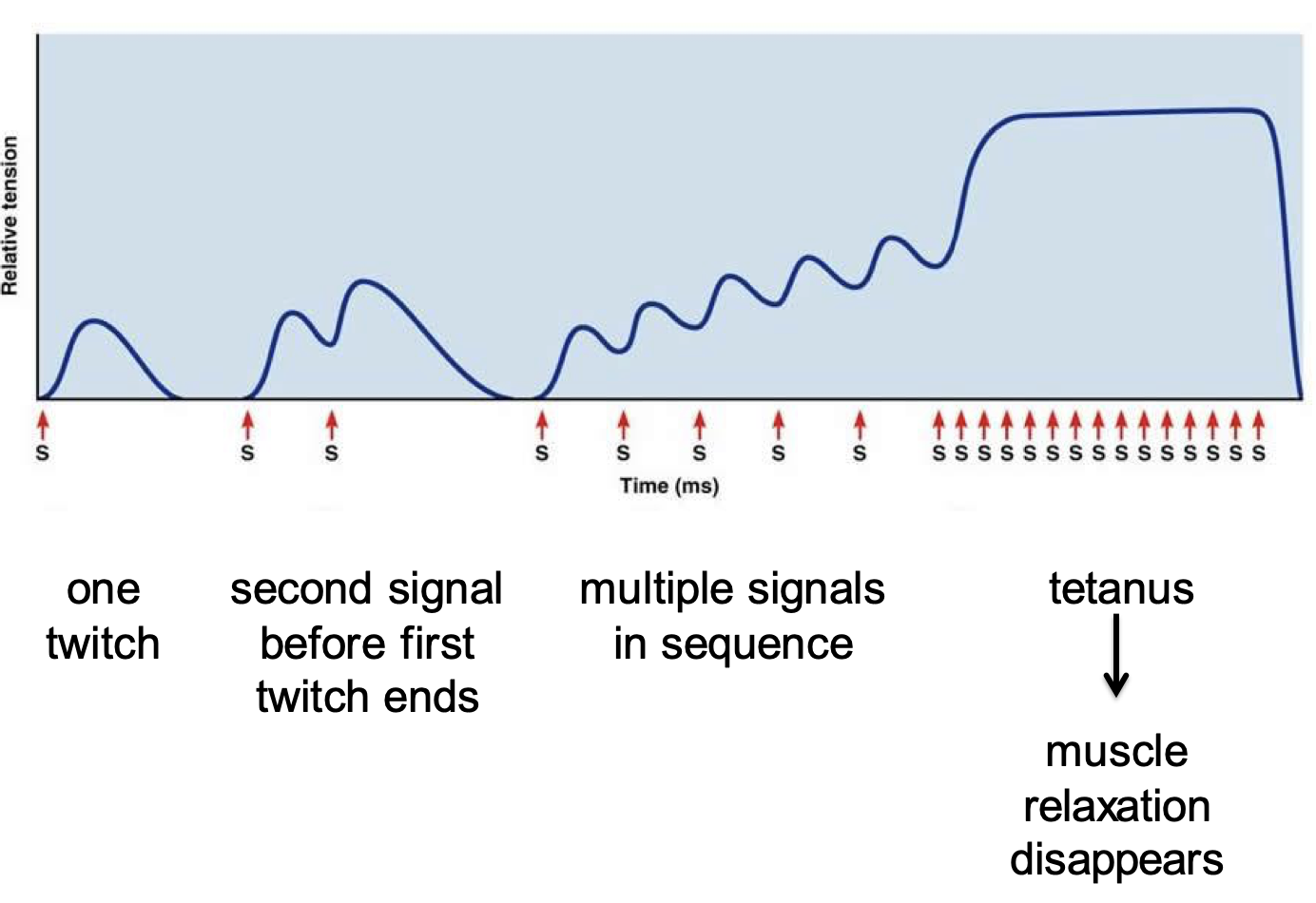
- Tetanus
- Tetanus caused by multiple stimuli to muscles not to be confused with the disease “tetanus”
- Caused by a soil bacteria
- Releases a toxin that interferes with the release of inhibitory neurotransmitter
- Continuous excitation of muscle fibers
- Early manifestations often involve the masseter muscle
- “Lockjaw”
- The strength of stimulation
- As more muscle fibers are stimulated by more neurons, strength of contraction increases
- Smallest muscle fibers stimulated first
- As more force needed, larger fibers stimulated
D. Types of Skeletal Muscle Fibers
- Slow and fast twitch fibers
- Some muscles take longer to reach peak tension during contraction
- Soleus (in the calf) muscle contains mostly slow twitch fibers
- Gastrocnemius (in the calf) has equal numbers of both
- Extraocular muscles have mainly fast twitch muscle fibers
- Difference between slow and fast twitch fibers reflects type of myosin present
- Velocity of muscle contraction depends on how quickly cross bridges recycle
- Rate limiting step is the synthesis of ATP
- Muscles with many fast twitch fibers can synthesize ATP more quickly
- Therefore, muscles shorten faster
- Fast and slow twitch muscles are good for different things
- Some muscles take longer to reach peak tension during contraction
Slow twitch | Fast twitch |
|---|---|
Efficient in using oxygen | Do not burn oxygen to create energy |
Delayed muscle firing | Fast to fire, best for explosive body movements |
Do not fatigue easily | Tire out quickly |
Best suited for: endurance sports, including cycling, marathon running and long-distance triathlons | Best suited for: short bursts of activity, including sprinting races, pole vaulting and crossfit-style events |
- Glycolytic and oxidative fibers
- Besides classifying muscles based on their speed of contraction, they can also be classified based on their metabolic properties
- All muscle fibers can produce ATP from both oxidative phosphorylation and glycolytic phosphorylation
- Differ in their capacities for doing so
- Besides classifying muscles based on their speed of contraction, they can also be classified based on their metabolic properties
Glycolytic fibers | Oxidative fibers |
|---|---|
Glycolytic enzymes high | Glycolytic enzymes low |
Few mitochondria | Rich in mitochondria |
Larger diameter | Smaller diameter |
Fewer capillaries | Lots of capillaries |
No myoglobin | Myoglobin (red) |
Produce ATP less efficiently | Produce ATP more efficiently |
White muscle | Red muscle |
- The various combinations of contractile speed and metabolic processes leads to 3 types of muscle fibers
- 1) slow oxidative: maintaining posture, aerobic endurance (running a marathon)
- 2) fast oxidative: walking, sprinting
- 3) fast glycolytic: rapid, intense movement of short duration (weight lifting, throwing a ball)
- Generally, slow oxidative fibers activated first
- Fast oxidative second
- Fast glycolytic fibers last
- Only used if muscle is generating a lot of force (high intensity exercises)
- Fatigue sets in differently for each type of muscle fiber
- Glycolytic activity generates more lactic acid
E. Cardiac and Smooth Muscle
- Cardiac muscle
- Like skeletal muscle, cardiac muscle is:
- Striated
- Contains actin and myosin arranged in sarcomeres
- Contract by sliding filament mechanism
- Unlike skeletal muscle:
- Cells are branched and interconnected
- Cells joined by gap junctions
- Myocardium behaves as a single functional unit
- A few other differences:
- The nucleus is found in the centre of the cell
- Electrical signals are generated automatically
- The gap junctions between cells stain darkly
- Intercalated disks
- Like skeletal muscle, cardiac muscle is:
- Smooth muscle
- Found in walls of blood vessels, bronchioles, digestive tract, ureters, etc
- Helps to propel contents
- Do not contain sarcomeres
- Do have a lot of actin and myosin
- Arrangement permits more stretching
- ex) Smooth muscle allows uterus to stretch up to 8x original length by end of pregnancy
- Takes much longer to initiate and terminate smooth muscle contraction
- Regulated by autonomic neurons (as opposed to motor neurons for skeletal muscle)
- Parasympathetic and sympathetic: almost always affect smooth muscle cells in opposite ways: excitatory or inhibitory
- Neural signal usually affects many cells as opposed to single cells (as with skeletal muscle)
- Gap junctions convey information between cells
- Smooth muscle tissue varies in the degree to which cells are connected by gap junctions and how they are innervated
- Single unit
- Extensively linked by gap junctions
- Innervated by few neurons
- ex) GI tract, uterus
- Multi-unit
- Few gap junctions
- Richly supplied with neurons
- ex) large respiratory airways, large arteries
- Single unit
- Found in walls of blood vessels, bronchioles, digestive tract, ureters, etc
Topic 9: Heart and Vascular Systems
A. Overview
- The vascular system
- Can be thought of as a transport system
- Takes necessary substances to specific places
- Removes waste material
- Diffusion too slow
- Responsible for O2 and CO2
- Also various nutrients
- Also various hormones
- Tightly linked to other systems such as urinary and respiratory
- Can be thought of as a transport system
- Path of blood flow
- Circulatory system consists of 2 divisions:
- 1) Pulmonary
- Takes deoxygenated blood from heart to lungs and delivers oxygenated blood back
- 2) Systemic
- Delivers oxygenated blood from heart to rest of body and takes deoxygenated blood back
- 1) Pulmonary
- Circulatory system consists of 2 divisions:
B. Cardiac Physiology
- General structure
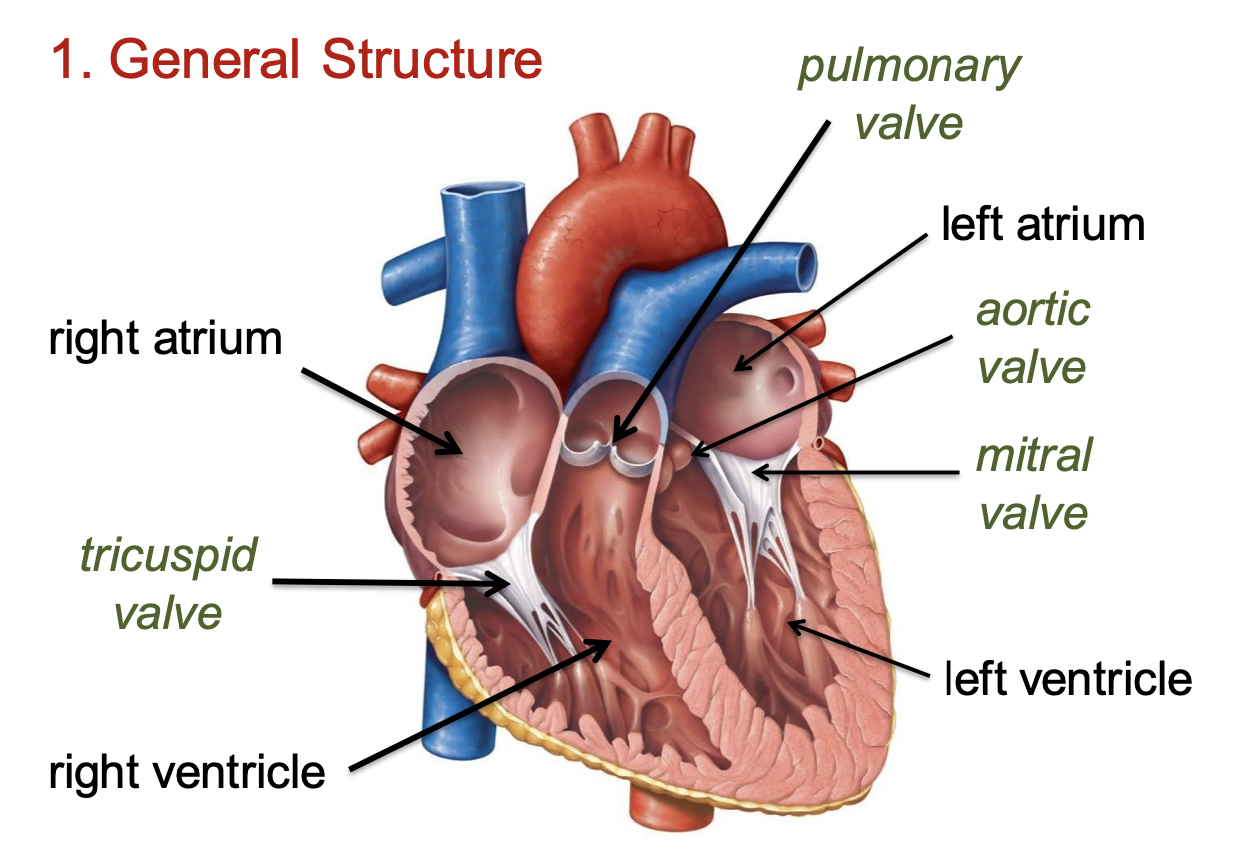
- Nervous control
- Cardiac muscle must contract in highly synchronized manner
- First both atria
- Then both ventricles
- The heart controls its own contraction
- Doesn’t rely on nervous system
- Myogenic vs neurogenic
- Can be altered by nervous system
- Two types of specialized muscle cells:
- Pacemaker cells
- Conduction fibers
- Cardiac muscle must contract in highly synchronized manner
- Pacemaker cells
- Unlike typical nerve cells, these continuously depolarize
- Generate regular action potentials
- These stimulate cardiac muscle to contract rhythmically
- Determine pace at which heart beats
- Pacemaker cells are found (mainly) in two regions
- Sinoatrial node
- Located in superior vena cava
- Rate of about 75 bpm
- Atrioventricular node
- Interatrial septa superior to ventricles
- 50 bpm
- Sinoatrial node
- Because impulses generated in the sinoatrial node are fastest, they drive the beating of the heart
- Unlike typical nerve cells, these continuously depolarize
- Conduction fibers
- Specialized to conduct quickly the action potentials generated by the pacemaker cells
- Innervate cardiac muscle cells of myocardium (muscle in heart wall)
- Larger in diameter and can conduct impulses faster
- Purkinje fibers
- Cardiac conduction system
- Main parts:
- SA node, AV node
- Bundle of HIS
- Purkinje fibers
- SA node -> atria contract -> AV node -> bundle of HIS -> purkinje fibers
- Signal creates electric current that can be seen on an electrocardiogram
- Main parts:
- How conduction works
- Sinoatrial node generates impulse -> atrial muscle contracts
- Impulse triggers atrioventricular node -> ventricular muscle contracts
- There is a brief delay between contraction of atria and ventricles
- Due to bundle of HIS
- Artificial pacemakers
- Implanted to regulate irregular contractions of the heart
- Most frequently used to increase heart rates
- Are also used in some cases to slow a fast heart rate
- The electrocardiogram
- Electrical activity of heart is carried to the skin
- Can be recorded by surface electrodes
- The recording is called an ECG or EKG
- Electrodes attached to arms and legs
- 6 electrodes attached to chest
- Total of 12 leads to detect pattern of electrical activity
- Electrical activity of heart is carried to the skin
- The EKG has 3 basic parts:
- P wave: depolarization of atria
- QRS complex: depolarization of ventricles
- T wave: ventricular repolarization
- What is happening electrically?
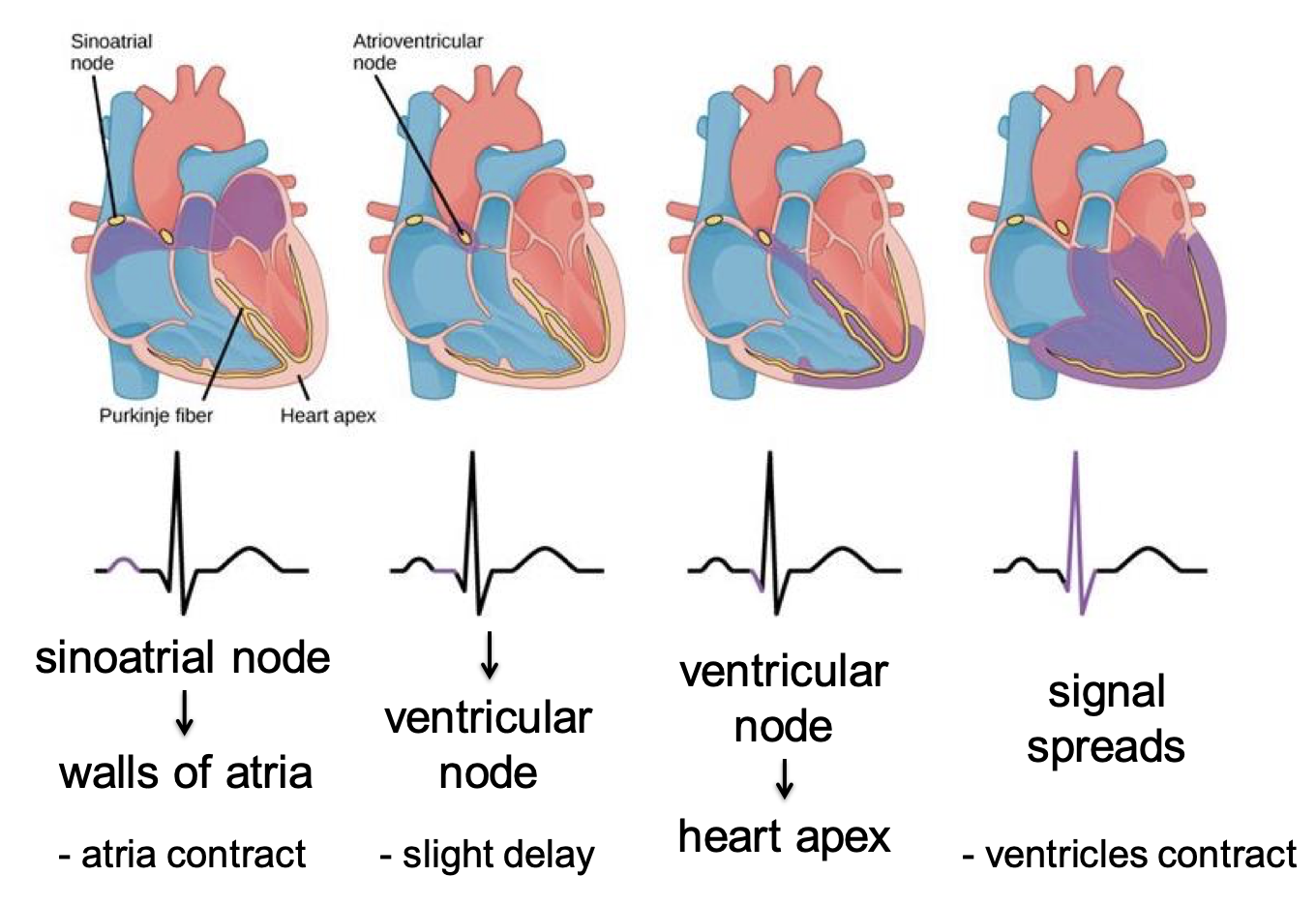
- Heart Arrhythmia
- Caused by defects in this process
- Irregular beating of the heart
- Fibrillation
- Very rapid, out-of-phase contractions
- Need to defibrillate
- Shock the heart
- Like rebooting a computer
- The cardiac cycle and heart sounds
- Involves the events of one heartbeat
- Includes both ventricular contraction and ventricular relaxation
- Therefore, the cycle can be divided into 2 major stages:
- a) Systole: ventricular contraction
- b) Diastole: ventricular relaxation
- Atria also go through contraction and relaxation at this time, but the terms really refer to ventricular events
- Ventricles contract at beginning of systole -> lub
- Ventricles relax at beginning of diastole -> dub
- Closing of AV (mitral) and semilunar (aortic) valves produce characteristic sounds
- Phonocardiogram
- Detects and records heart sounds
- 4 sounds are usually produced by the heart
- Only 2 are ordinarily audible
- Can hear 4 with stethoscope
- 4 valves
- Wiggers diagram: putting it all together
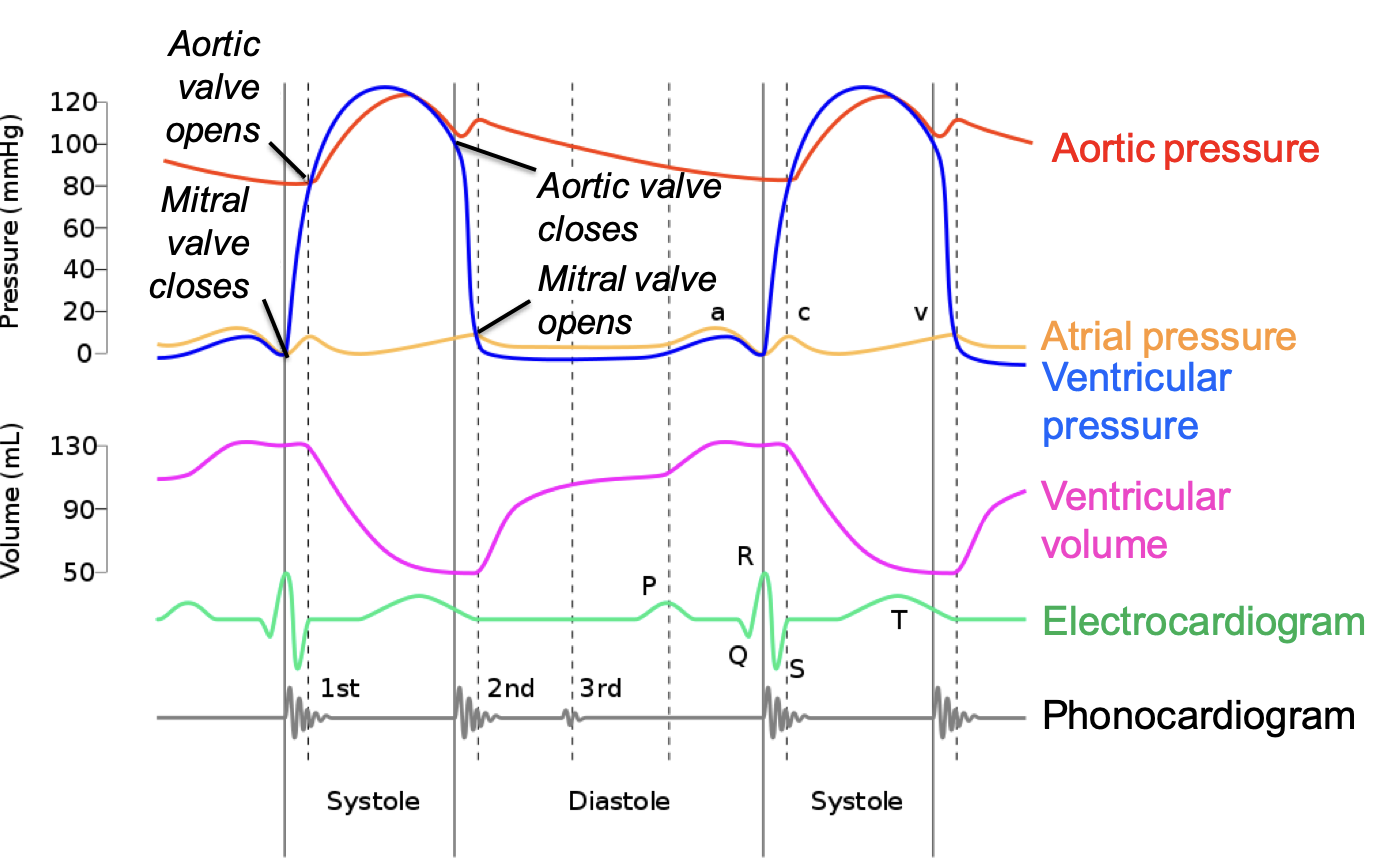
C. Vascular Physiology
- Overview of the vessels
- At the most basic level, there are 3 types of blood vessels
- Arteries
- Capillaries
- Veins
- Find the same layers in arteries and veins
- Tunica interna, tunica media, and tunica externa
- Variation in these layers
- For example, arteries differ based on their distance from the left ventricle
- Elastic artery: more elastic, close to heart
- Muscular artery: more muscle, farther from heart
- This is a way of controlling blood pressure
- At the most basic level, there are 3 types of blood vessels
- Vascular resistance to blood flow
- To also understand blood pressure, need to understand hemodynamics
- Hemodynamics: the flow of blood through tubes
- F=P/R
- F=flow rate (volume of blood that passes per unit time)
- P=pressure
- R=resistance
- To also understand blood pressure, need to understand hemodynamics
- Pressure gradient
- Difference in pressure between the beginning and end of a blood vessel
- Contraction of heart provides pressure: the pressure decreases as it flows through vessels due to resistance
- Difference in pressure between the beginning and end of a blood vessel
- Resistance
- Measure of hindrance to blood flow caused by friction between the moving fluid and the stationary walls
- Depends on:
- Viscosity
- Friction between molecules
- Tends to be relatively constant in blood
- Vessel length/radius
- Friction between blood and vessel
- Ex) resistance is 16x greater in a tube that’s half the diameter
- Viscosity
- Blood flow
- Because of the pressure, resistance, and total area of the tubes, the speed of blood flow varies in different parts of the circulatory system
- The pressure of the blood varies through the circulatory system too
D. Cardiac Output and Its Control
- Cardiac output
- Refers to the volume of blood pumped per minute by each ventricle
- Cardiac output (ml/min)=cardiac rate (beats/min) x stroke volume (ml/beat)
- Average resting cardiac rate=70 bpm
- Average stroke volume is 78-80 ml/beat
- Thus, the cardiac output is about 5.5 L per minute
- This is also equivalent to the total blood volume of the body
- Therefore, to regulate cardiac output, need to regulate the rate and/or the volume
- Heart rate: nerves and hormones
- Stroke volume: blood volume and vascular resistance
- Regulation of cardiac rate
- In absence of neural stimulation, heart will beat according to SA node
- However, if SA node was in complete control, the heart would always beat at the same rate
- HR is modified by the autonomic nervous system and endocrine system
- Things that increase heart rate:
- Sympathetic system: norepinephrine
- Adrenal glands: epinephrine
- Things that decrease heart rate:
- Parasympathetic system: acetylcholine
- Things that increase heart rate:
- Cardiac rate regulated by the ANS
- It is also regulated hormonally
- Regulation of stroke volume
- Regulated by 3 factors:
- Contractility: the strength of ventricular contraction
- End diastolic volume: the amount of blood in the ventricles just before they begin to contract (end of diastole)
- Afterload: or total peripheral resistance; the pressure ventricles need to work against
- Regulated by 3 factors:
- Contractility
- Any force that causes the ventricles to contract with more force will increase stroke volume
- This in turn increases cardiac output
- Nervous control:
- ANS control of stroke volume regulated almost entirely by sympathetic nervous system
- Epinephrine increase contraction strength
- Hormonal control:
- Ventricular contractility increased by a number of hormones
- Insulin, glucagon, thyroid hormones
- Any force that causes the ventricles to contract with more force will increase stroke volume
- End diastolic volume
- Force of ventricular contraction varies in response to stretching of ventricular wall
- Starling’s law: when the rate at which blood flows into the heart from the veins (venous return) changes, stretching of the ventricular wall changes, causing the ventricle to contract with greater or lesser strength so that the stroke volume (output) matches the venous return (input)
- So, if the amount of blood that returns increases, cardiac muscle will contract more to compensate
- Increased blood volume= increased stretch of myocardium= increased force to pump blood out
- Basically, starling’s law states that the more a heart fills, the stronger the force of contraction
- So, if the amount of blood that returns increases, cardiac muscle will contract more to compensate
- Afterload
- Both of the previously mentioned factors influence stroke volume by altering ventricular contraction
- Stroke volume also depends on amount of force opposing contraction
- Increased arterial pressure causes stroke volume to decrease
- The afterload is determined in the aorta after contraction starts
- Increased resistance = increased pressure = increased afterload = decreased stroke volume
E. Blood Pressure
- Blood pressure
- Regulated by blood volume, peripheral resistance, cardiac rate
- An increase in any one of these will increase blood pressure
- Blood volume can be regulated by kidneys
- Sympathetic system:
- Vasoconstriction: increases TPR
- Promotes cardiac output
- Both raise blood pressure
- Regulated by blood volume, peripheral resistance, cardiac rate
- Baroreceptors
- Detect changes in blood pressure
- Stretch receptors located in the aortic arch and the carotid sinuses
- Increase in pressure causes wall to stretch
- Signals travel through 2 cranial nerves to medulla oblongata
- Cardiac control centre
- Baroreceptors function to counteract pressure changes
- What do the kidneys do?
- Play a vital role in regulating blood volume
- Decrease in BP going into kidney -> cells of kidney release renin -> increase in angiotensin II
- How does angiotensin II promote a rise in blood pressure
- Increased resistance of blood vessels
- Acts directly on small arteries and arterioles
- Vasoconstriction
- Increased blood volume
- Thirst centers in hypothalamus stimulated
- Secretion of aldosterone from adrenal glands stimulated
- Causes more salt and water to be retained by kidneys
- This is known as the renin-angiotensin-aldosterone system
- Increased resistance of blood vessels
- Circulatory shock
- Inadequate blood flow and/or oxygen uptake by tissues
- Can result from low blood volume
- Vasoconstriction in various organs, including skin
- Results in low BP, rapid pulse, cold clammy skin
- Blood is diverted to heart and brain
- Septic shock
- Dangerously low blood pressure that results from sepsis (infection)
- High mortality (50-70%)
- Bacterial action activates immune system which promotes vasodilation
- Also, leakage from blood vessels
- Blood pressure drops
Topic 10: Blood Cells and the Lymphatic System
A. Blood Composition
- Composition of blood
- The blood consists of blood cells and platelets in a fluid matrix called plasma
- Blood cells
- RBCs carry oxygen to tissues
- WBCs have a number of functions, mainly defensive
- Platelets
- Cell fragments responsible for coagulation
- Plasma
- Mainly water
- Various wastes, nutrients, hormones, etc
- Red blood cells (erythrocytes)
- Optimized for gas transport
- Biconcave disk shape maximizes surface area
- Nucleus-free cytoplasm packed with hemoglobin
- Each Hb molecule can carry 4 molecules of oxygen
- Can also carry CO2 but <2%
- The life cycle of erythrocytes
- Production
- Remain in bloodstream for about 120 days
- New erythrocytes being produced at 2-3 million per second
- Erythropoietin released from kidney (and liver) in response to low O2
- Triggers erythrocyte production in bone marrow
- Needed: iron, folic acid, vitamin B12
- Destruction
- Spleen stores blood cells and removes old RBC from circulation
- Destroyed by macrophages
- Iron is removed from hemoglobin
- Hemoglobin converted to bilirubin
- Bilirubin released in blood
- Yellowish tinge
- Travels to liver; broken down further
- Products excreted in feces and urine
- Production
- Hematocrit
- Blood plasma can be separated into its main elements by centrifugation
- Hematocrit= the % by volume of red cells in your blood
- The sample shows the proportion of RBCs
- Generally around 45%
- Can vary from 35-55%
- Simple test that is done routinely
- Abnormal scores can mean many things
- White blood cells: leucocytes
- WBCs are divided into granulocytes and agranulocytes
- Granulocytes
- Neutrophils (most abundant WBC)
- Eosinophils
- Basophils (least abundant WBC)
- Agranulocytes
- Lymphocytes (most abundant agranulocyte)
- Monocytes
- Leucocytes differ from erythrocytes in several important features:
- Have nuclei and mitochondria
- Can move in amoeboid fashion
- Can squeeze through capillary walls to site of infection
- Therefore, leucocytes are found both in and out of the cardiovascular system
- Play an important role in the immune system
- Neutrophils
- Make up 50-80% of all WBCs
- Capable of phagocytosis
- Engulfs and digests microorganisms, abnormal cells, foreign particles
- Circulate in blood for 7-10 hours then migrate into tissues
- Live in tissues for a few days
- Levels increase during bacterial and viral infections
- Also, in response to inflammation and after surgery
- Eosinophils
- Make up 1-4% of all WBCs
- Also capable of phagocytosis
- Mainly attack parasitic invaders too large to be engulfed by neutrophils
- Attach to body of parasites and discharge toxic molecules from cytoplasmic granules
- Elevated levels often due to parasitic infections
- Can also be the result of a number of diseases (asthma, eczema)
- Basophils
- Make up <1% of all WBC
- Nonphagocytic cells
- Thought to defend against larger parasites
- Also release histamine and other chemicals that contribute to allergic reactions
- During acute allergic reactions, basophil levels in blood decrease
- Move to the site of the reaction
- Monocytes
- Make up 2-8% of all WBC
- Important phagocytes
- Tend to do most of their work outside the blood vessels
- In blood for a few hours before migrating into tissues
- Become 5-10x larger
- Develop into active phagocytic cells called macrophages
- Can undergo further differentiation in specific tissues
- Lymphocytes
- Make up 20-40% of all WBC
- Approximately 99% of these cells are found in interstitial fluid
- Extracellular fluid found outside the blood
- 3 major types: B-cells, T-cells, null cells (mainly natural killer cells)
- Complex functions in the immune system
- Platelets
- Thrombocytes
- Fragments of large cells called megakaryocytes
- Found in bone marrow
- Fragments that enter circulation lack nuclei but are capable of ameboid movement
- Live for 5-9 days
- Play important role in blood clotting
B. Blood Typing
- Antigens
- Certain molecules on surfaces of all cells
- Recognized as foreign by the immune system of another individual
- Lymphocytes secrete antibodies that bind with antigens
- Sets off a cascade of reactions that ultimately destroy the cell
- Red blood cell antigens are of extreme clinical importance
- Types must be matched between donors and recipients
- ABO system
- 2 antigens
- A and B
- This gives 4 blood types
- Blood type denotes the kind(s) of antigens present
- 2 antigens
- Transfusion reactions
- If blood types do not match between donor and recipient, recipient’s antibodies can attach to donor’s red blood cells
- Causes cells to lump together
- Can block small arteries
- Universal donor
- Type O
- Any recipient antibodies have nothing to attach to
- Universal recipient
- Type AB
- Recipient lacks antibodies for A and B antigens
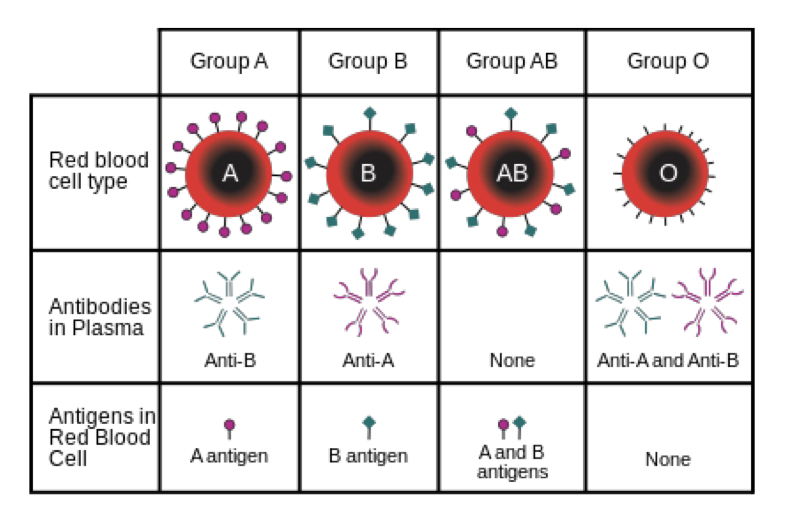
- If blood types do not match between donor and recipient, recipient’s antibodies can attach to donor’s red blood cells
- Rh factor (Rhesus)
- Another group of antigens found on RBCs
- Rh positive -> have the Rh antigen
- Rh negative -> don’t have the Rh antigen
- Of particular importance when Rh- mothers give birth to Rh+ babies
- Blood systems usually kept separate through pregnancy
- At time of birth, certain mixing may occur, mother starts producing antibodies
- May affect subsequent pregnancies because the maternal antibodies attack fetal RBCs
C. Blood clotting
- Blood clotting
- When a blood vessel is injured, get a number of physiological mechanisms to stop bleeding
- Vasoconstriction
- Formation of platelet plug
- Production of a web of fibrin proteins
- Hemostasis
- Blood-stopping
- When a blood vessel is injured, get a number of physiological mechanisms to stop bleeding
- Functions of platelets
- In the absence of vessel damage, platelets repelled from each other and vessel wall
- Prevents inappropriate clotting
- Damage to vessel wall exposes collagen
- Platelets stick to collagen
- Released molecules that attract other platelets
- Many platelets aggregate
- Form platelet plug
- Also contains RBC
- Aspirin prevents release of molecules
- Also contains RBC
- Platelet plug must be reinforced by strong fibers
- Formed from fibrin
- Fibrin is the final product of a number of clotting factors
- Formation of fibrin can be activated 2 ways:
- Intrinsic pathway: no additional extrinsic chemicals
- Extrinsic pathway: chemical released from damaged tissues
- In the absence of vessel damage, platelets repelled from each other and vessel wall
- Bleeding disorders
- May be the result of incomplete plug formation
- Due to deficiencies in one or more of the clotting factors
- Majority of bleeding disorders are inherited
- Also caused by low RBC count or certain medications
D. The lymphatic system
- Lymphoid tissue
- Composed of reticular connective tissue
- Macrophages attached to fibers
- Diffuse lymphoid tissue
- Found in nearly every organ
- Lymphoid nodules
- Solid, spherical bodies
- Lots of B-lymphocytes
- Smaller than a lymph node
- Composed of reticular connective tissue
- Nodes
- 100s of small organs located along lymphatic vessels
- Groups of nodes occur near the surface in certain regions:
- Cervical
- Axillary
- Inguinal
- Functions:
- Filter lymph before returning it to the bloodstream
- Activate immune system
- swollen lymph nodes
- If large numbers of bacteria trapped in node, they can become inflamed
- Causes swelling and tenderness
- Typically occurs in neck, armpit, or groin
- Lymph: consists of fat, water, proteins, salts, glucose and WBCs, does not normally contain RBCs
- Other lymphoid organs
- A number of other organs have aggregates of lymphoid tissue
- Spleen
- Similar in shape and structure to a lymph node but much larger
- Largest lymphoid organ
- Filters blood in much the same way that the lymph node filter lymph
- Also stores breakdown products of RBCs and re-circulates them to liver
- Thymus
- Examined with endocrine system
- Located just above heart
- Large in newborns and continues to increase in size
- Begins to decline after puberty
- Function declines as we get older
- Primary function: processing and maturation of T-lymphocytes
- Development of immune responses
- Mucosa-associated lymphoid tissue (MALT)
- Patches of lymphoid tissue located on mucous membranes throughout the body
- Strategically placed to protect us from pathogens entering the body
- Tonsils:
- Form a ring of lymphoid tissue around entrance to pharynx
- Remove many of the pathogens entering through the mouth or nose
- Peyer’s patches
- Patches of lymphoid tissue located in the small intestine
- Immunosurveillance
- Appendix
- Tubular offshoot at beginning of large intestine
- It, along with the Peyer’s patches, helps destroy bacteria in intestine
- Movement of lymph
- Lymphatic capillaries are blind ending tubes
- Located with blood capillaries
- Extremely permeable
- Endothelial cells fit together like flaps
- Open when fluid between cells increases
- Act like one-way swinging door
- Same mechanisms that propel blood along veins
- Lymph flows into larger vessels from the lymphatic capillaries
- Capillaries -> collecting vessels -> trunks -> ducts
- Lymphatics near skin travel along superficial veins
- Deep lymphatics travel along deep arteries
- More variable than blood vessels
- Lymph eventually transported to one of 2 large ducts in thoracic region
- Each of these ducts empties into the jugular vein where it means the subclavian vein
- Right lymphatic duct
- Thoracic duct
- Each of these ducts empties into the jugular vein where it means the subclavian vein
- Interactions of the lymphatic system with other systems
- Cardiovascular
- Returns fluid and proteins that have been filtered out of blood vessels
- Immune
- Acts as a filter to help capture and destroy foreign pathogens
- Digestive
- Picks up absorbed fat and transfers it into circulatory system
- Cardiovascular
- Relationship with the cardiovascular system
- Let’s talk about BP again
- Ventricular contraction generates a great deal of pressure (hydrostatic)
- Declines as we get to capillaries
- Still high enough to favor fluid flowing out of capillaries
- However, there is another kind of pressure (osmotic)
- Results from unequal concentration of proteins inside and outside the arteriole
- Favors fluid moving back into the circulatory system
- Results from unequal concentration of proteins inside and outside the arteriole
- As blood approaches the capillaries:
- Hydrostatic pressure > osmotic pressure
- Fluid is forced into tissues
- As blood leaves the capillaries:
- Osmotic pressure > hydrostatic pressure
- Almost all of the fluid is forced back into circulatory system
- But about 10% of the fluid that has leaked out of the circulatory system is not forced back in
- This is where the lymphatic system comes in…
- Any fluid that remains in tissues is picked up by lymphatic vessels
- One way flow of fluid
- Enters circulatory system at subclavian vein
- Blood filtered along the way
- Let’s talk about BP again
- Relationship with the immune system
- Forms a major part of our immune response, to the continual exposure to microorganisms
- Organisms must first get past:
- Physical barriers such as the skin
- Toxic barriers such as acidic contents of stomach
- If they get past these, must be dealt with by immune system
- Lymphatic system plays key role in immunity as lymph fluid is continually presented to immune system cells
- Relationship with digestive system
- Almost all fats absorbed by intestines are taken up by the lymphatic system
- Small intestine has specialized vessels of lymphatic system called lacteals
- Found in the absorptive layer of the intestine
- Lacteals absorb fats and fat-soluble vitamins
- Blood capillaries take up everything else
Topic 11: The Respiratory System
A. Introduction
- Respiration
- The process of gas exchange
- External respiration: exchange between atmosphere and body tissues
- Internal respiration (cellular respiration): use of oxygen to generate ATP in cells
- We will focus on external
- External respiration involves 4 processes
- Breathing
- Inspiration and expiration
- Exchange of gasses between lungs and blood
- Transportation of gasses between lungs and tissues
- Exchange of gasses between blood and tissues
- Breathing
- In addition to its main function, the respiratory system performs several other functions
- Contributes to acid-base balance in blood
- Enables vocalization
- Defense against pathogens and foreign particles
- Provides route for water and heat loss
- Enhances venous return
- Activates certain plasma proteins
B. Forces for Pulmonary Ventilation
- Pulmonary pressures
- 3 primary pressures are associated with ventilation:
- Atmospheric pressure
- Pressure in air around you
- Usually around 760 mmHg at sea level
- Can be affected by a number of things
- (Intra) alveolar pressure
- Air pressure in alveoli
- At rest it is the same as atmospheric pressure
- Varies during different stages of respiration
- It is the difference between atmospheric pressure and intra-alveolar pressure that drives respiration
- (Intra) pleural pressure
- Air pressure in pleural cavity
- Always slightly lower than intra-alveolar pressure
- The slight pressure difference between the pleural cavities and alveoli keep the lungs inflated
- Atmospheric pressure
- 3 primary pressures are associated with ventilation:
- It’s important that the pleural pressure is always lower than the alveolar pressure
- If something happens to equalize the pressure, the lung collapses
- The transpulmonary pressure is the difference between the intra-pleural pressure and the intra-alveolar pressure
- Transmural pressure: pressure differences on 2 sides of wall
- The lungs at rest
- Between breaths, all breathing muscles relaxed
- No movement of air into or out of lungs
- No pressure gradient to drive air movement
- Muscular movement needed to create pressure gradient
- Ie, atmospheric pressure = alveolar pressure
- Mechanics of breathing
- When we breathe, pressure relationships change
- Inspiration:
- Diaphragm contracts, moves inferiorly
- Volume of thoracic cavity increases
- Can be aided by external intercostal muscles
- Together, these can result in an increase in volume of the thoracic cavity of about 500 mL
- Increased volume of thoracic cavity -> lungs stretch -> alveolar pressure drops slightly -> air rushes into lungs
- Expiration:
- Relies more on the elasticity of the lungs
- Diaphragm relaxes, rib cage descends
- Can be aided by the internal intercostal muscles
- Other muscles used while breathing
- Inspiration
- During regular (quiet) breathing, increase in thoracic cavity volume results from diaphragm and external intercostal muscles
- Can be aided by sternocleidomastoid, scalenes, and pectoralis minor
- Expiration
- No muscles necessary during quiet breathing
- During active breathing can use internal intercostals, abdominals
- Inspiration
- Lung volumes and capacities
- Spirometers are used to assess lung functioning
- Maximum rate a person can exhale critical in diagnosing certain pulmonary diseases
- Enable measurement of 3 to 4 lung volumes that make up total lung capacity
- Lung capacities are the sums of 2 or more lung volumes
- Inspiratory reserve volume (IRV)
- Maximum amount of air that can be inspired from the end of a normal inspiration (~2000 mL)
- Tidal volume
- Single, unforced breath (~500 mL)
- Expiratory reserve volume (ERV)
- Maximum amount of air that can be expired from the end of a normal expiration (~1000 mL)
- Residual volume (RV)
- Left over air that can’t be expired (~1200 mL)
- Spirometers are used to assess lung functioning
C. Gas Exchange
- Gas exchange
- During external respiration, oxygen diffuses into the blood and CO2 diffuses out
- Passive process requiring no energy
- Relies on pressure relationships
- Internal vs external respiration
- External: oxygen flows into blood; carbon dioxide flows out
- Internal: oxygen flows out of blood; carbon dioxide flows in
- As blood vessel approaches alveolus:
- Partial pressure of O2 in alveolus > partial pressure of O2 in blood vessel
- O2 moves into blood
- The opposite occurs for CO2
- When partial pressures equalize, no further gas exchange
- Partial pressure of O2 in alveolus > partial pressure of O2 in blood vessel
- Gas exchange is aided by:
- Large surface area
- So many alveoli provide tremendous amount of area over which gas exchange occurs
- Very thin membrane
- Large surface area
D. Control of Respiration
- Control of respiration
- We need a reliable way of inflating and deflating the lungs
- It must be:
- Automatic: should not depend on levels of consciousness
- Adaptable: be able to compensate for changes in O2 or CO2
- Subject to voluntary control: need to override the control mechanisms at least for brief periods of time
- Neural control of breathing by motor neurons
- Inspiration requires contraction of inspiratory muscles; expiration is a passive process
- Because inspiratory muscles are skeletal, stimulated by somatic motor neurons
- Phrenic nerve -> diaphragm
- Intercostal nerves -> intercostal muscles
- Generation of breathing rhythm
- Breathing is under both voluntary and involuntary control
- Respiratory control regions are located in the pons and medulla
- These are usually referred to as inspiratory and expiratory centers
- Both regions have both types of centers
- Most regulation of quiet breathing takes place in medulla
- Peripheral input to respiratory centers
- Several types of sensory input can alter respiration
- Central and peripheral chemoreceptors
- Monitor chemical conditions in cerebrospinal fluid and arterial blood
- Primarily responsible for regulating breathing while at rest
- Pulmonary stretch receptors
- In smooth muscle of pulmonary airways
- Irritant receptors
- Stimulated by smoke, dust, cold
- Breathing very slowly (or not at all) alters the chemical composition of arterial blood
- Changes detected by chemoreceptors in major arteries and brain
- Peripheral sensors located in carotid and aortic bodies
- Central sensors located in medulla
- Hyperventilation
- Increase in rate and depth of breathing
- Exceeds body’s need to remove CO2
- Low CO2 results in cerebral blood vessel constriction
- This can lead to fainting
- Other controls of breathing
- Hypothalamus
- Can influence breathing rate during strong emotions or pain
- Ex) increased or decreased rates while angry or excited
- Cerebral cortex
- Can consciously control breathing rate and bypass medulla
- Ex) holding breath underwater
- Hypothalamus
- Respiratory adjustments
- During exercise
- Not dependent on levels of CO2 or O2
- Impulses from proprioceptors in joints and muscles excite respiratory centers
- At high altitude
- Short term
- Breathing rate increases
- Can also result in dizziness, nausea, headaches
- Long term
- Acclimatization
- Physiological changes in both respiratory and circulatory systems
- Higher levels of RBCs
- Short term
- During exercise
E. Respiratory Acid-Base Balance
- Acid-Base balance
- Nearly all biochemical reactions in the body are influenced by pH
- Therefore, acid-base balance has to be strictly regulated
- Arterial blood: pH=7.4
- Venous blood and IF: pH=7.35
- Intracellular fluid: pH=7.0
- Alkalosis: pH of arterial blood > 7.45
- Acidosis: pH of arterial blood < 7.35
- H+ concentration in blood is regulated by:
- Chemical buffers (within seconds)
- Respiratory rate (within minutes)
- Kidneys (hours/days)
- Respiratory pH imbalances
- Occurs when respiratory mechanisms to balance acid-base are not working properly
- Respiratory acidosis
- Not breathing hard enough to get rid of CO2
- Too little CO2 exhaled.. Can lead to passing out
- Blood becomes more acidic
- Often occurs with lung ailments
- Pneumonia, cystic fibrosis, emphysema
- Not breathing hard enough to get rid of CO2
- Respiratory alkalosis
- Breathing too hard
- Too much CO2 exhaled.. Can lead to passing out
- Hyperventilation
- Often due to stress or pain
- Breathing too hard
- Metabolic pH imbalances
- All acid-base imbalances, except those cause by too much/little CO2 in the blood
- Metabolic acidosis
- Low blood pH levels
- Can occur for a number of reasons:
- Consumption of too much alcohol
- Persistent diarrhea
- Kidney failure
- Starvation
- Metabolic alkalosis
- Much less common
- Vomiting (losing acid from stomach)
- Consuming too many antacids
- In general:
- Respiratory imbalances affect CO2
- Metabolic imbalances affect HCO3 (bicarbonate)
Topic 12: The Urinary System and Fluid Balance
A. The Urinary System
- Overview of system
- Organs include kidney, bladder
- Kidney structure
- Both the cortex and medulla contain nephrons
- Cortex: outer region and extends between pyramids
- Medulla: consists of renal pyramids
- Calyces: collecting area for urine
- Ureter: delivers waste to bladder
- The nephron
- Main functional unit of the kidney
- More than a million crowded into each kidney
- It is within these structures that blood is filtered
- Wall is one cell layer thick but differs histologically depending on location and function
- What the kidneys do
- They work hard
- 1200 mL of blood pass through glomeruli each minute
- 650 mL is plasma
- About 125 mL forced into Bowman’s capsule as filtrate
- This means that all the plasma in your body is filtered through the kidneys about 60 times each time
- 3 processes involved
- Glomerular filtration
- Pouring blood into a container
- Not very selective
- Everything in plasma but proteins
- Tubular reabsorption
- Reclaiming what the body needs
- Selectively move substances back into bloodstream
- Tubular secretion
- Selectively remove other things from blood
- Becomes part of the waste (urine)
- Glomerular filtration
- Glomerular filtration
- Plasma moving into Bowman’s capsule
- Simple mechanical filtration
- No energy required
- 3 layers regulate filtration:
- Capillaries are fenestrated
- Pores in the walls of the capillary allow everything but blood cells to pass through
- Basement membrane of capillary epithelium
- Physical barrier that blocks all but smallest proteins
- Specialized cells attach to the capillaries for added filtration
- Podocytes have armlike extensions that cover the capillary
- Creates filtration slits
- Capillaries are fenestrated
- Tubular reabsorption
- Involves both active and passive transport
- Different substances reabsorbed in different parts of the tubule system
- Proximal convoluted tubule
- Most active region of reabsorption
- Nearly all the glucose and amino acids
- 65% of the sodium and water
- Also get reabsorption of uric acid and urea
- Later secreted back into filtrate
- Loop of Henle
- Water reabsorbed from descending limb but not ascending limb
- Just the opposite for solutes
- Ex) sodium, potassium, chloride
- Distal convoluted tubule
- Most water and solutes have been reabsorbed at this point
- Get fine tuning of what’s left
- Largely under hormonal control
- Example: antidiuretic hormone: vasopressin
- Acts on collecting duct and distal tubule
- Collecting duct is now permeable to water, causes concentrated urine
- Normally, collecting duct is impermeable to water, urine is dilute
- Tubular secretion
- Moves selected substances from peritubular capillaries into filtrate
- PCT is the main site of secretion
- Important for:
- Certain drugs and substances that bind closely to proteins
- Urea and uric acid
- Excess potassium (K)
- Controlling blood pH
- Renal clearance
- Rate at which certain substances are removed from the plasma by the kidneys
- Related to glomerular filtration rate (GFR)
- Tests for GFR:
- Look at possible kidney damage
- Follow progression of kidney disease
- Rate at which certain substances are removed from the plasma by the kidneys
- Chronic renal disease
- GFR < 60 ml/min for at least 3 months
- Nitrogenous wastes accumulate in blood
- Blood becomes more acidic
- Main causes:
- Diabetes
- Hypertension
- Renal failure
- GFR < 15 ml/min
- Results in uremia (urine in the blood)
B. Water Balance
- Water balance
- To keep the body hydrated, need to take in as much fluid as we get rid of
- Most fluid taken in with food and water
- Most fluid released in urine, through our skin, and through our lungs
- Water intake regulation: thirst
- [solute] in ECF increases -> osmoreceptors in hypothalamus -> sensation of thirst -> drink -> water absorbed from GI tract -> [solute] in ECF decreases
- Water output regulation
- Body is always losing water
- Cannot survive long without replacing it
- Minimum amount of water excreted in urine: 500 mL per day
- To get rid of waste from metabolism
- The amount excreted in addition to this depends on fluid intake and water loss by other means
- ex) perspiration, diarrhea
- Body is always losing water
- Antidiuretic hormone
- Increased levels of ADH = more water reabsorbed into the blood from collecting ducts of kidneys
- Seen when water content of the blood is low
- Urine becomes more concentrated
- Urine output is low
- Lower levels of ADH = urine becomes more dilute
- Too much alcohol causes less ADH
- Seen when water content of the blood is high
- Urine output is high
- Increased levels of ADH = more water reabsorbed into the blood from collecting ducts of kidneys
- Disorders of water balance
- Dehydration
- When water output exceeds water intake over a period of time
- Common causes: hemorrhage, burns, vomiting, diarrhea, sweating, water deprivation
- Possible effects:
- Short term: thirst, dry skin, decreased urine output
- Long term: weight loss, fever, mental confusion
- Hypotonic hydration (overhydration)
- Common causes: kidneys not working properly, drinking too much water
- Possible effects: nausea, vomiting, muscular cramping, damage to neurons, disorientation, convulsions, coma, death
- Edema
- Atypical accumulation of fluid in the interstitial space
- Leads to tissue swelling
- Common causes: increased pressure in capillaries, increased permeability in capillaries, blockage in lymphatic vessels
- Possible effects: decrease in blood volume and a drop in blood pressure
- Dehydration
- Edema can be organ specific
- Cerebral edema
- Extracellular fluid accumulation in the brain
- Causes drowsiness or loss of consciousness
- Pulmonary edema
- Pressure in blood vessels in the lung is raised because of obstruction to remove blood via the pulmonary veins
- Shortness of breath
- Cerebral edema
C. Electrolyte Balance
- Electrolyte balance
- Includes salts, acids, bases, and proteins
- Usually refers to salt balance
- Sodium, potassium, calcium are important electrolytes
- Most salts obtained with food and drink
- Tendency to take in more than needed
- Salt lost in perspiration, feces, urine, and vomit
- Sodium balance
- Regulating the balance between input and output of sodium one of the main kidney functions
- NaHCO3 + NaCl -> 90-95% of all solutes in the extracellular fluid
- Water follows salt, therefore, Na+ is the main molecule controlling osmotic pressure
- How is salt regulated in the body?
- Normally
- 65% of sodium reabsorbed in proximal tubules
- 25% reabsorbed in loops of Henle
- Aldosterone
- Hormone produced by adrenal cortex
- Regulates Na+ absorption and K+ secretion in kidneys
- Angiotensin II
- Activates release of aldosterone
- Also, a vasoconstrictor
- Low blood volume/pressure -> angiotensin II -> aldosterone -> Na+ reabsorption -> water reabsorption -> increased blood volume/pressure
- Normally
- Angiotensin receptor blockers (ARBs)
- Angiotensin can significantly increase blood pressure
- Good if BP is low
- Bad if BP is high
- ARBs are used for controlled high blood pressure
- Inhibit effects of angiotensin on both vasoconstriction and aldosterone release
- Remember: ACE inhibitors are angiotensin-converting enzyme inhibitors)
- Angiotensin can significantly increase blood pressure
- Influence of other hormones
- Estrogen
- Chemically similar to aldosterone
- Enhanced Na+ reabsorption by kidney tubules
- Leads to retention of water
- Largely responsible for edema during pregnancy
- Progesterone
- Partially blocks the effect of aldosterone
- Promotes sodium and water loss
- Estrogen
- Potassium balance
- Very important for neural and muscular functioning
- Slight changes in ECF can be life threatening
- Directly affects resting membrane potentials
- Particularly important for the heart
- Too much or too little can disrupt electrical conduction
- Sudden death
- Most of the regulation takes place in the collecting duct
- Normally people have enough potassium
- More K+ secreted from capillaries into collecting duct
- Also regulated by aldosterone
- If potassium low -> secretion inhibited
- Calcium balance
- Calcium and phosphate are important minerals of bones
- About 99% of the body’s calcium found here
- Outside of bones -> calcium affects:
- Normal clotting
- Cell membrane permeability
- Neuromuscular activity
- ECF levels of calcium are calcium are closely regulated by parathyroid hormone
- Calcium and phosphate are important minerals of bones
D. Renal Acid-Base Balance
- Remember what an acid is:
- Hydrogen (H+) containing substances that separate when in solution to free up H+ and negatively charged anions
- pH is inversely related to the concentration of H+ ions
- Therefore, the lower the pH, the more H+ ions, the more acidic the solution
- pH of arterial blood -> 7.45
- pH of venous blood -> 7.35
- Acidosis: blood pH < 7.35
- Alkalosis: blood pH > 7.45
- Acids continually being added to body fluids due to metabolic activities
- Must not be allowed to accumulate
- Have previously looked at control of blood pH by the respiratory system
- It is also controlled by the kidneys
- The kidneys control pH of body fluids by adjusting 3 factors: H+, HCO3-, NH3
- H+ excretion
- Almost all H+ enters the urine via secretion
- Free H+ in blood
- Enters proximal tubule through Bowman’s capsule
- Also secreted into tubule from peritubular capillaries
- Excreted in urine which tends to be quite acidic (pH~6.0)
- HCO3- excretion
- Plasma H+ buffered to a large degree by HCO3- (bicarbonate)
- HCO3- itself has to be regulated
- Also involves adjustment of amount of HCO3- excreted in urine
- Coupled with H+ secretion
- Ammonia (NH3) secretion
- H+ secreted into urine against concentration gradient
- Urine can become 800 x as acidic as plasma
- If left unbuffered as free H+, only about 1% of excess H+ produced daily could be secreted
- Ammonia (NH3) allows kidneys to keep secreting H+ ions
- NH3 + H+ -> NH4+ (ammonium)
- H+ secreted into urine against concentration gradient
Topic 13: The Immune System
- The immune system
- Protects the body against disease-causing organisms and nonliving substances that enter the body
- Immunity
- Ability to protect people by recognizing pathogenic agents
- Bacteria, bacterial toxins, viruses, parasites, fungi
- Ability to protect people by recognizing pathogenic agents
- Also disposes of aging cells and cellular debris
- Participates in wound healing
- Sometimes recognizes mutant cells that can become cancerous
A. Innate Defenses
- Innate defenses
- Defenses that are present at birth
- Ready to battle pathogens
- Pathogen: any harmful microorganism
- Bacteria, fungi, viruses, prions
- Consist of physical barriers, leukocytes, lymphoid tissues
- Surface barriers: skin and mucosae
- Body’s first line of defense
- Prevents entry of most microorganisms
- Nonspecific protection against foreign matter
- Has millions of organisms on it
- The hands are particularly rich in fauna
- Underneath nails -> palms -> backs of hands
- Microorganisms rarely penetrate epidermis
- Keratin resistant to most substances, including bacterial enzymes and toxins
- Especially associated with sweat glands and hair follicles
- Sebum and sweat may contain chemicals toxic to bacteria
- Typically cause no problems
- Some microorganisms can still penetrate intact skin, often through pores of sweat and oil glands
- Include some fungi, bacteria, worms
- Microorganisms much more likely to get into the body when skin is broken
- Bacteria and other pathogens enter wound
- Inflammatory response initiated
- Body’s first line of defense
- The skin
- The skin is an effective barrier, seen when diseases are a response to injury or penetration
- Some examples:
- Rabies virus
- Death almost certain if not treated
- Insect transmitted pathogens
- Ex) malaria, yellow fever, sleeping sickness, Lyme disease
- Rabies virus
- Vectors
- Vector= a carrier of a disease-causing agent
- Mosquito: malaria or yellow fever
- Tick: Lyme disease
- Tsetse fly: sleeping sickness
- Mucous membranes
- Mucous membranes line all the body cavities that open to the exterior
- Digestive, respiratory, reproductive, urinary tracts
- Act as a physical barrier (like skin)
- Also provide a wide variety of substances that combat microorganisms
- Acid
- Enzymes (ex: lysozyme)
- Mucous
- Defensins
- Mucous membranes line all the body cavities that open to the exterior
- Internal defenses: cells and chemicals
- Neutrophils: respond quickly to pathogens that get past the skin (50-80% of all WBCs)
- “Eat” bacteria
- Macrophages: monocytes that leave the bloodstream
- Very important in attacking and destroying pathogens
- Neutrophils: respond quickly to pathogens that get past the skin (50-80% of all WBCs)
- Phagocytosis steps
- 1) Ingesting pathogen
- 2) Enclosing pathogen in vesicle
- 3) Fusion with lysosome
- 4) Killing and breakdown of pathogen
- 5) Release of waste
- Natural killer cells
- Unique group of lymphocytes that can destroy pathogens before adaptive immune system is alerted
- The “pitbulls” of the immune system
- Generally referred to as NK cells
- NK cells attack in packs
- Release chemicals that perforate their victims
- Can even attack tumor cells
- NK cells act more quickly than other lymphocytes
- Respond within hours
- Usually respond to viral infections
- Also attack some tumor cells
- Recognize viral-infected cells
- Release perforins
- Proteins that form holes in membrane of infected cell
- Causes it to lyse
- Patients deficient in NK cells highly susceptible to early phases of herpes infection (and presumably other viral infections)
- Inflammation: friend or foe?
- Inflammation: response to tissue damage
- Heat, chemicals, infection
- Symptoms:
- Redness
- Heat
- Swelling pain
- Inflammation: response to tissue damage
- Functions of inflammation
- Prevent spread of damaging agents
- Disposes of cell debris and pathogens
- Alerts adaptive immune system
- Prepares tissue for repair
- Inflammatory response
- Mast cells release histamine
- Vasodilation
- Increased permeability of capillaries
- Delivery of cells and fluids to injured areas
- Phagocytes flood the damaged area
- First neutrophils, then macrophages
- Clear the area of any foreign material and dead tissue
- Mast cells release histamine
- Other signs of inflammation
- Pus is a sign of an inflammatory battle
- Dead and dying neutrophils
- Broken down tissue
- Living and dead pathogens
- In some cases, pus becomes walled off: abscess
- Pus is a sign of an inflammatory battle
- So, when is inflammation a problem?
- Inflammation is a normal and appropriate response involving your body’s defense system to infection and trauma
- Trouble occurs when that defense system runs out of control
- Get overactive immune response
- Can result in allergies, rheumatoid arthritis, autoimmune disease, asthma
B. Adaptive Defenses
- Adaptive defenses
- Protect us from a variety of infectious agents, as well as abnormal body cells (ex=cancer cells)
- Amplifies the inflammatory response
- Must “learn” to recognize specific pathogens
- Can then respond must more quickly
- Adaptive defense: main characteristics
- It’s specific: recognizes and attacks particular pathogens or substances
- It’s systemic: effects not restricted to the initial site of infection
- It has “memory”: after encountering a pathogen once, will recognize it the next time
- Antigens
- Substances that provoke an immune response
- Do not normally occur in the body
- Recognized as intruders
- Results in the production of antibodies
- anti(body)gen(erating)
- Have already observed an antigen-antibody response with respect to blood groups
- Many things can act as antigens
- Bacteria, fungi, viruses recognized as being foreign by molecules on their surfaces
- Large, foreign proteins
- Smaller molecules are usually not antigenic, but can combine with the body’s own proteins
- Incomplete antigens or haptens
- Ex) penicillin
- Incomplete antigens or haptens
- Bacteria, fungi, viruses recognized as being foreign by molecules on their surfaces
- Cells of the adaptive immune system
- 3 important types of cells:
- T lymphocytes
- Involved in cellular response
- Do not produce antibodies
- B lymphocytes
- Involved in humoral response
- Produce antibodies
- Antigen-presenting cells
- Helpers
- T lymphocytes
- 3 important types of cells:
- T lymphocytes (T cells)
- Helper T cells
- Main regulators of the immune system
- Primary task is to activate B cells and killer T cells
- Also need to be activated themselves
- Done by antigen-presenting cells
- Eats pathogen
- Presents information about that pathogen to helper T cell
- Activated helper T cells begin to divide and produce proteins that activate other immune cells
- Killer T cells
- Specialized in attacking cells of the body infected by viruses or bacteria
- Can also attack cancer cells
- Has receptors on surface used to recognize infected cells
- Infected cells have bits of antigens on their surfaces
- Helper T cells
- B lymphocytes (B cells)
- Searches for antigen matching its receptors
- If it encounters one, begins to divide and produces 2 different types of cells
- Plasma cell
- Produces antibodies that help destroy the specific intruder
- Release 10s of thousands of antibodies per second
- Memory cell
- Have prolonged lifespan and remember the specific intruder
- Will activate immune system much faster
- Plasma cell
- Antigen-presenting cells
- Engulf antigens and present fragments of them to T cells
- Dendritic cells
- Found close to the body surface
- Very good at catching antigens
- Enter lymphatic system and present antigen to T cell
- Macrophages
- Can also activate T cells
- Also need to be activated themselves
- Important phagocytes
- Dendritic cells
- Engulf antigens and present fragments of them to T cells
- Humoral immune response
- 1) The B-cell encounters an antigen that matches its receptors
- 2) It is then activated by a T helper cell
- 3) The B-cell divides to produce plasma and memory cells
- 4) Plasma cells produce antibodies that attach to the current invader
- 5) Macrophages prefer intruders with antibodies and begin to eat them
- 6) If the same intruder invades again, memory cells help to activate immune system more quickly
- Cellular immune response
- When antibodies presented to T cells
- Provoke a cellular immune response
- Some T cells directly kill infected cells, cancerous cells, cells from transplanted tissues
- Other T cells release chemicals that regulate the immune response
- Steps:
- 1) Cell infected by virus or bacteria
- 2) Antigen (parts of broken down pathogen) attach to MHC protein of cell
- 3) Antigen-MHC complex presented at surface of cell
- 4) Killer T cell (cytotoxic T cell) is activated by antigen-MHC complex
- 5) Activated T cells divide to form clones
- Receptors specific for this antigen-MHC complex
- 6) Upon binding, killer T cell releases chemicals that kill the target cell
- When antibodies presented to T cells
C. Some Problems
- Organ transplants
- Rejection by the immune system is a problem for tissue and organ transplants
- Success depends on similarity of tissues
- To minimize rejection:
- Same blood type
- Tissue matching (MHC antigens) as much as possible
- Immunosuppressant drugs
- Rejection by the immune system is a problem for tissue and organ transplants
- Immunosuppressant drugs
- Corticosteroids
- To suppress inflammation (in this case, inflammation is bad!)
- Antidepressants and antiproliferatives: kill rapidly dividing cells such as lymphocytes
- Problem: immune system now much less effective against other pathogens
- Requires other drugs (such as antibiotics)
- Corticosteroids
- Immunodeficiencies
- Any condition that impairs the production or function of immune cells or antibodies
- Ex) Hodgkin’s lymphoma: cancer of the B cells
- Ex) Acquired immunodeficiency syndrome (AIDS): cripples the immune system by interfering with the activity of helper T cells
- Autoimmune diseases
- Immune system loses ability to distinguish between “self” and “non-self”
- Begins to attack own tissues
- Examples:
- Rheumatoid arthritis: joints
- Multiple sclerosis: myelin
- Type I diabetes: pancreatic cells
- Lupus: various cells and tissues
- Immune system loses ability to distinguish between “self” and “non-self”
- Hypersensitivities
- When immune system attacks something that is relatively harmless
- Can be fast acting
- Allergies
- When particularly serious can result in anaphylactic shock
- Treat with epinephrine to reverse effects of histamine
- Can also act more slowly
- Ex) contact dermatitis (some plants - poison ivy, some metals, some cosmetics)
Topic 14: The Digestive System
A. Diet and Nutrition
- Diet and nutrition
- Nutrients are needed for growth, maintenance, and repair
- Major nutrients: carbohydrates, lipids, proteins (and water)
- Minor nutrients: vitamins, minerals
- Essential nutrients: approximately 50 molecules that the body must obtain through food
- Carbohydrates
- Almost all come from plants
- Except lactose
- Monosaccharides: fructose and galactose go to the liver, released as glucose, used as ATP
- While most of the mono- (and di-) saccharides come from fruit and sugar, polysaccharides come from fruit, vegetables, and grains
- Complex carbohydrates
- Starch (digestible) and fiber (nondigestible)
- Starch takes longer to be digested than simple sugars
- Still ultimately broken down and absorbed as glucose
- Almost all come from plants
- Some of the complex carbohydrates is fiber
- The part of food that is not affected by the digestive process in the body
- Fiber can be soluble or insoluble
- Fiber
- Insoluble: cellulose
- Good for colon health
- Eases and prevents constipation
- Soluble: retains water and turns to gel
- Stay fuller longer
- Lowers blood cholesterol
- Improves blood sugar
- Many important benefits
- Assist in moving food through the intestine
- Decreases cholesterol levels in blood
- Slow food absorption
- Increases “healthy” gut bacteria
- Insoluble: cellulose
- Cholesterol
- Waxy, fat-like substance found naturally in your body
- Body needs some cholesterol to work properly
- Too much can be a problem: atherosclerosis
- Required for:
- Making certain hormones
- Vitamin D production
- Making substances that help you digest food
- Our body can manufacture all the cholesterol we need
- Problem: it is contained in a lot of food as well (esp. Convenience foods)
- Cholesterol travels through the bloodstream in packages called lipoproteins
- Lipoproteins
- Made of fat on the inside and proteins on the outside
- There are 2 kinds:
- Low density (LDL)
- High density (HDL)
- Healthy levels of both is important
- LDL vs HDL
- LDL: bad cholesterol
- Stores cholesterol in the bloodstream
- HDL: good cholesterol
- Regulates LDL storage and promotes excretion
- Think of LDL as someone who drops stuff all over the house and HDL as the person who picks it up!
- LDL + HDL = total cholesterol
- High levels often said to be bad, but really want to minimize LDL
- LDL: bad cholesterol
- Lipids
- Fats have the same amount of calories but some are better than others
- Saturated fats
- Animal products, dairy, eggs
- Also, coconut and palm oils
- Solid at room temperature
- Raise “bad” cholesterol levels
- Unsaturated fats
- Should make up about 85% of your dietary fat
- Monounsaturated fats:
- Liquid at room temperature
- Begin to solidify at colder temperatures
- Increase “good” cholesterol
- Polyunsaturated fats
- Also liquid at room temperature
- Can reduce bad cholesterol
- Can also reduce good cholesterol
- Trans fats or hydrogenated fats
- These are also saturated fats
- Raise the “bad” cholesterol and lower the “good”
- Used mainly to extend the shelf life of baked goods
- Omega-3 fatty acids
- Include an essential fatty acid
- May reduce risk of heart disease and boost immune systems
- Fats
- Although fats have gotten a bad reputation, they are needed in the diet
- Should get about 25% of our calories from fat
- Why do we need them?
- Help absorb fat-soluble vitamins
- Major fuel source for some cells
- Myelin sheaths and cell membranes
- Although fats have gotten a bad reputation, they are needed in the diet
- Proteins
- Need a combination of proteins that provide all the amino acids
- Amino acids are used to build new proteins or can be used as an energy source
- Complete proteins
- Eggs, milk, fish, most meat
- Have all the amino acids required by the body
- High in protein
- Legumes (beans and peas), nuts, cereals
- Low in one or more of the essential amino acids
- Protein functions
- Digestive enzymes help facilitate chemical reactions
- Support muscle contraction and movement
- Antibodies support immune function
- Provide support to the body
- Hormones help coordinate bodily functions
- Support the regulation and expression of DNA and RNA
- Move essential molecules around the body
- Vitamins
- Required in small amounts for good health
- Not used for energy or as building blocks
- Most act as coenzymes
- Enzyme “helpers”
- Ex) glucose —vitamin B→ATP
- Vitamins are present in almost all foods
- But no one food contains all the necessary vitamins
- Water soluble
- B complex and vitamin C
- Absorbed along with water
- Any not used are excreted quickly
- Fat soluble
- Vitamins A, D, E, K
- Binds to lipids during absorption
- Most can be stored in the body
- Minerals
- Mainly calcium, phosphorus, potassium, sulfur, sodium, chlorine, magnesium
- Wide variety of functions
- Examples:
- Calcium and phosphorus: bones and cartilage
- Iron: hemoglobin
- Iodine: thyroid hormone
B. Digestion and Absorption
- Digestion
- Humans: digestive system is about 9m long
- Normally takes 24-72 hrs for digestive process to be completed
- Digestion refers to the breakdown of food into components that can be absorbed into the bloodstream
- Mechanical and chemical
- Humans: digestive system is about 9m long
- Mechanical digestion
- Generally, happens before chemical digestion
- Most mechanical digestion takes place in the mouth
- Teeth and tongue
- Creates a bolus of food that digestive enzymes can work on
- Further mechanical digestion takes place due to the muscular contractions of the stomach
- Chemical digestion
- Although mechanical digestion changes the appearance of the food, chemical digestion breaks down food into simple molecules that can be absorbed
- Enzymatic breakdown involves hydrolysis
- Adding water to a molecular bond to break it
- Monomer is a small molecule: sugars, amino acids, fatty acids, nucleotides
- Digestion of carbohydrates
- Monosaccharides: glucose, fructose, galactose
- Can be absorbed directly into bloodstream
- Disaccharides: sucrose (table sugar), lactose (milk sugar), maltose (grain sugar)
- Need to be broken down (digested) into simple sugars
- Polysaccharides: glycogen, starch
- Need to be broken down (digested) into simple sugars
- Average diet: about 60% of carbohydrates consumed as starch
- Note: we consume other nondigestible carbohydrates (cellulose) that provide fiber to diet
- Starch digestion begins in the mouth
- Salivary amylase converts starch into oligosaccharides
- Salivary amylase continues to work until food reaches stomach
- Inactivated by acid and protein-digesting enzymes
- Carbohydrate digestion finished in small intestine
- Pancreatic amylase converts carbohydrates into mostly maltose
- Enzymes that are found in the brush border of intestinal lining complete the digestion into monosaccharides
- Monosaccharides: glucose, fructose, galactose
- Digestion of proteins
- Dietary proteins, enzyme proteins from various glands, and proteins from cell breakdown are broken down in the digestive tract
- Protein digestion begins in the stomach
- Pepsin only active in acidic conditions
- About 15% of protein digestion takes place here
- Protein digestion ends in the small intestine
- Proteases released by pancreas break down proteins into smaller peptide chains
- Enzymes located in brush border break chains into amino acids
- Amino acids enter blood
- Digestion of lipids
- Lipids usually consumed in the form of triglycerides
- Insoluble in water (form fat globules)
- Need to be broken up (emulsified) so lipases can act on them
- Fat digestion begins in the mouth
- Lingual lipases:
- 10% of fat digestion
- Negligible amount
- Emulsification only
- Most important in newborns to help break down milk fat
- Lingual lipases:
- Continues in the stomach
- Gastric lipase:
- Begins fat breakdown in absence of bile
- Again, probably most important in newborns
- Estimated that 50% of fat broken down by lingual and gastric lipases (in infants)
- Gastric lipase:
- And ends in the small intestine
- In adults, triglycerides are for the most part unchanged until they reach the small intestine
- Pancreatic lipase:
- Breaks fat down to fatty acids and monoglycerides
- Absorption
- Nearly all the absorption of nutrients takes place in the small intestine, particularly in the jejunum
- Leaving the small intestine is only indigestible material, water, and bacteria
- Some substances pass through cell membranes passively (lipid soluble) while others require active transport
- Ultimately enter blood capillary or lacteal in villi of small intestine
- Water absorbed in large intestine
- Absorption of carbohydrates
- Active transport to get into intestine
- Facilitated diffusion to get into bloodstream
- Absorption of proteins
- Active transport to get into intestine
- Facilitated diffusion to get into bloodstream
- Absorption of lipids
- Slightly different as lipids are absorbed into lacteals instead of capillaries
- Bile salts emulsify lipids into droplets/micelles
- Chylomicrons in epithelial cell layer get released into lacteal via secretory vesicles
- Absorption of vitamins
- Depends on whether they are fat soluble of water soluble
- Fat soluble
- A, D, E, K
- Attach to dietary fats to cross epithelia of intestine
- Water soluble
- B, C
- Absorbed by active or passive transport
- Fat soluble
- Depends on whether they are fat soluble of water soluble
- Absorption of water
- Most water reabsorption occurs before the large intestine
- Moves in and out by osmosis
- More moves out
C. Neural and Hormonal Regulation of the Digestive System
- Regulation of digestive system
- Activities of different regions regulated by the vagus nerve and various hormones
- Neural
- Sight, smell, or taste of food activates vagus nerve
- Stimulates salivary and gastric secretions
- Conditioned reflex
- Hormonal
- GI tract both an endocrine gland and a target for various hormones
- Produces at least 6 hormones
- Regulation of gastric function
- Much of the control of movement and secretion are automatic
- Waves of contraction generated along the GI tract
- Secretion of acids and enzymes in stomach stimulated by presence of proteins
- Effects of autonomic nerves and hormones superimposed on this automatic activity
- Extrinsic control of gastric function can be separated into 3 phases
- Cephalic, gastric, intestinal
- Extrinsic control of gastric function can be separated into 3 phases
- Much of the control of movement and secretion are automatic
- Cephalic phase
- Controlled by brain via vagus nerve
- Activation of vagus nerve (by smell, taste, sight, etc)
- Chief cells secrete pepsinogen
- Parietal cells secrete HCl
- Also stimulates certain cells to produce gastrin (a hormone)
- Cephalic phase lasts about 30 mins at beginning of meal
- Gastric phase
- Stimulated by arrival of food in stomach
- Gastric secretion is dependent on:
- Distension of stomach (amount of chyme)
- Sends message back to brain via vagus nerve to increase activity
- Also works locally to increase secretion
- Chemical nature of chyme
- Polypeptides increase production of gastrin
- Stomach produces more pepsinogen and HCl
- Distension of stomach (amount of chyme)
- Intestinal phase
- Inhibition of gastric phase when chyme enters small intestine
- Due to neural reflex and hormone both originating in the duodenum
- Neural reflex due to stretch receptors sending signal back to CNS via vagus nerve
- Various hormones act to decrease movement and other gastric activity
- Inhibition of gastric phase when chyme enters small intestine
- Regulation of intestinal function
- The enteric nervous system (sometimes included with the autonomic nervous system) controls the activities of the intestine
- There are 2 plexuses in the wall of the intestine
- Contain about 100 million neurons
- About the same number as in the spinal cord
- Can operate independently of brain and spinal cord
- Regulation of pancreatic juice and bile secretion
- The arrival of chyme in the duodenum stimulates secretion of pancreatic juice and bile
- Low pH; fat and protein → secretion and cholecystokinin → pancreatic juice; gall bladder contracts and ejects bile
- Nutrient signals related to energy stores
- Rising blood levels of glucose, lipids, and amino acids: suppress hunger
- Gut hormones released during food absorption: suppress hunger
- Glucagon, epinephrine: stimulate hunger
- Ghrelin: stimulate hunger
Topic 15: The Endocrine System
A. Hormones
- Classification
- Chemically, there are 2 kinds of hormones:
- Amino acid based
- Size highly variable
- Amino acid → peptides → proteins
- Size highly variable
- Steroids
- Synthesized from cholesterol
- Manufactured in gonads or adrenal gland
- Amino acid based
- Chemically, there are 2 kinds of hormones:
- Protein structure
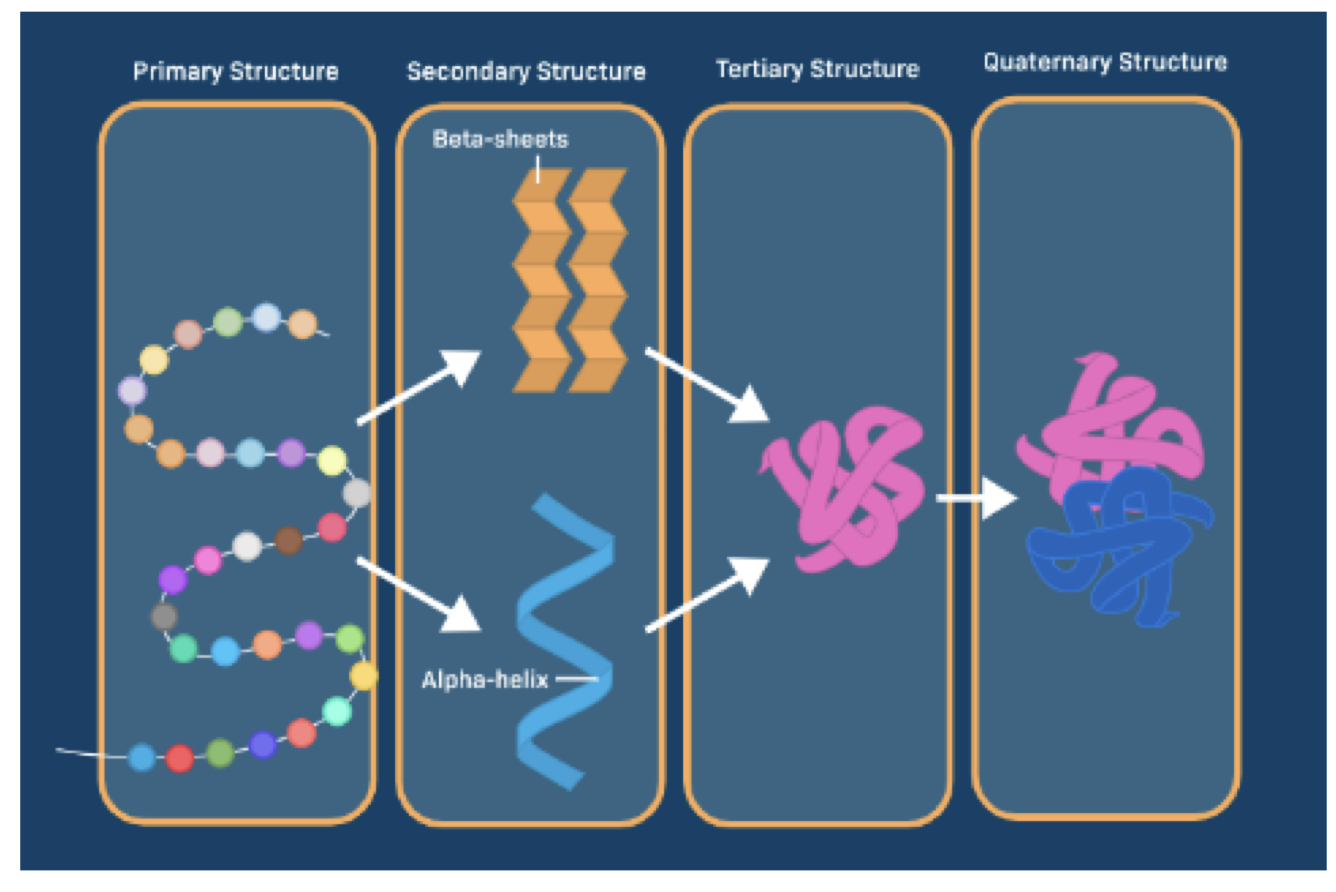
- Mechanisms of action
- Hormones are released into the bloodstream and are delivered to all tissues
- Come in contact with many different tissues
- However, only certain tissues respond
- Target tissues → cells with receptors for that hormone → activity change
- Steroid and peptide hormones enter cells differently
- Steroid hormones are lipid soluble
- Pass directly through the cell membrane
- Peptide hormones are water soluble
- Must first bind to receptors on cell membrane
- Steroid hormones are lipid soluble
- Steroid hormone
- Passes straight through the plasma membrane
- Binds to receptor protein in cytoplasm
- Enters nucleus and directly affects the expression of genes
- Amino acid based (peptide) hormone
- Hormone binds to receptor on cell membrane
- Receptor initiates a series of changes in the cell
- Ultimately enters nucleus and affects gene expression
- Or, affects cellular processes directly
- Control of hormone release
- Remember negative feedback loops
- External/internal stimulus → hormone secretion → effect on target tissues – inhibition of further hormone release
- 3 types of stimuli that initiate hormone release
- Humoral stimuli
- Changing blood levels of certain ions or nutrients
- Simplest type of endocrine control
- Example: control of blood calcium levels
- Neural stimuli
- Nerve fibers stimulate hormone release
- Example: response to stress
- Stimulus: action potentials from ANS stimulate adrenal gland
- Response: release of epinephrine and norepinephrine
- Hormone stimuli
- Release of hormones in response to other hormones
- Example: hypothalamus → pituitary gland → target endocrine gland
- Humoral stimuli
B. The Pituitary Gland and Hypothalamus
- Pituitary gland
- It is actually 2 glands in one
- Anterior pituitary
- Secretes hormones that control other endocrine glands
- Secretion regulated by hypothalamus
- Posterior pituitary
- Stores and secretes 2 hormones
- Hormones produced in hypothalamus
- Some terminology
- Pituitary gland: hypophysis
- Anterior lobe: adenohypophysis
- Pars distalis
- Pars tuberalis
- Posterior lobe: neurohypophysis
- Pars nervosa
- Pituitary hormones
- Anterior pituitary (pars distalis)
- These all end with the suffix “tropin” (attracted to)
- 1) Growth hormone (GH) or somatotropin
- Stimulates protein synthesis
- Promotes tissue and organ growth
- 2) Thyroid-stimulating hormone (TSH) or thyrotropin
- Stimulates thyroid gland to produce and secrete thyroxine
- 3) Adrenocorticotropic hormone (ACTH) or corticotropin
- Stimulates adrenal cortex to secrete glucocorticoids
- 4) Follicle-stimulating hormone (FSH) or folliculotropin
- Stimulates growth of ovarian follicles (females)
- Stimulates production of sperm (males)
- 5) Luteinizing hormone (LH) or luteotropin
- Stimulates ovulation (females)
- Stimulates testosterone production in testes (males
- 6) Prolactin (PRL)
- Stimulation of milk production (females)
- Acts on kidneys to help regulate fluid balance
- Anterior pituitary (pars distalis)
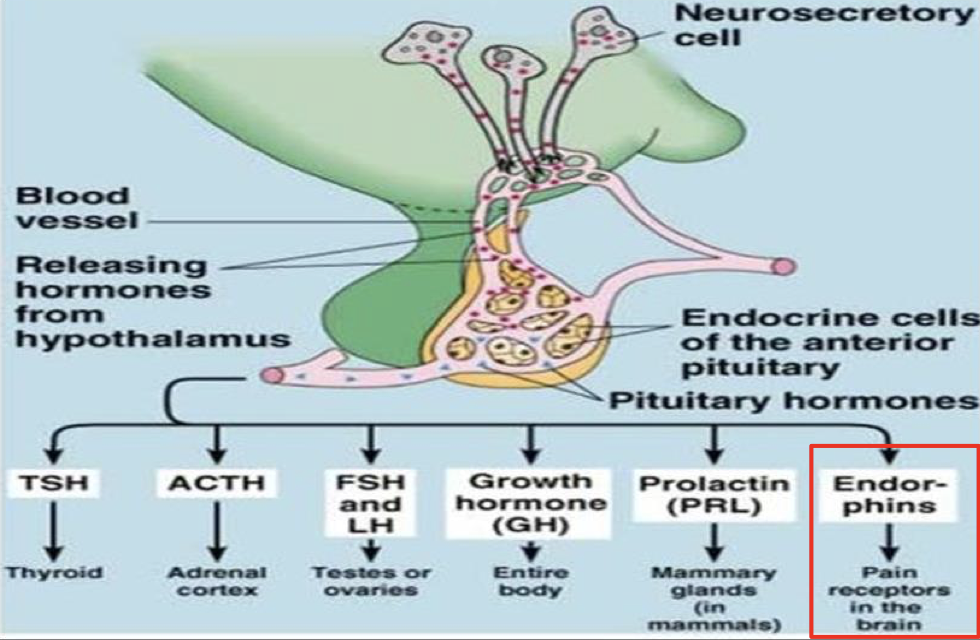
- Posterior pituitary
- 1) Oxytocin
- Acts as neurotransmitter in brain
- The “love hormone”
- Important for milk release during breastfeeding
- Stimulates uterine contraction during childbirth
- Acts as neurotransmitter in brain
- 2) Antidiuretic hormone (ADH)
- Inhibits or prevents urine formation
- Helps body avoid dehydration
- Targets kidney tubules
- 1) Oxytocin
- Posterior pituitary
- Hypothalamic control of the pituitary
- The secretion of hormones by the anterior pituitary is regulated by hormones of the hypothalamus
- These are generally called “releasing hormones”
- Many of these are involved in feedback loops
- Oxytocin and ADH are both produced in the hypothalamus
- Hypothalamus, pituitary hormones → target organs
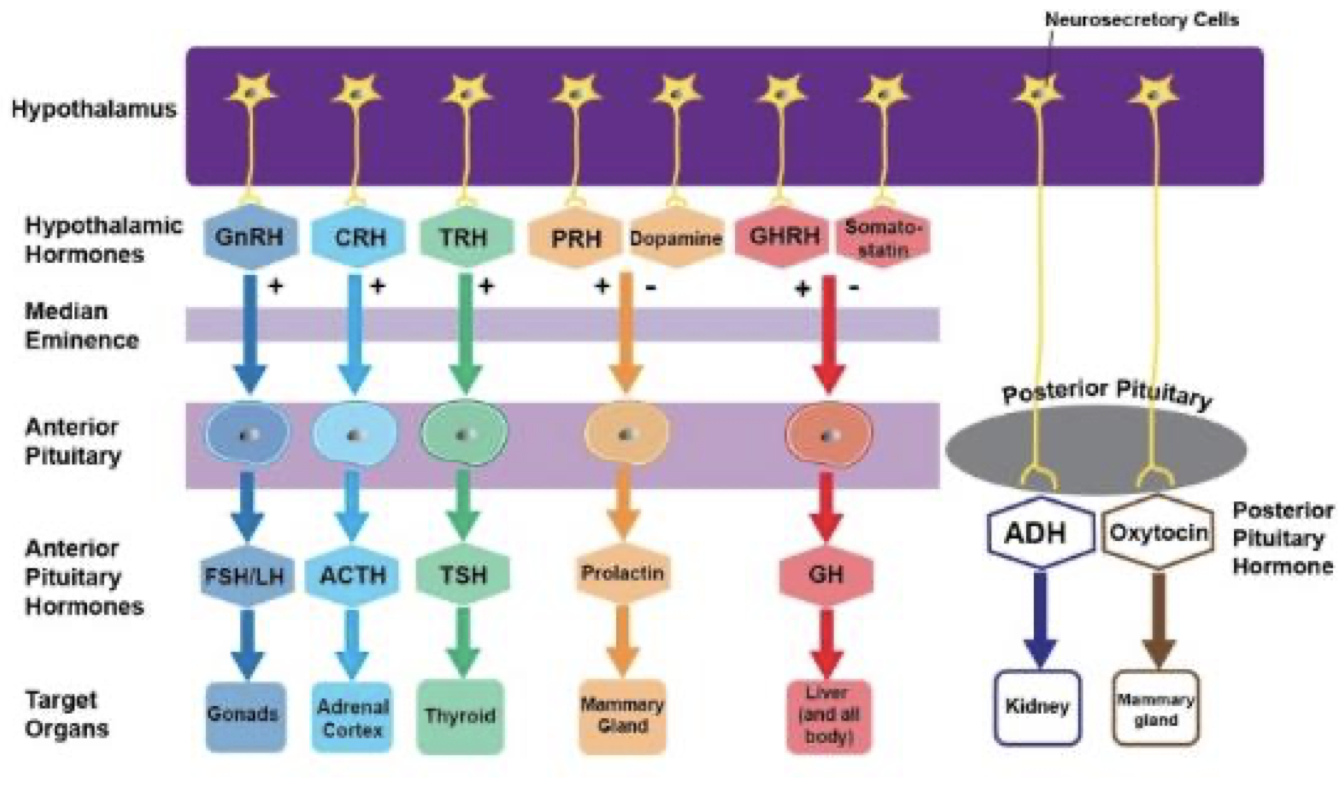
- Examples of feedback loops
- Hypothalamic-pituitary-thyroid axis
- TRH stimulates release of TSH → TSH stimulates production of thyroid hormone → thyroid hormone regulates metabolism → thyroid hormone provides feedback to the brain (pituitary and hypothalamus)
- Hypothalamus-pituitary-gonad axis
- Estradiol is involved in a positive feedback during the menstrual cycle - results in surge of LH that results in ovulation
- Hypothalamic-pituitary-thyroid axis
C. Adrenal Glands
- Parts of the adrenal glands
- Adrenal medulla:
- Inner region
- Hormones involved in “fight or flight” response
- Adrenal cortex:
- Outer region
- Secretes steroid hormones → mineral and energy balance
- Adrenal medulla:
- Adrenal medulla
- Secretes epinephrine and norepinephrine in a ratio of 4:1
- Effects similar to those caused by stimulating ANS, although last much longer
- Increase cardiac output and heart rate
- Dilate coronary blood vessels
- Increase mental alertness
- Increase respiratory rate
- Elevate metabolic rate
- Effects similar to those caused by stimulating ANS, although last much longer
- Secretes epinephrine and norepinephrine in a ratio of 4:1
- Adrenal cortex
- Secretes steroid hormones called corticosteroids
- 1) Mineralocorticoids
- Regulates concentration of sodium and potassium in extracellular fluids
- Important for functioning of muscular and nervous systems
- Most important one is aldosterone
- Accounts for >95% of mineralocorticoids produced
- 2) Glucocorticoids
- Help keep blood glucose relatively constant between meals
- Important stress hormones
- Most important in humans is cortisol
- Release follows predictable patterns through the day
- 1) Mineralocorticoids
- Secretes steroid hormones called corticosteroids
Highest in morning after breakfast
Lowest at bedtime
- Can increase dramatically when stressed
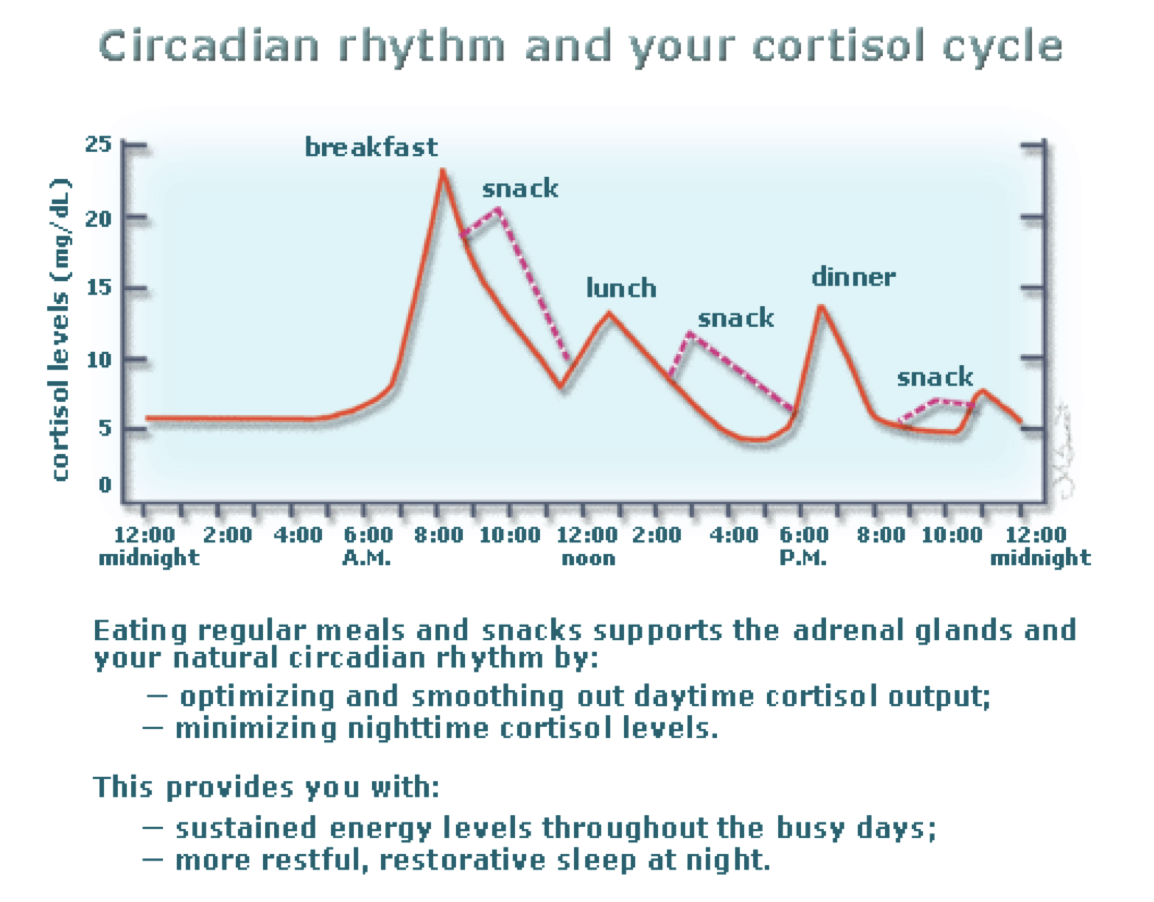
- 3) Gonadocorticoids
- Adrenal sex hormones
- Mainly androgens (weak male hormones)
- Function not entirely clear
- Contribute to axillary and pubic hair growth
- Thought to contribute to sex drive in women
- Produce estrogens after menopause
- Adrenal sex hormones
- 3) Gonadocorticoids
D. Thyroid and Parathyroid Glands
- Thyroid and Parathyroid
- Found just inferior to the larynx
- The largest purely endocrine gland in the body
- Thyroid secretes T4 and T3 which are needed for proper growth and development
- Parathyroid helps raise blood calcium concentration
- Hormones of the thyroid gland
- 1) Thyroid hormone
- Affects almost all cells of the body
- Increases metabolic rate and heat production
- Helps regulate growth and development
- Helps regulate blood pressure
- Release of thyroid hormone controlled by hypothalamus/pituitary
- 2) Calcitonin
- Works in concert with parathyroid hormone (opposite effects)
- Inhibits breakdown of bone tissue
- Stimulates excretion of calcium by kidneys
- Both actions result in lowering of calcium in blood
- Artificial supplements can be used to treat osteoporosis
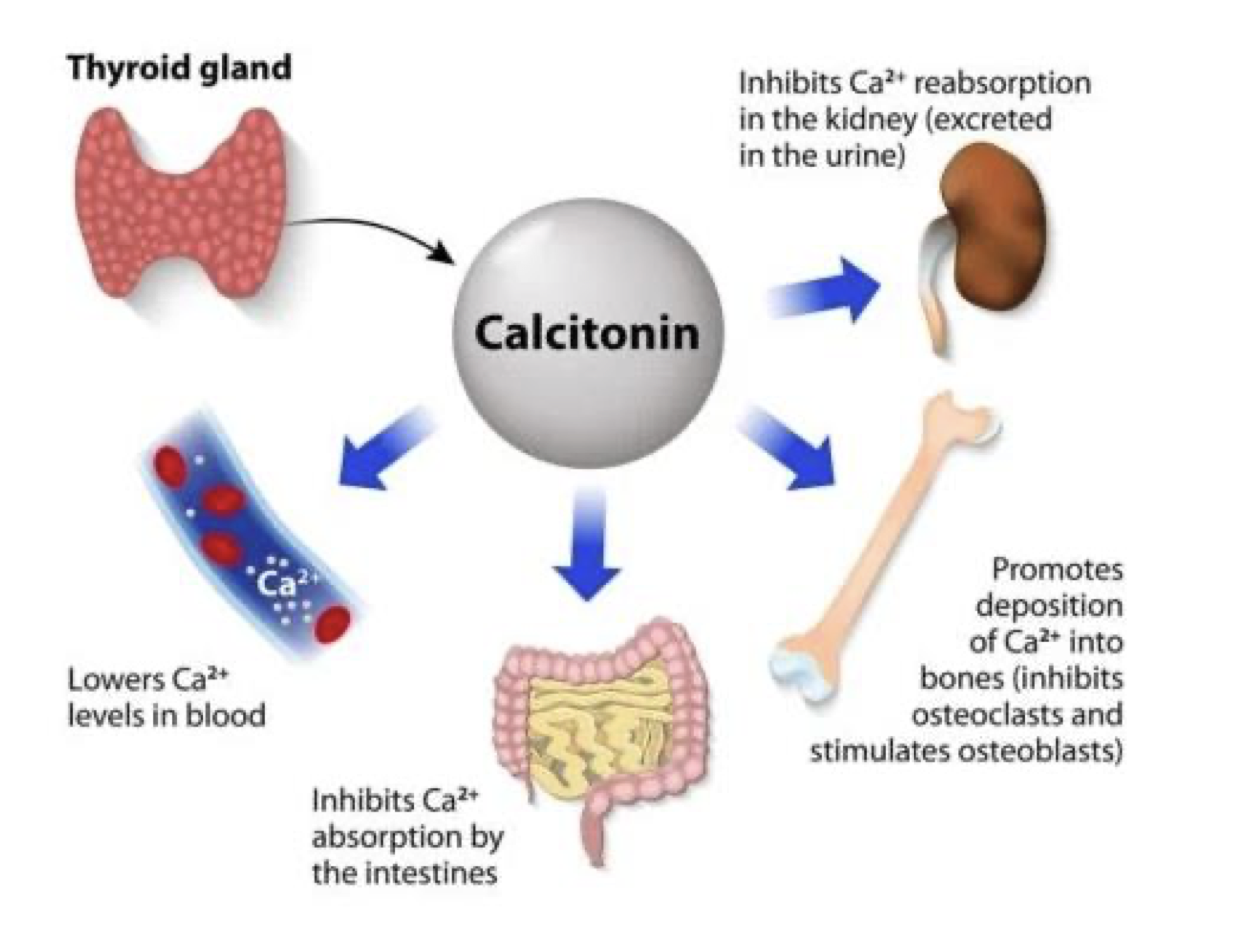
- Artificial supplements can be used to treat osteoporosis
- 1) Thyroid hormone
- Hormone of the parathyroid gland
- Parathyroid hormone
- Raises blood calcium levels
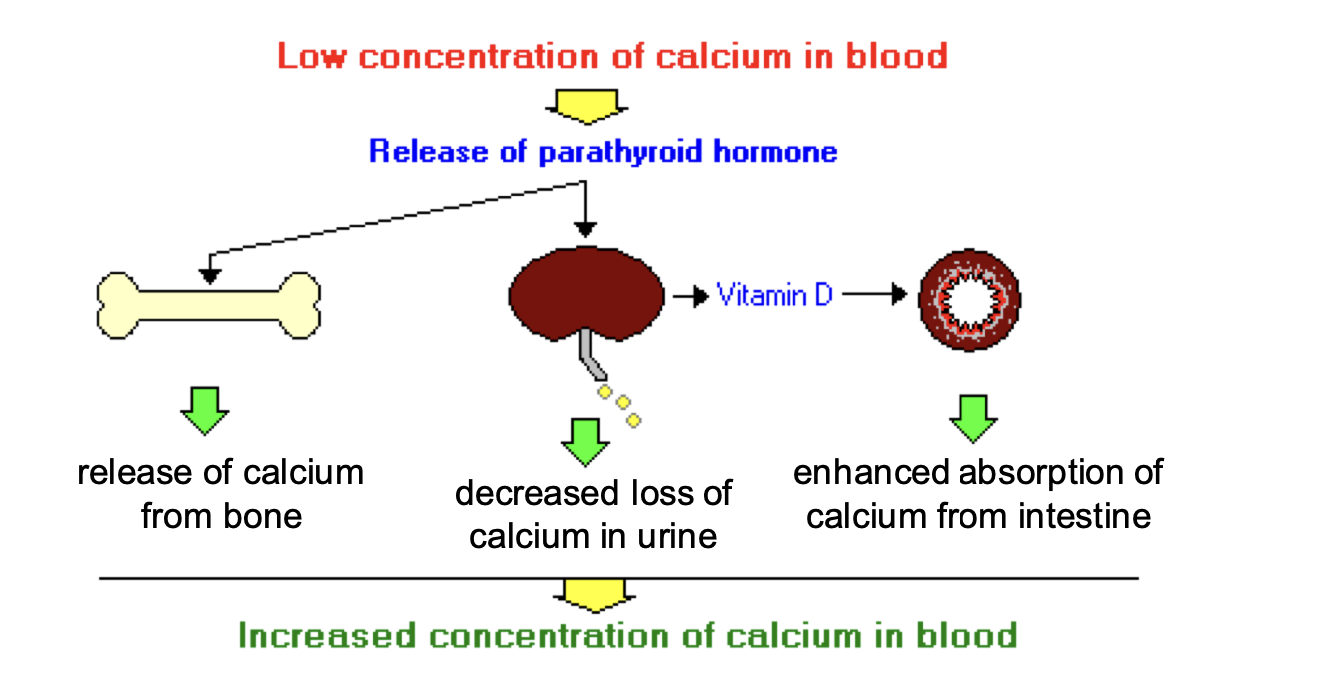
- Raises blood calcium levels
- Parathyroid hormone
- Calcium homeostasis
- Low calcium levels stimulates PTH secretion
- PTH stimulates osteoclast (breaking down the bone matrix)
- High calcium levels stimulates calcitonin secretion
- Calcitonin stimulates active osteoblast (increasing the bone matrix)
- Low calcium levels stimulates PTH secretion
E. Pancreas
- The pancreas
- Located in the first loop of the small intestine
- Secrete digestive enzymes to help break down food
- This is NOT the endocrine function
- Pancreas is both an endocrine and exocrine gland
- The endocrine function of the pancreas is to control blood sugar
- 2 hormones are produced in regions of the pancreas called Islets of Langerhans
- These islets are scattered throughout
- Hormones of the pancreas
- 1) Glucagon
- Very good at increasing blood sugar levels
- One molecule can cause the release of 100 million molecules of glucose
- Acts on the liver to:
- Break down glycogen into glucose
- Synthesize glucose from other molecules
- Release glucose into blood
- 2) Insulin
- Main function is to lower blood glucose levels
- Accomplishes this by:
- Promoting uptake of glucose into most cells, particularly muscle and fat
- Inhibiting breakdown of glycogen into glucose
- Inhibiting conversion of amino acids and fats into glucose
- So, blood sugar levels are largely controlled by feedback loops involving glucagon and insulin
- 1) Glucagon
- Diabetes
- Results from problems associated with insulin
- Type I diabetes
- Pancreas does not produce insulin
- Only found in about 5% of diabetics
- Must take insulin injections
- Type 2 diabetes
- Pancreas does not produce enough insulin or body doesn’t properly use the insulin available
- Can usually be treated with exercise and diet
- Gestational diabetes
- Can develop during pregnancy
F. Other Endocrine Glands
- Pineal gland
- Attached to roof of 3rd ventricle
- Secretion peaks between the ages of 1 and 3 years
- By the end of puberty, declines by 75%
- Secretes melatonin which is involved in circadian and seasonal rhythms and sexual maturation
- Thymus
- Bilobed organ in front of the aorta
- Relatively large in newborns and children
- Decreases in size after puberty
- Responsible for T-cells (lymphocytes) involved in immune system
- Also secretes a number of hormones that stimulate T-cells
- Gonads and placenta
- Gonads are also both endocrine and exocrine
- Exocrine products: eggs, sperm
- Endocrine products: sex steroids
- Females: estradiol, progesterone
- Males: Testosterone
- Placenta is a temporary endocrine organ
- Secretes several steroid and peptide hormones
- Most important ar estrogen and progesterone
- Influence pregnancy
- Pregnancy detected by HCG as it rises quickly, and then declines into the 3rd trimester
- Progesterone and estrogen however increase in the 3rd trimester
- Gonads are also both endocrine and exocrine
- Gastrointestinal tract
- Stomach and small intestine secrete various hormones that act on GI tract, pancreas, gallbladder
- Examples:
- Gastrin: released by stomach, stimulates secretion of gastric acid
- Secretin: released by 1st part of small intestine, stimulates secretion of digestive enzymes by pancreas, stimulates release of bile from gallbladder
Topic 16: Reproductive Physiology
A. Reproductive Physiology
- Reproductive physiology
- The hypothalamus-pituitary unit is the central regulator of endocrine function
- Activity of the gonads largely controlled by hormones released by pituitary
- Luteinizing hormone (LH) and follicle stimulating hormone (FSH)
- These, in turn, control many activities in the male and female reproductive systems
- Including the production of estrogen, progesterone, and testosterone
- Activity of the gonads largely controlled by hormones released by pituitary
- The hypothalamus-pituitary unit is the central regulator of endocrine function
- The hypothalamic-pituitary-gonadal axis
- The male and female hormones will then affect the amounts of hormones released by the brain
- Good example of a negative feedback loop!
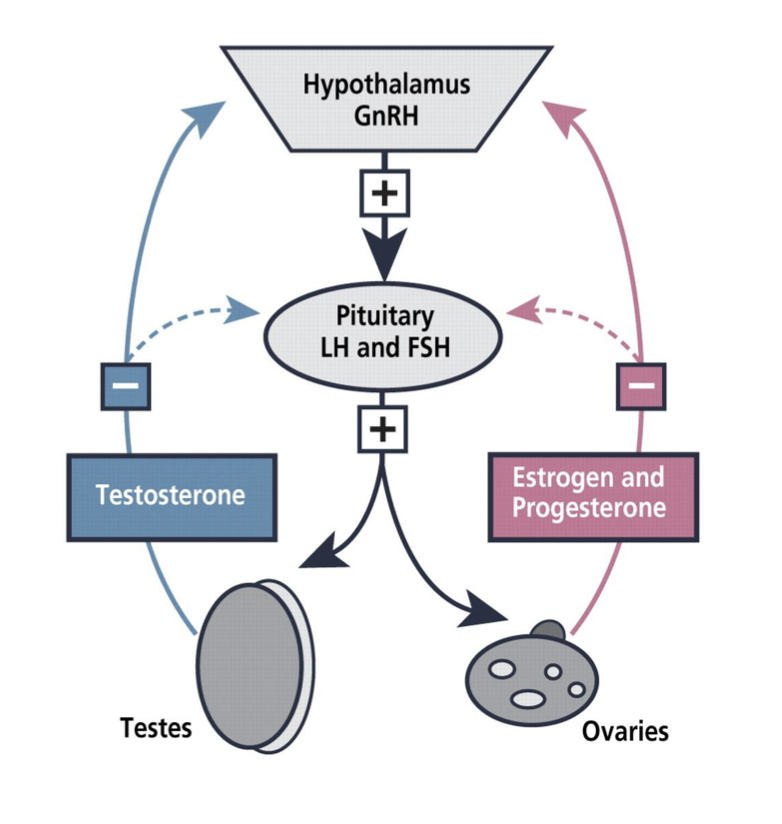
- The main hormones
- Estrogen
- Made in ovarian follicle, corpus luteum, adrenal cortex
- Promotes female characteristics and behaviour
- Oocyte maturation and uterine proliferation
- Progesterone
- Made in corpus luteum, adrenal cortex
- Maintains uterine secretion and stimulates mammary duct formation
- Testosterone
- Made in testes (Leydig cells), adrenal cortex
- Promotes male characteristics and behaviour
- Sperm development
- Production rate declines by age
- Estrogen
B. Female Reproductive Physiology
- Overview of the female system
- Uterus, fallopian tube, ovary, ligaments, etc
- Egg production and maturation
- The ovarian cycle
- Monthly series of events associated with the maturation of an egg
- 2 phases:
- Follicular phase
- Lasts approximately 14 days
- Egg development
- Luteal phase
- Lasts 14 days
- When corpus luteum active
- Follicular phase
- The ovarian cycle
- Follicular phase
- 1) Primordial follicle becomes primary follicle
- Occurs before the follicular phase
- Primordial follicle activated
- Cells around it grow, become cuboidal shaped
- Oocyte enlarges
- 2) Primary follicle becomes secondary follicle
- Follicular cells multiply
- When there are more than 2 layers
- Granulosa cells
- Oocyte grows rapidly
- 3) Secondary follicle becomes vesicular follicle
- When 6-7 layers of granulosa cells present antrum develops
- antrum= fluid filled cavity
- Antrum continues to expand
- Oocyte, surrounded by granulosa cells, perched on a stalk
- Capsule of granulosa cells called the corona radiata
- 1) Primordial follicle becomes primary follicle
- Ovulation
- Mature vesicular follicle bulges out from ovary and eventually pushes through the wall
- Some pain experienced by some women at this point: pain is called mittelschmerz
- In 1-2% of the time, more than one egg released
- Can result in multiple births
- Luteal phase
- After ovulation occurs, ruptured follicle collapses
- Remaining granulosa cells enlarge
- Combine with thecal cells to form corpus luteum
- Begins to secrete progesterone
- If pregnancy does not occur, degenerates after 10 days
- If pregnancy does occur: continues until placenta takes over role
- Hormonal regulation
- GnRH
- Gonadotropin releasing hormone
- Released by hypothalamus
- LH
- Luteinizing hormone
- Released by pituitary
- FSH
- Follicle stimulating hormone
- Released by pituitary
- Estrogen and progesterone
- Released by ovaries
- GnRH
- Changes in hormones during the ovarian cycle
- GnRH stimulates the release of FSH from pituitary
- FSH stimulates development of follicles
- Follicles begin to produce estrogen
- Estrogen tells pituitary to produce LH and uterus to start preparing for implantation
- High levels of LH stimulate ovulation
- Corpus luteum begins to produce progesterone
- LH and FSH drop
- If implantation doesn’t happen, all the work in the uterus is discarded
- Menstruation
- Cycle begins again
- Changes in the uterus
- Days 1-5: menstrual phase
- Uterus sheds most of the endometrium
- Days 6-14: proliferative phase (preovulatory)
- Endometrium rebuilds itself in response to rising estrogen levels
- Days 15-28: secretory phase (postovulatory)
- Uterine lining continues to develop in response to progesterone from corpus luteum
- Days 1-5: menstrual phase
- Changes in uterine glands during the menstrual cycle
- Proliferative stage
- Immediately after menstruation
- Straight tubules
- Secretory (luteal) phase
- Begins at ovulation
- Glandular development stimulated by progesterone
- Glands become highly coiled
- Proliferative stage
- Overview of the female reproductive cycle
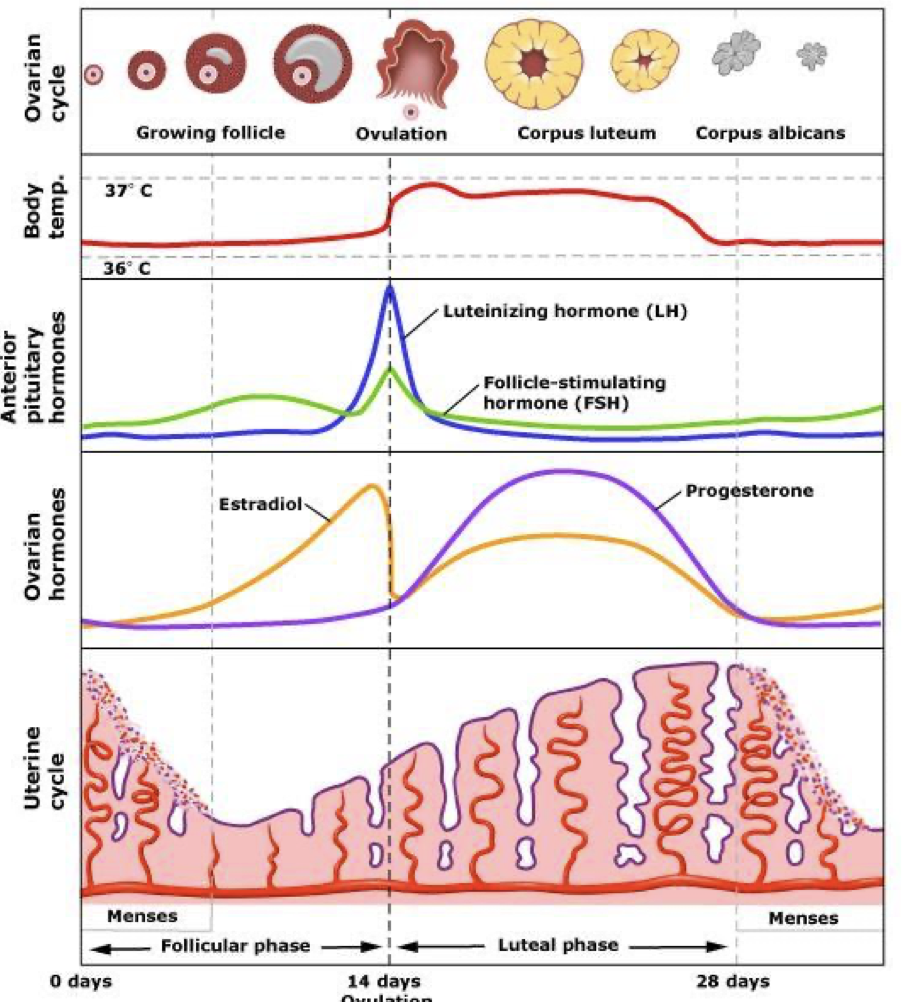
- LH and FSH spike during ovulation
- Progesterone spike after ovulation
C. Fertilization and Implantation
- Fertilization and implantation
- Goal of sperm: reach the egg
- Distance to travel: about 12 cm
- Sperm can reach egg within a few minutes
- However, can’t fertilize it until about 7 hours
- Must be capacitated
- Male reproductive physiology
- Penis, testes, epididymis, prostate, seminal vesicle, vas deferens, etc
- Sperm production
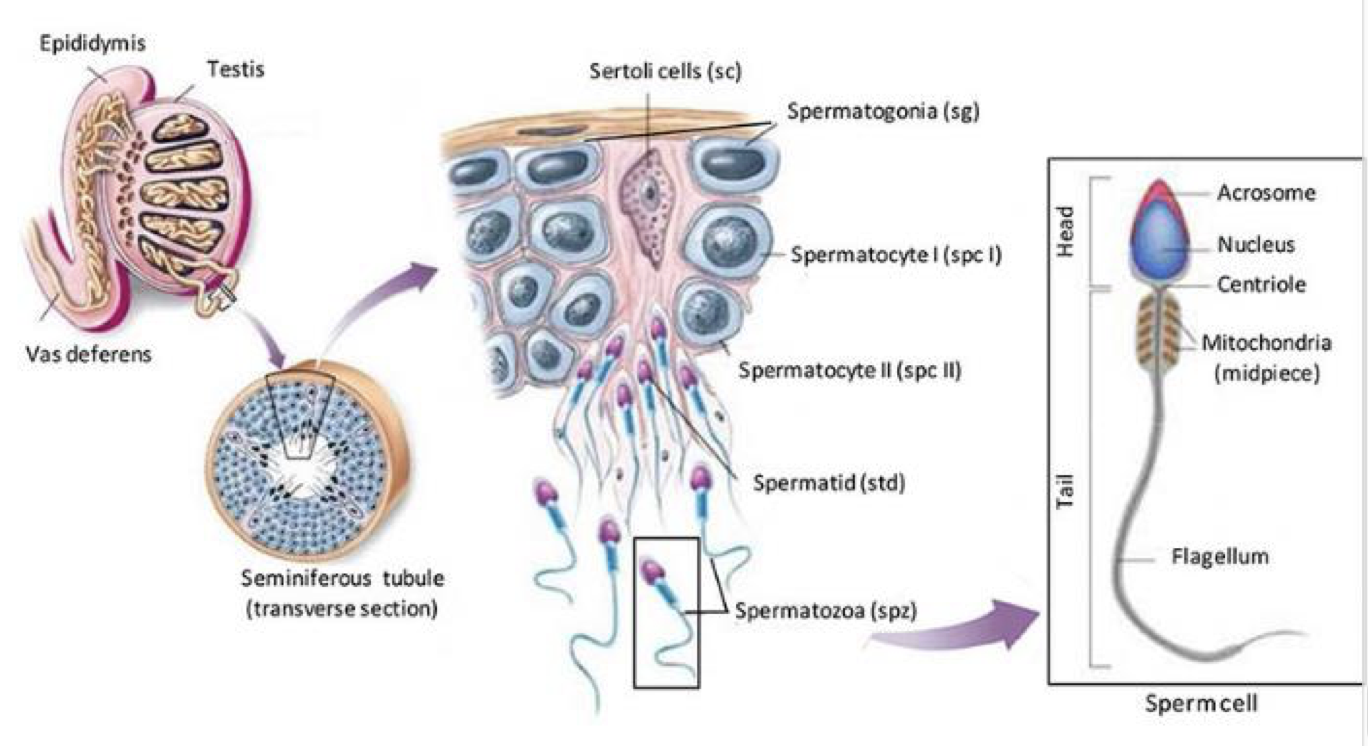
- Sperm capacitation
- Functional and morphological changes in the sperm to prepare for fertilization
- Tail beats more vigorously
- Plasma membrane prepares to fuse with egg
- Changes stimulated by conditions in the female reproductive tract
- Capacitated = proteins/surface molecules on the head of the sperm removed
- How the female helps sperm get closer to the egg
- Muscular contractions of the oviduct
- Peristalsis
- Oviductal fluid moved by oviduct contractions
- Also gets moved by cilia beating
- Chemical signals from egg
- Muscular contractions of the oviduct
- How the sperm fertilizes the egg
- Sperm needs to penetrate 2 layers around the egg before getting to the plasma membrane
- Corona radiata: granulosa cells that still surround oocyte
- Zona pellucida: clear layer on top of oocyte’s plasma membrane
- When sperm reaches zona pellucida, releases contents of acrosome
- Helps penetrate zona pellucida and plasma membrane
- Although hundreds of sperm may swarm to a single egg, only one will actually get inside
- The sperm fuses with the egg cell membrane
- Tail separates from the sperm head
- Male nucleus travels to the female nucleus in the centre of the cell
- Why doesn’t more than one sperm get in?
- Blocking polyspermy
- Polyspermy= more than one sperm fertilizing egg
- Entrance of sperm results in cortical reaction
- Granules just inside cell membrane released beneath zona pellucida
- Destroy sperm receptors
- Hardens fluid around egg
- Prevents further sperm entrance
- Blocking polyspermy
- Fertilization
- Occurs in the fallopian tube
- In about 1% of the cases, 2 eggs released by the ovaries
- Both fertilized
- Both implant and develop
- Dizygotic (fraternal) twins
- Less commonly, zygote splits during development
- As early as the 2-cell stage but more often when there are 70-100 cells
- Monozygotic (identical) twins
- Embryonic development
- The fertilized egg divides as it travels down the fallopian tube
- 4 or 5 rapid divisions
- Volume of zygote doesn’t change
- At this point it implants into uterine wall
- The fertilized egg divides as it travels down the fallopian tube
- Parts of the blastocyst
- Inner cell mass: becomes embryo
- Blastocoele: fluid filled cavity
- Trophoblast: becomes fetal part of placenta
- Implantation
- At the end of the first week, blastocyst comes into contact with uterine wall
- Embeds via trophoblast cells
- 50-75% fail to implant
- This is typically why pregnancy requires several ovulation cycles to achieve
- Blastocyst shed with uterine lining during menses
- Implantation is complete by the middle of the 2nd week
- A few days after implantation, home pregnancy test can give a positive result
- Due to presence of human chorionic gonadotropin (hCG) in urine secreted by trophoblast cells