Hypersensitivity and Autoimmunity
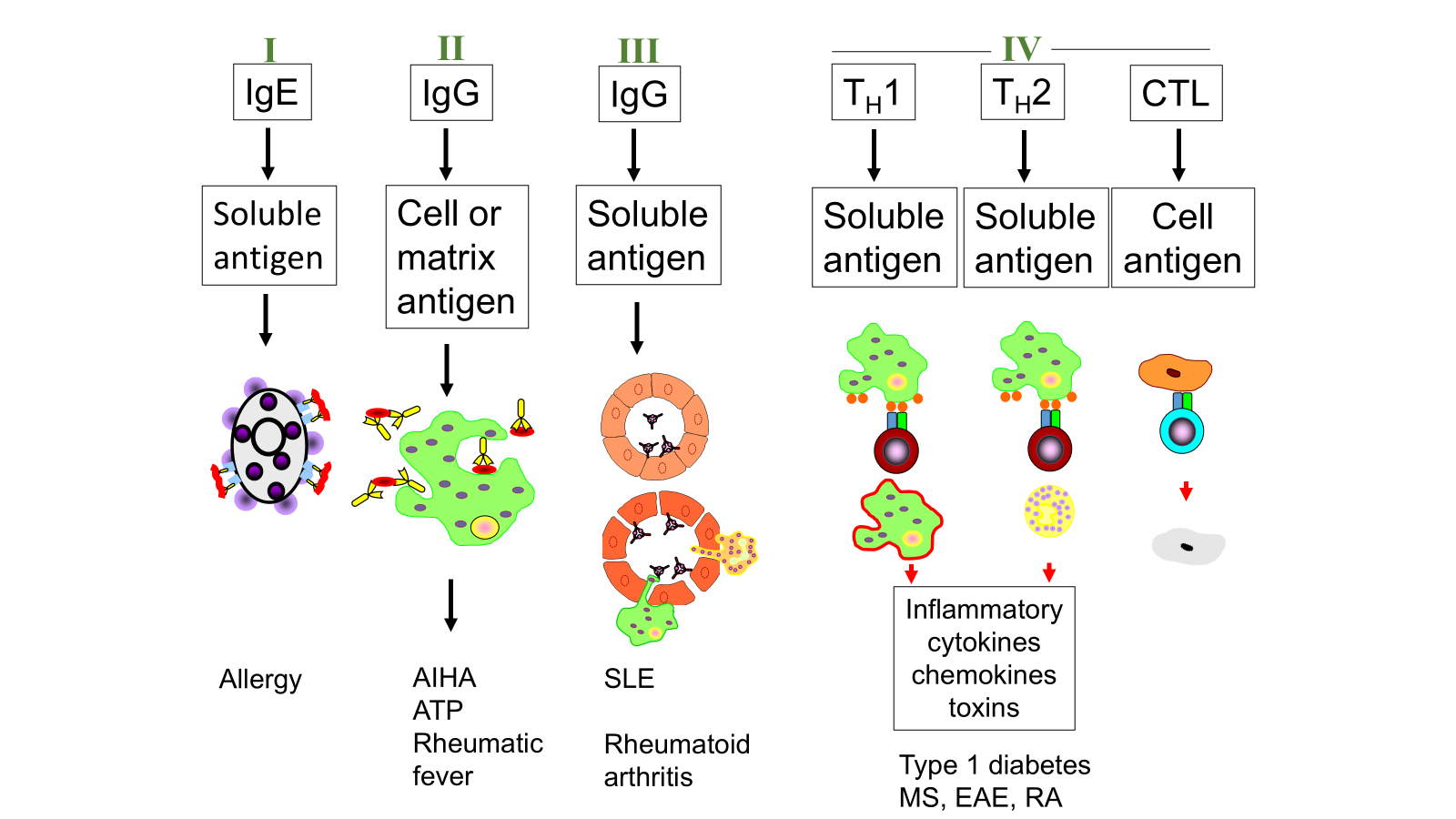
Learning Outcomes: • Contrast the mechanisms of Type I,II,III and IV hypersensitivity
• Understand how allergens can induce immediate immune responses during early phase allergy
• Understand the relationship between antibodies (IgE and IgG) and Fc receptors
• Define atopy
• Understand the differences between type II and III antibody mediated hypersensitivity
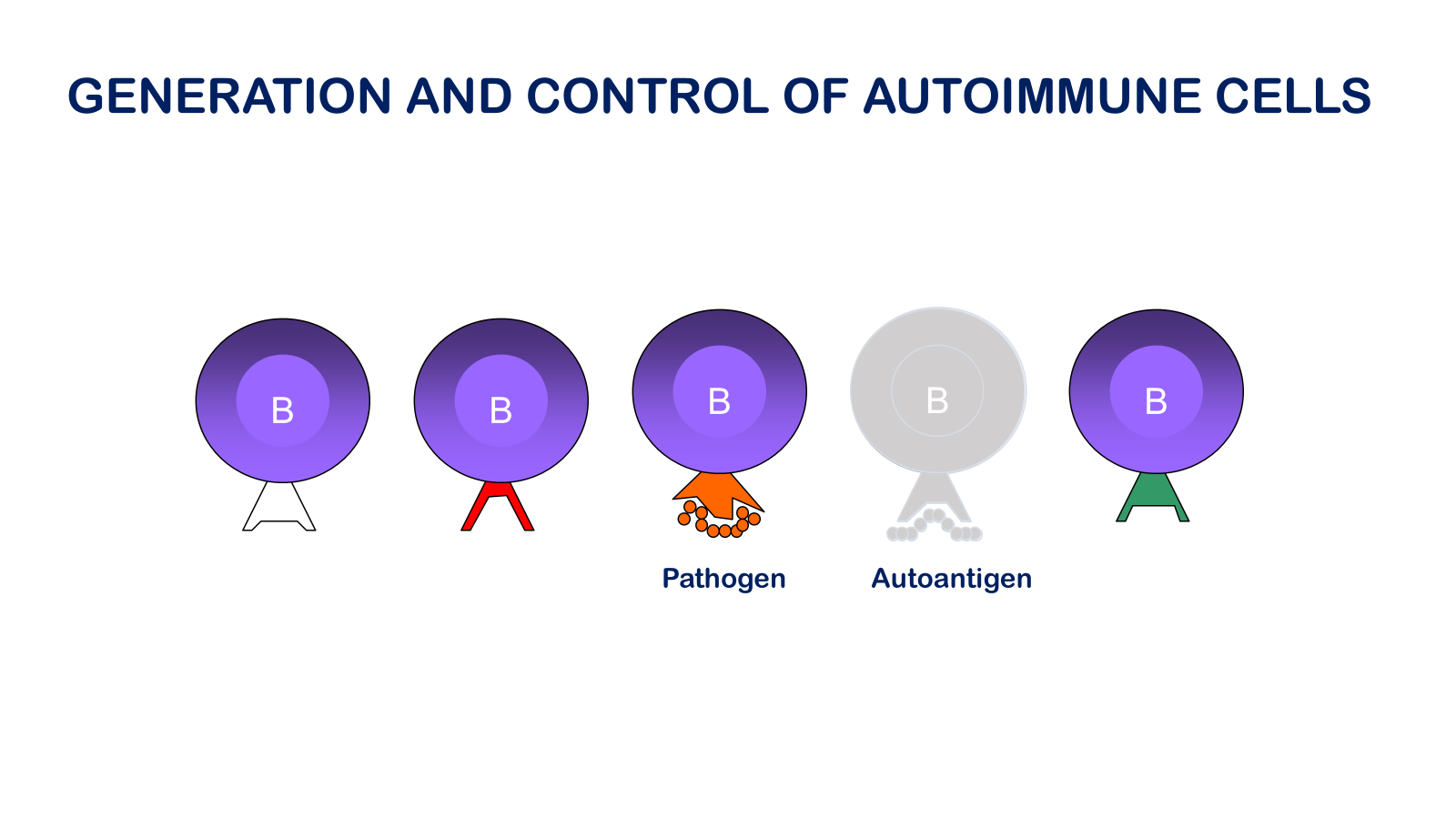
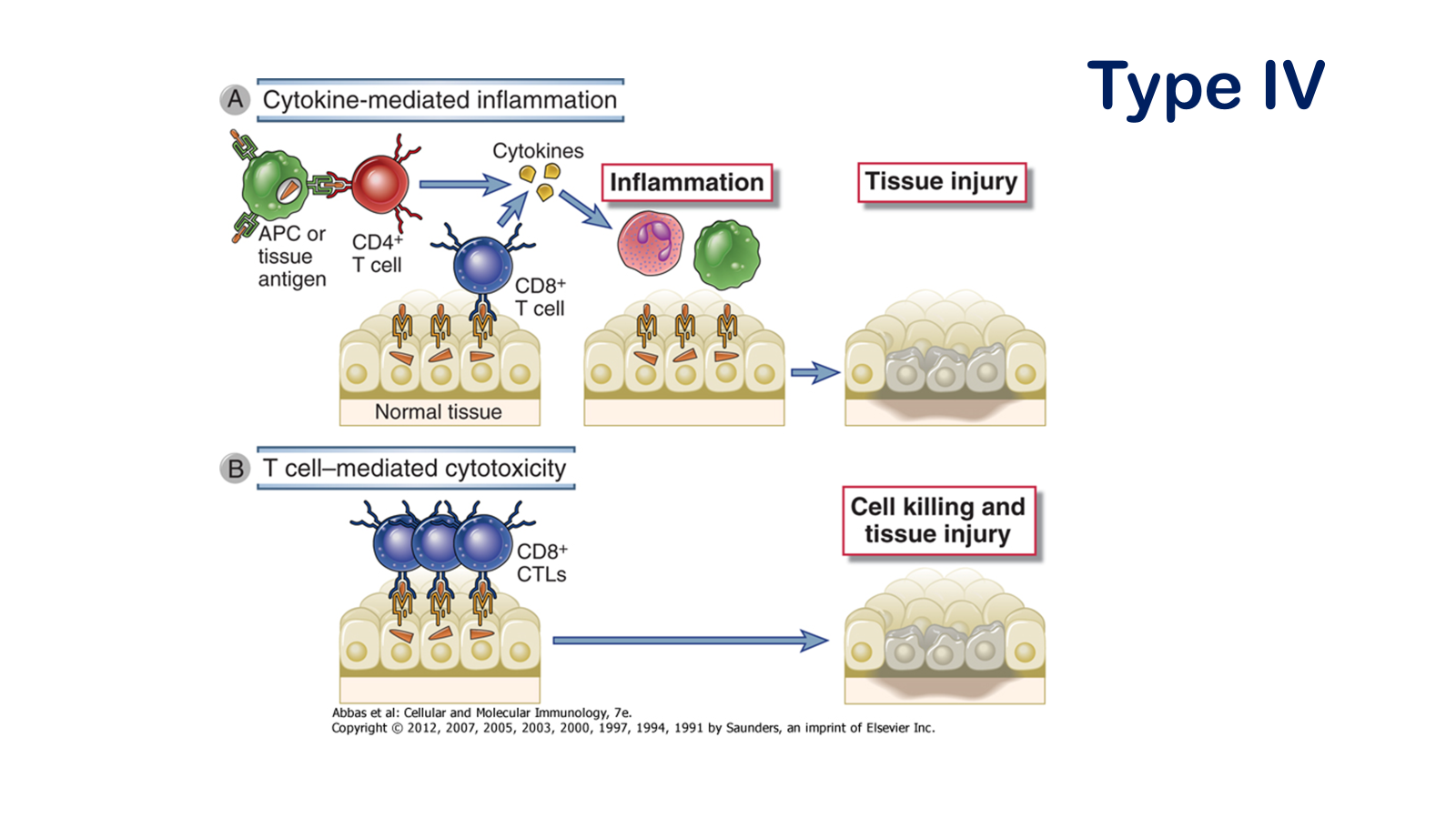
• Understand the factors mediated by T cells to cause tissue damage and autoimmune disease
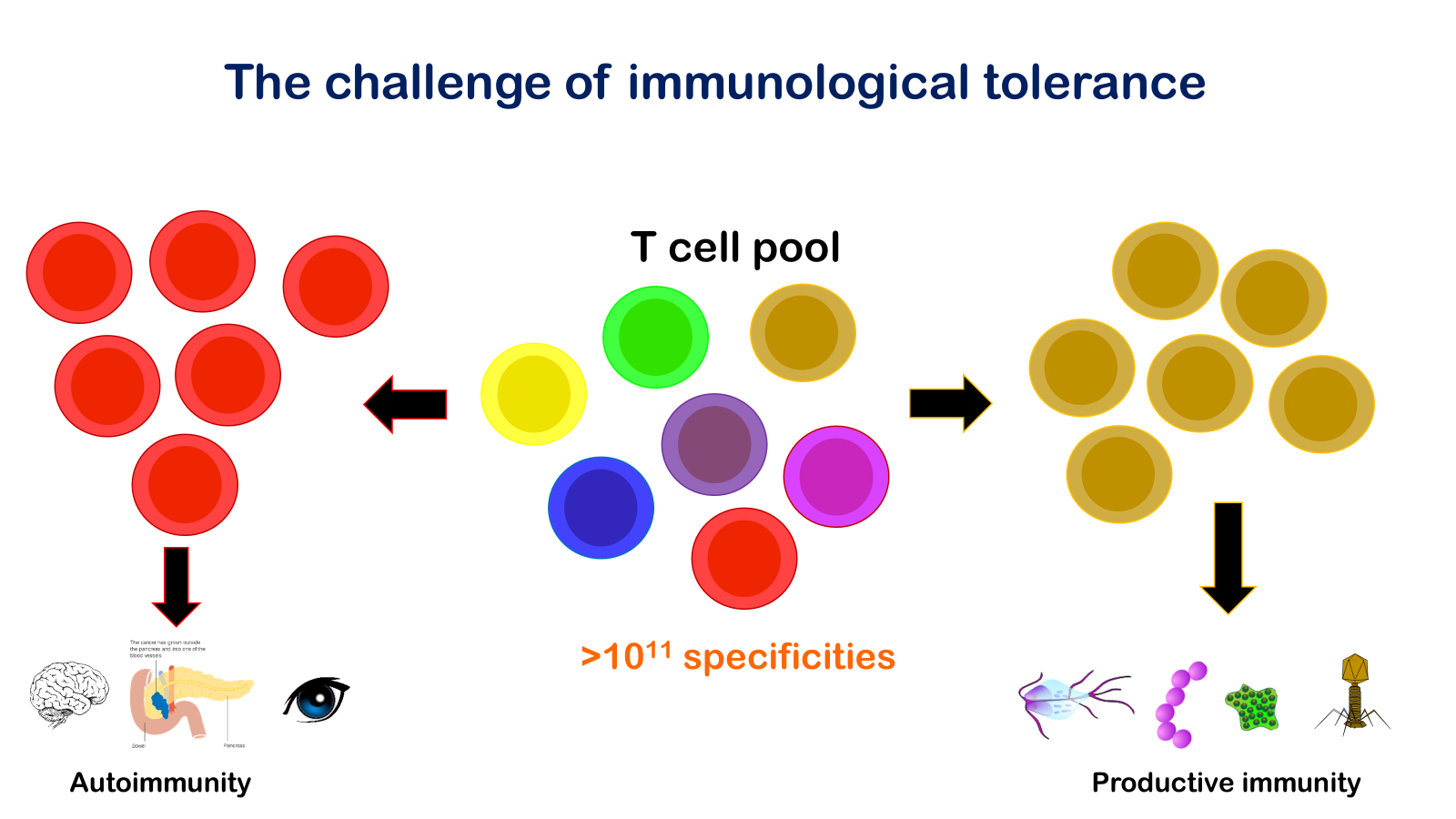
• Define immune tolerance and autoimmune disease
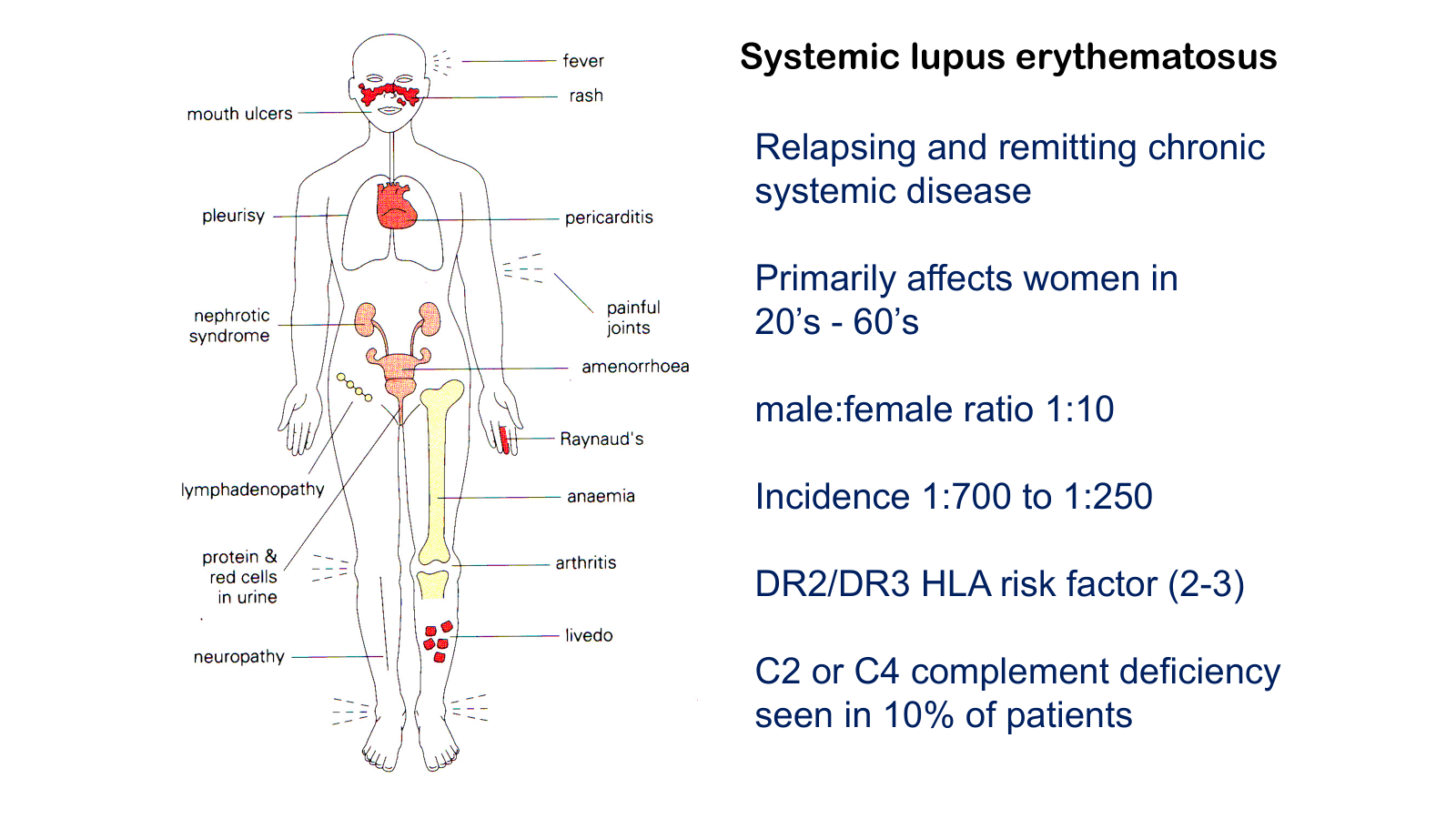
• Contrast systemic and organ specific autoimmune disease
specificity critical to type II immunoresponse
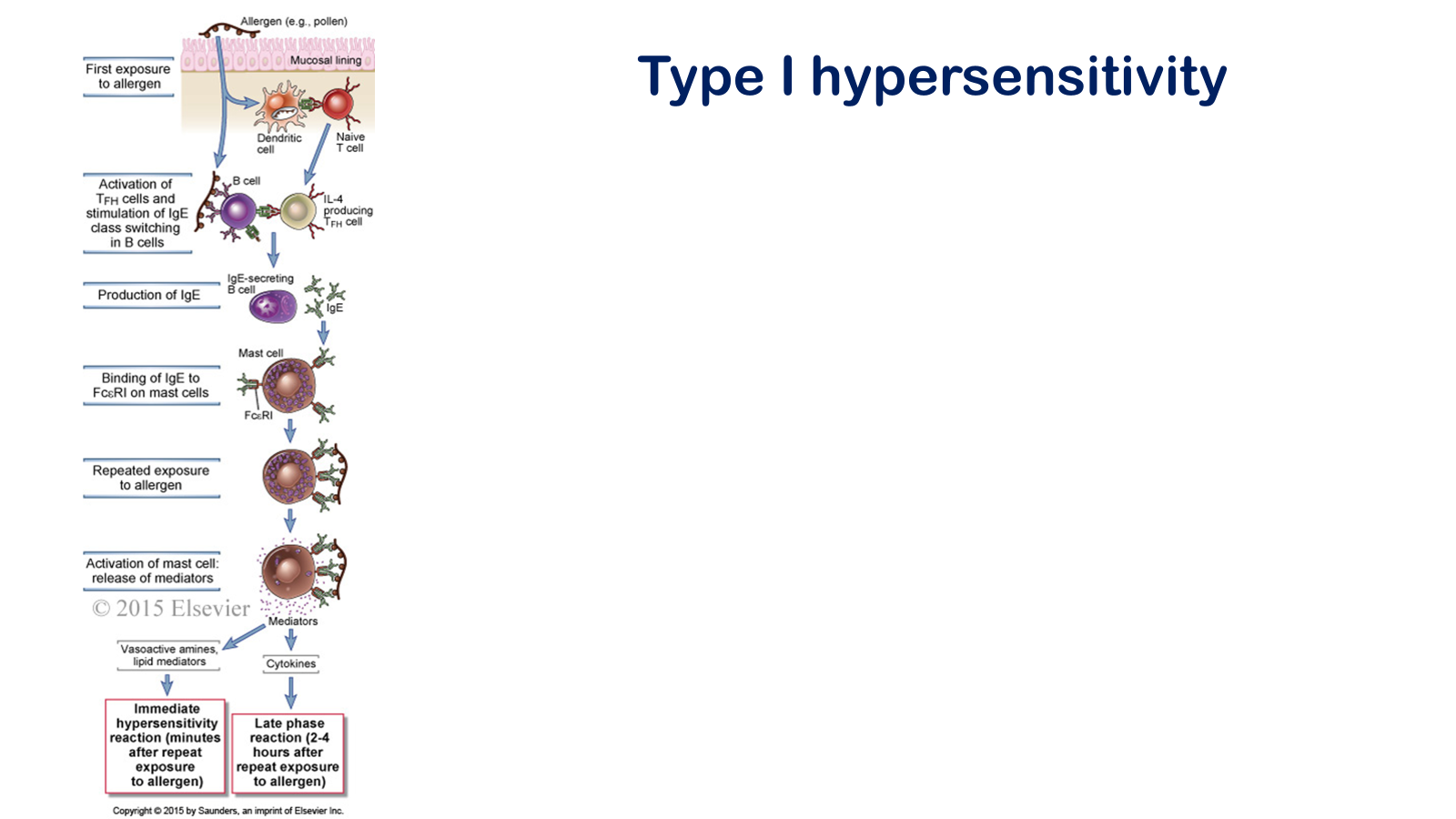
Figure 19-1 Sequence of events in immediate hypersensitivity reactions. Immediate hypersensitivity diseases are initiated by the introduction of an allergen, which stimulates TH2 reactions and IgE production. IgE sensitizes mast cells by binding to FcεRI, and subsequent exposure to the allergen activates the mast cells to secrete the mediators that are responsible for the pathologic reactions of immediate hypersensitivity
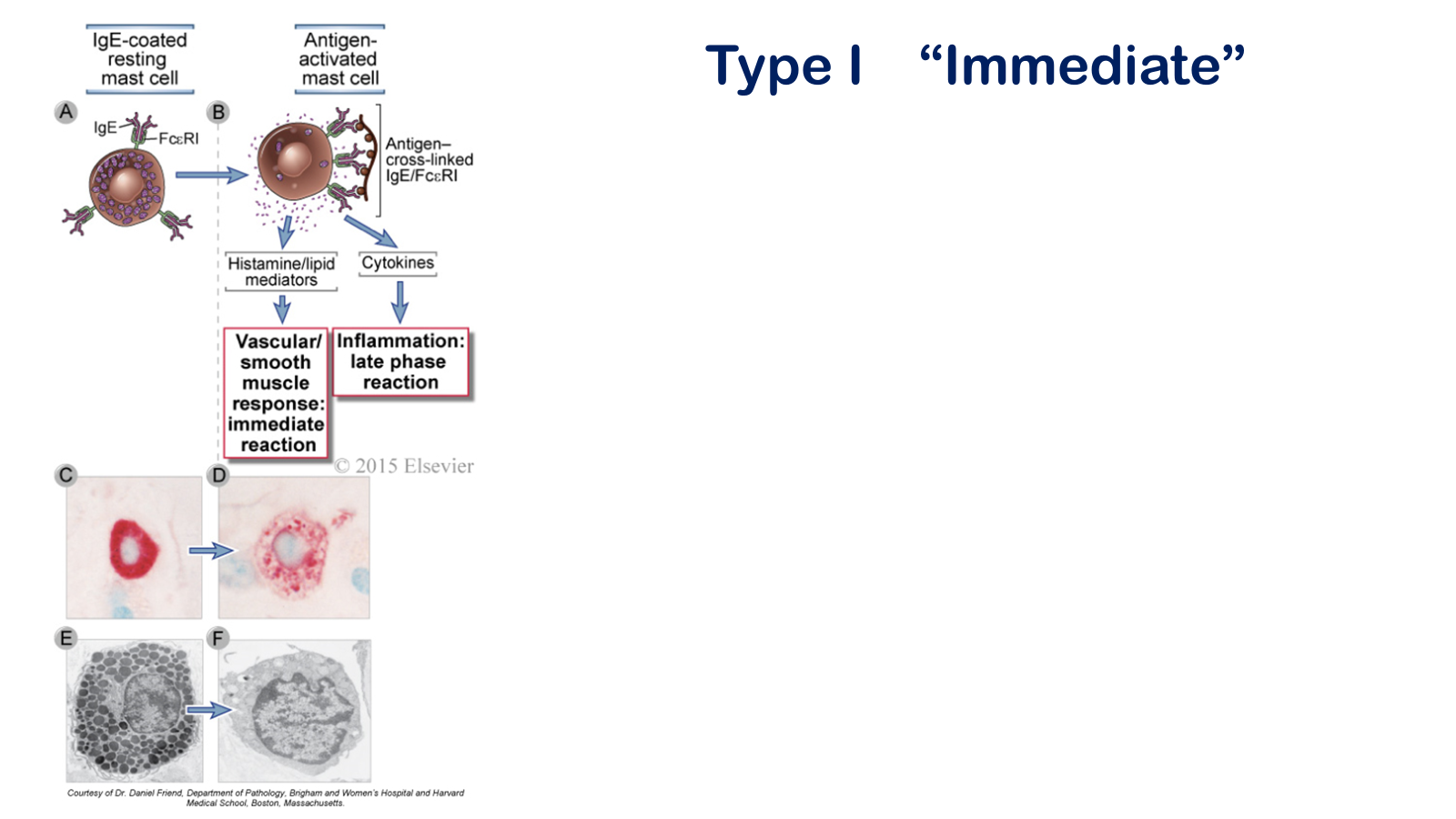
Mast cell activation. Antigen binding to IgE cross-links FcΕRI molecules on mast cells, which induces the release of mediators that cause the hypersensitivity reaction (A, B). Other stimuli, including the complement fragment C5a, can also activate mast cells. A light photomicrograph of a resting mast cell with abundant purple-staining cytoplasmic granules is shown in C. These granules are also seen in the electron micrograph of a resting mast cell shown in E. In contrast, the depleted granules of an activated mast cell are shown in the light photomicrograph (D) and electron micrograph (F).
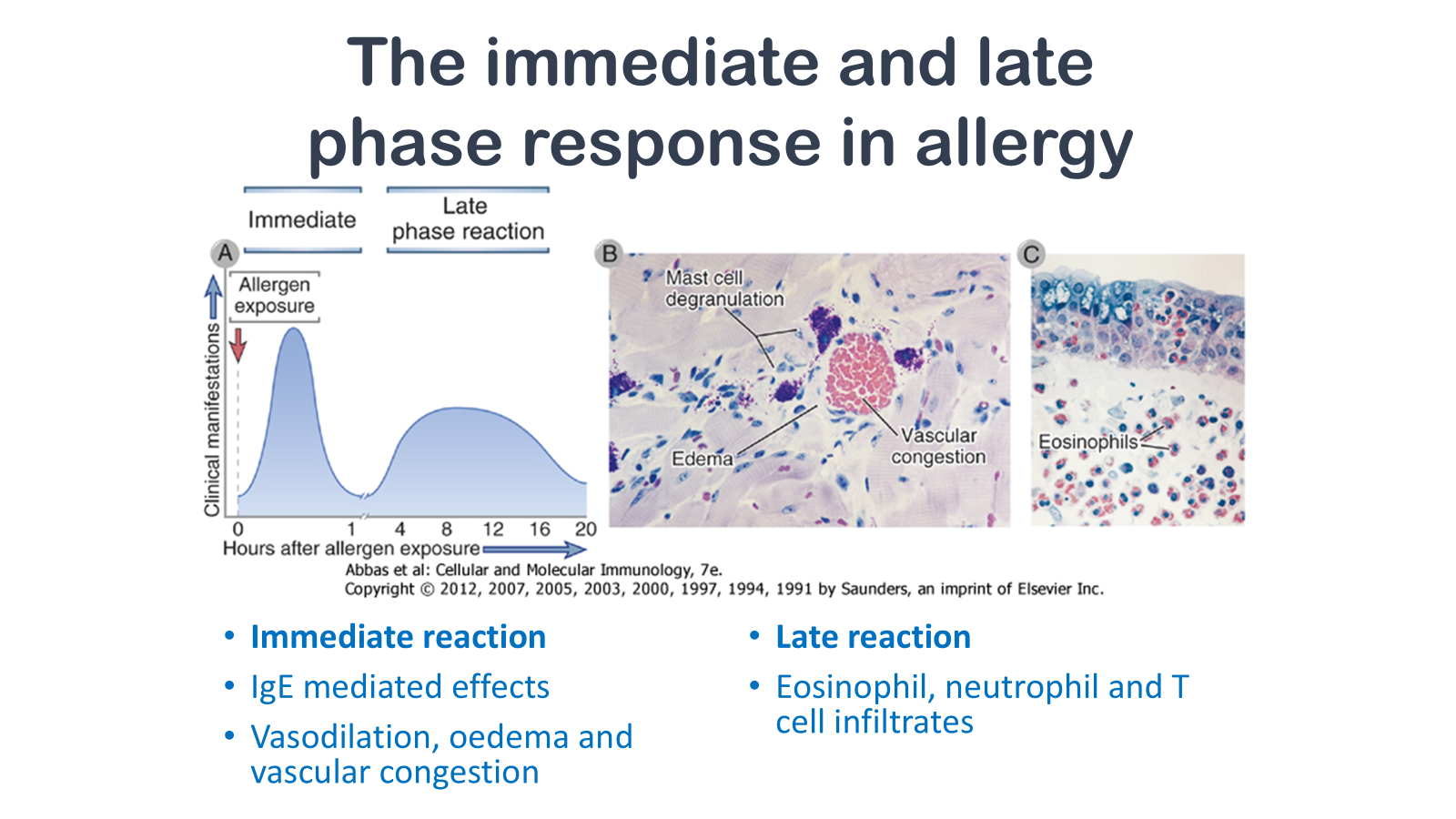
Figure 19-7 The immediate and late-phase reactions of allergy. A, Kinetics. The immediate vascular and smooth muscle reaction to allergen develops within minutes after challenge (allergen exposure in a previously sensitized individual), and the late-phase reaction develops 2 to 24 hours later. B, C, Morphology. The immediate reaction (B) is characterized by vasodilation, congestion, and edema, and the late-phase reaction (C) is characterized by an inflammatory infiltrate rich in eosinophils, neutrophils, and T cells. (Courtesy of Dr. Daniel Friend, Department of Pathology, Brigham and Women's Hospital, Boston, Massachusetts.)
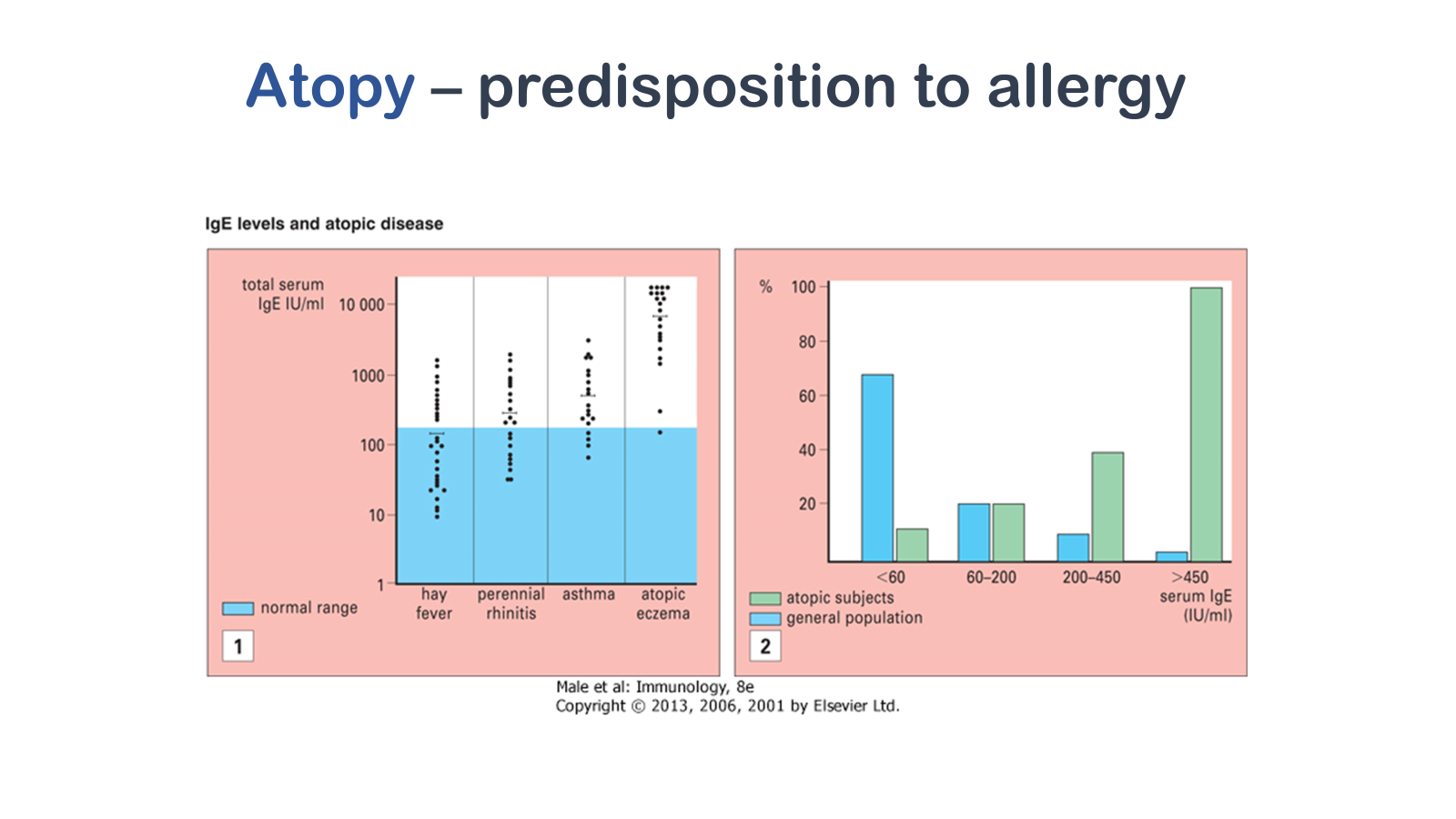
(1) The serum concentration of IgE (which is around 100 IU/mL) is only approximately 0.001% that of IgG (around 10 mg/mL) and comprises less than 0.001% of the total immunoglobulin. Levels in atopic patients tend to be raised, and this is especially so in atopic eczema (the International Unit [IU] for IgE equals 2.4 ng). (2) The higher the level of IgE, the smaller the percentage of the population is affected, but the greater the likelihood of atopy. Where the level is greater than 450 IU/mL the majority of subjects are atopic.
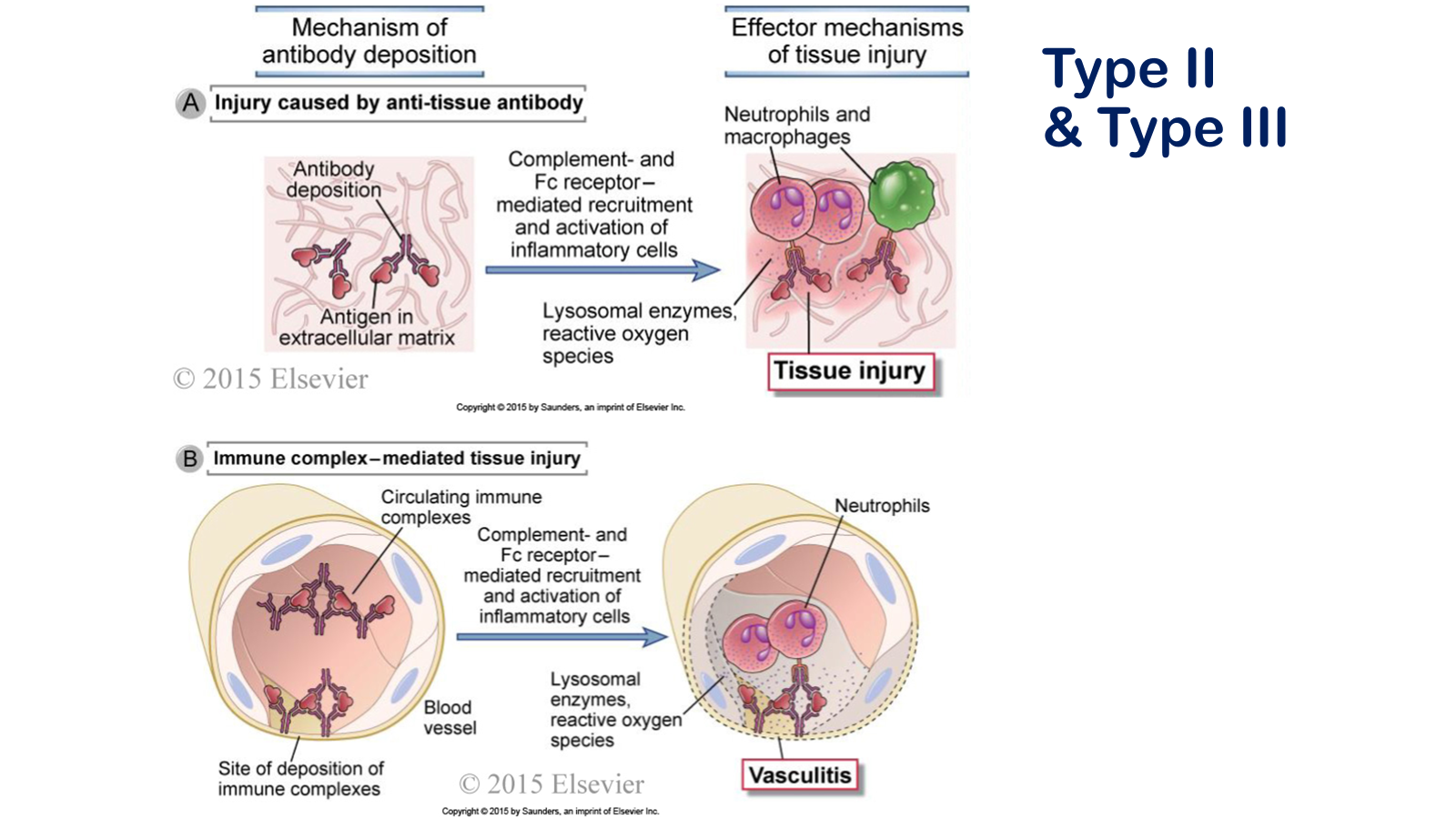
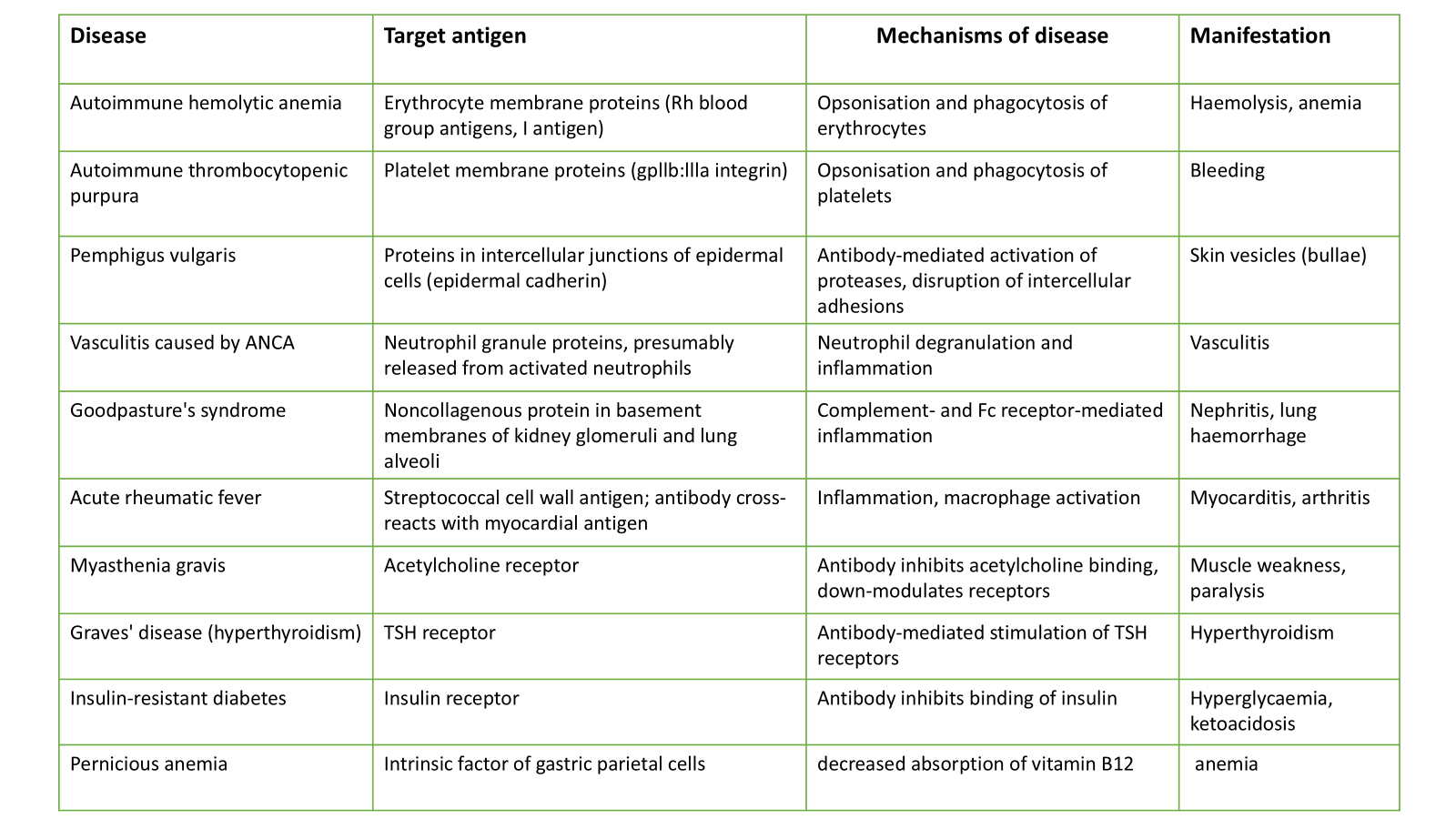
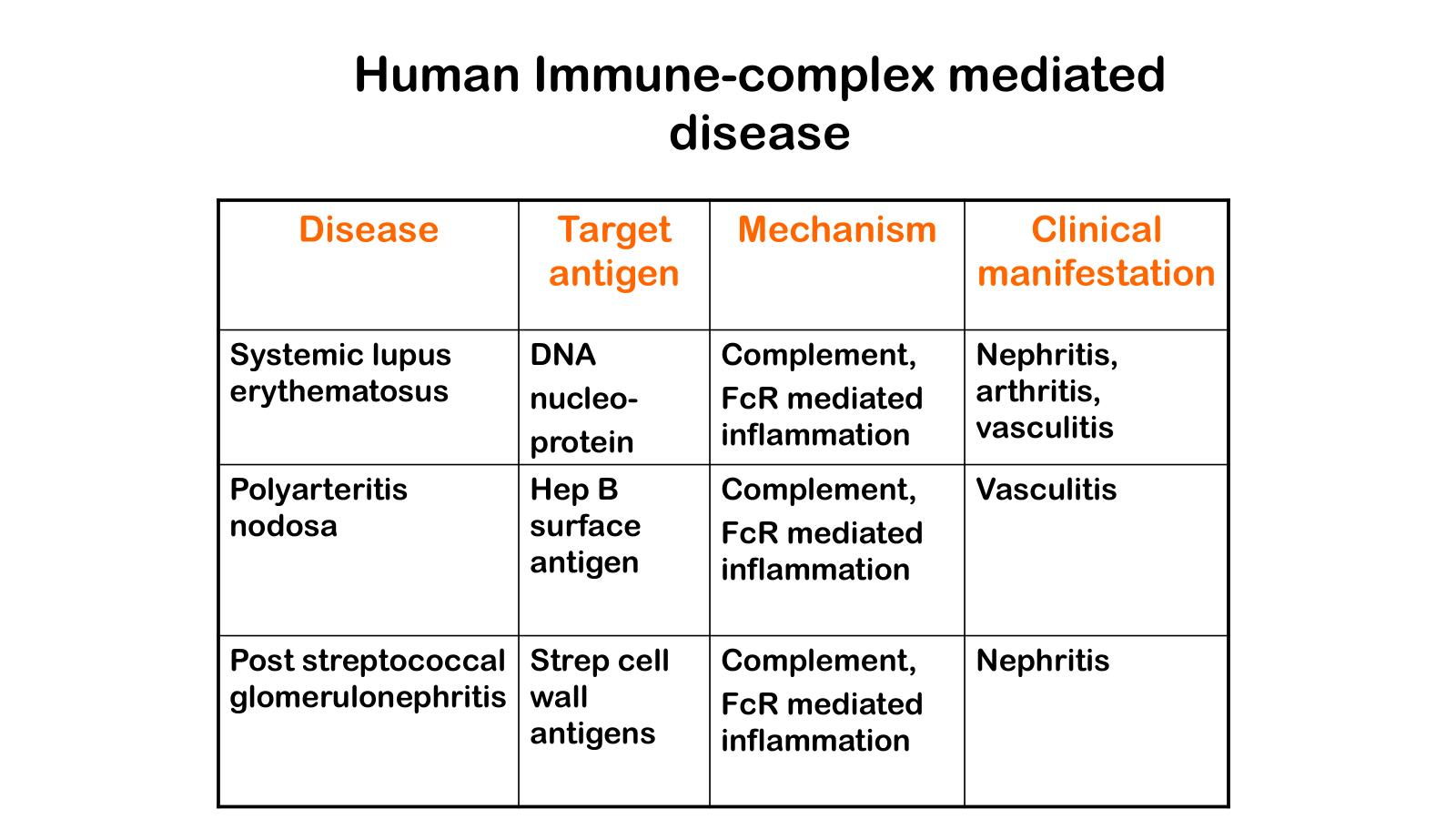
Types of antibody-mediated diseases. A, Antibodies may bind specifically to tissue antigens and the recruited leukocytes cause tissue injury. B, Complexes of antibodies and antigens may be formed in the circulation and deposited in blood vessels and other sites. These immune complexes induce vascular inflammation, and subsequent ischemic damage to the tissues. Antibodies against cellular proteins can also cause depletion of the cells and functional abnormalities (not shown).
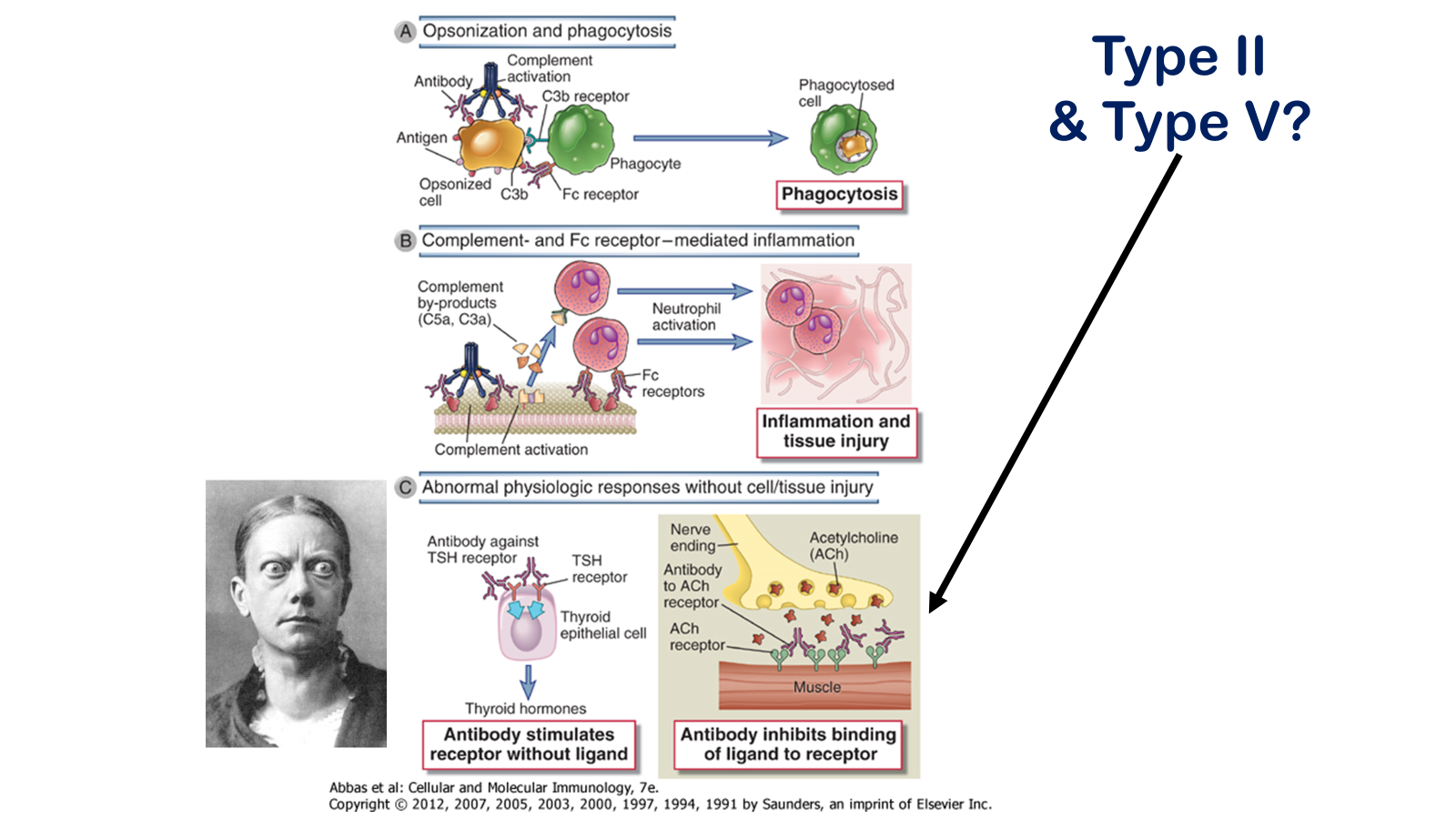
Effector mechanisms of antibody-mediated disease. A, Antibodies opsonize cells and may activate complement, generating complement products that also opsonize cells, leading to phagocytosis of the cells through phagocyte Fc receptors or C3b receptors. B, Antibodies recruit leukocytes by binding to Fc receptors or by activating complement and thereby releasing byproducts that are chemotactic for leukocytes. C, Antibodies specific for cell surface receptors for hormones or neurotransmitters may stimulate the activity of the receptors even in the absence of the hormone, as in Graves’ diseases (hyperthyroidism) (left panel), or may inhibit binding of the neurotransmitter to its receptor, as in myasthenia gravis (right panel). TSH, thyroid-stimulating hormone.
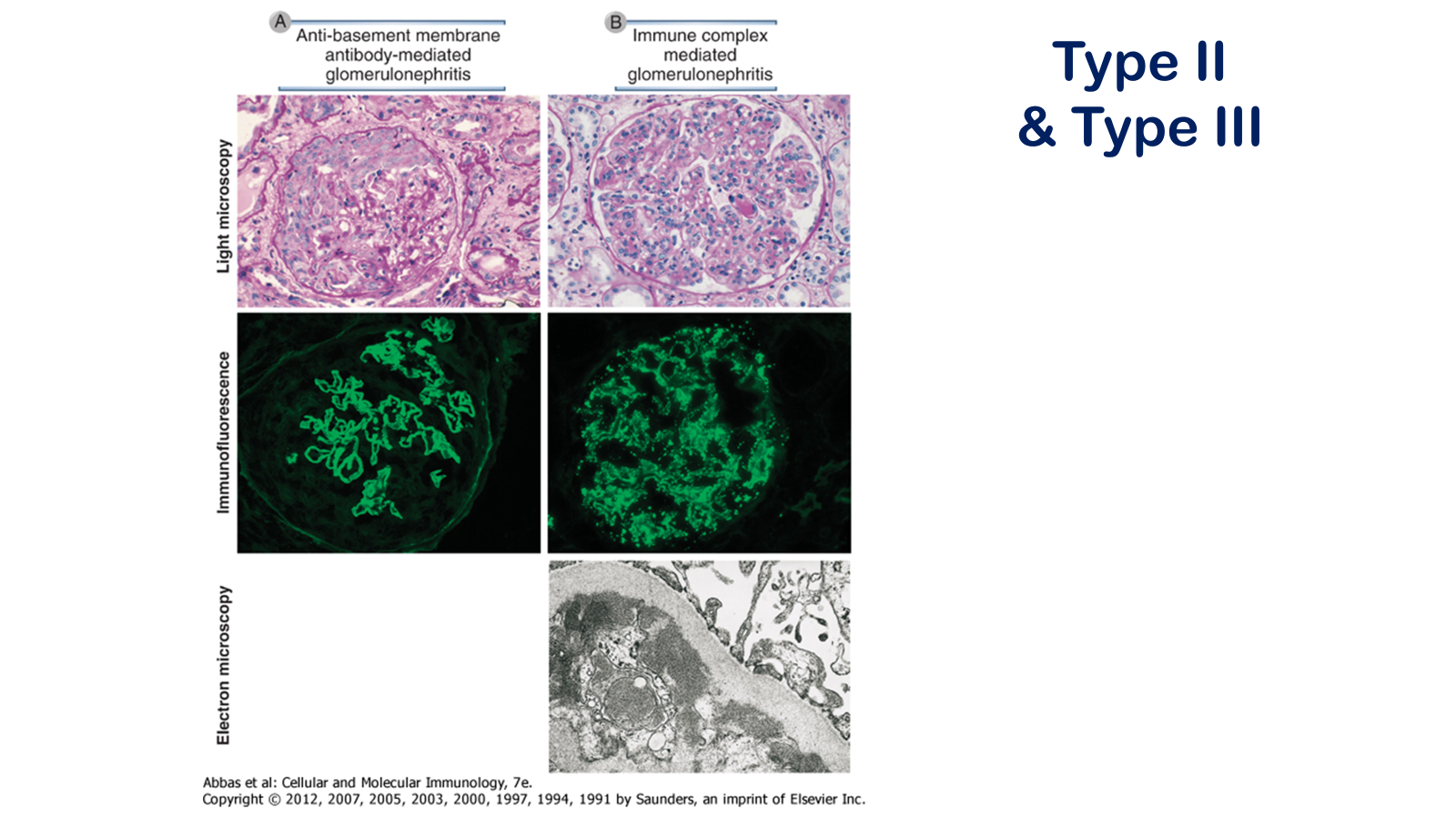
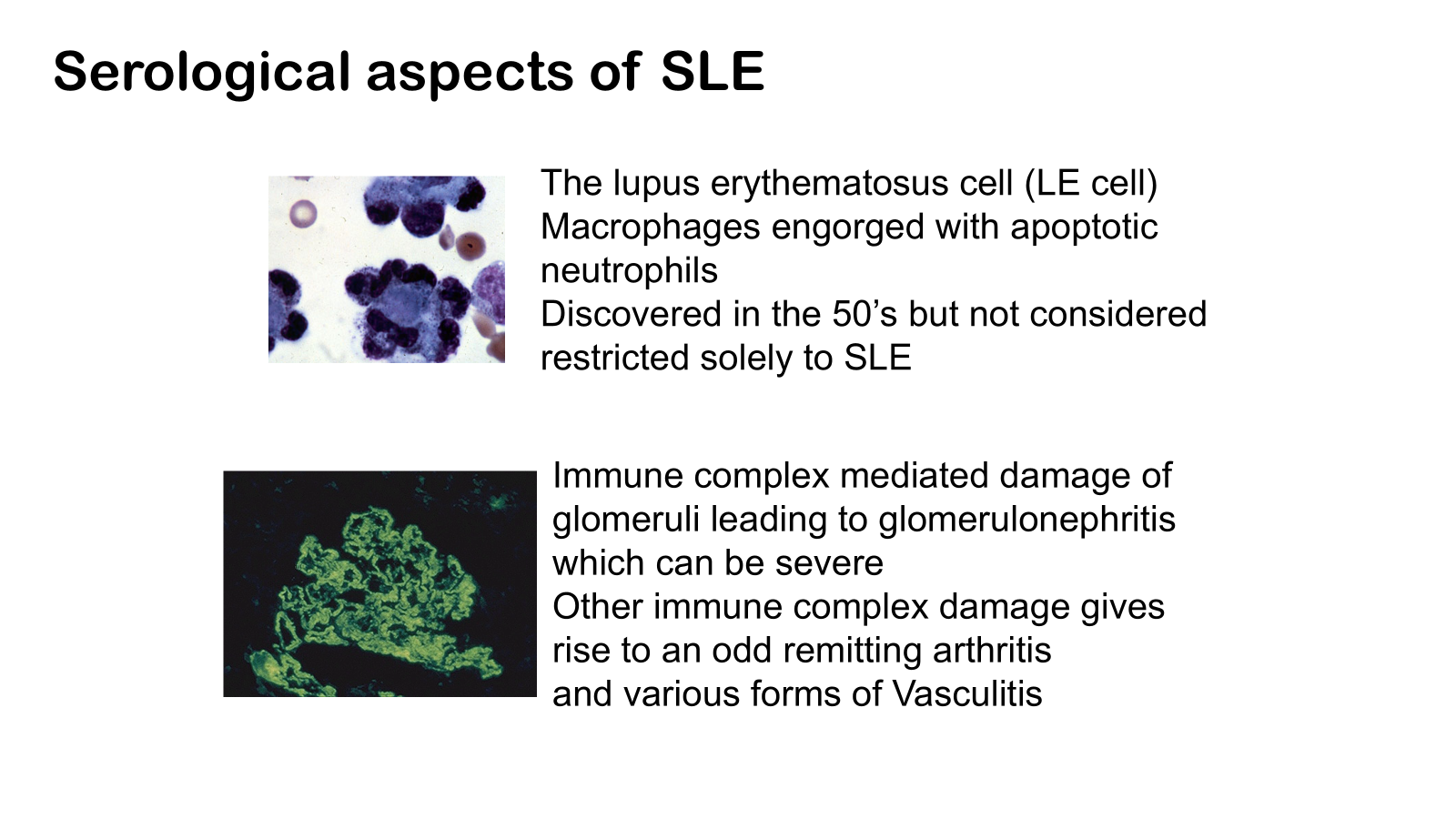
Pathologic features of antibody-mediated glomerulonephritis. A, Glomerulonephritis induced by an antibody against the glomerular basement membrane (Goodpasture's syndrome): the light micrograph shows glomerular inflammation and severe damage, and immunofluorescence shows smooth (linear) deposits of antibody along the basement membrane. B, Glomerulonephritis induced by the deposition of immune complexes (systemic lupus erythematosus): the light micrograph shows neutrophilic inflammation, and the immunofluorescence and electron micrograph show coarse (granular) deposits of antigen-antibody complexes along the basement membrane.
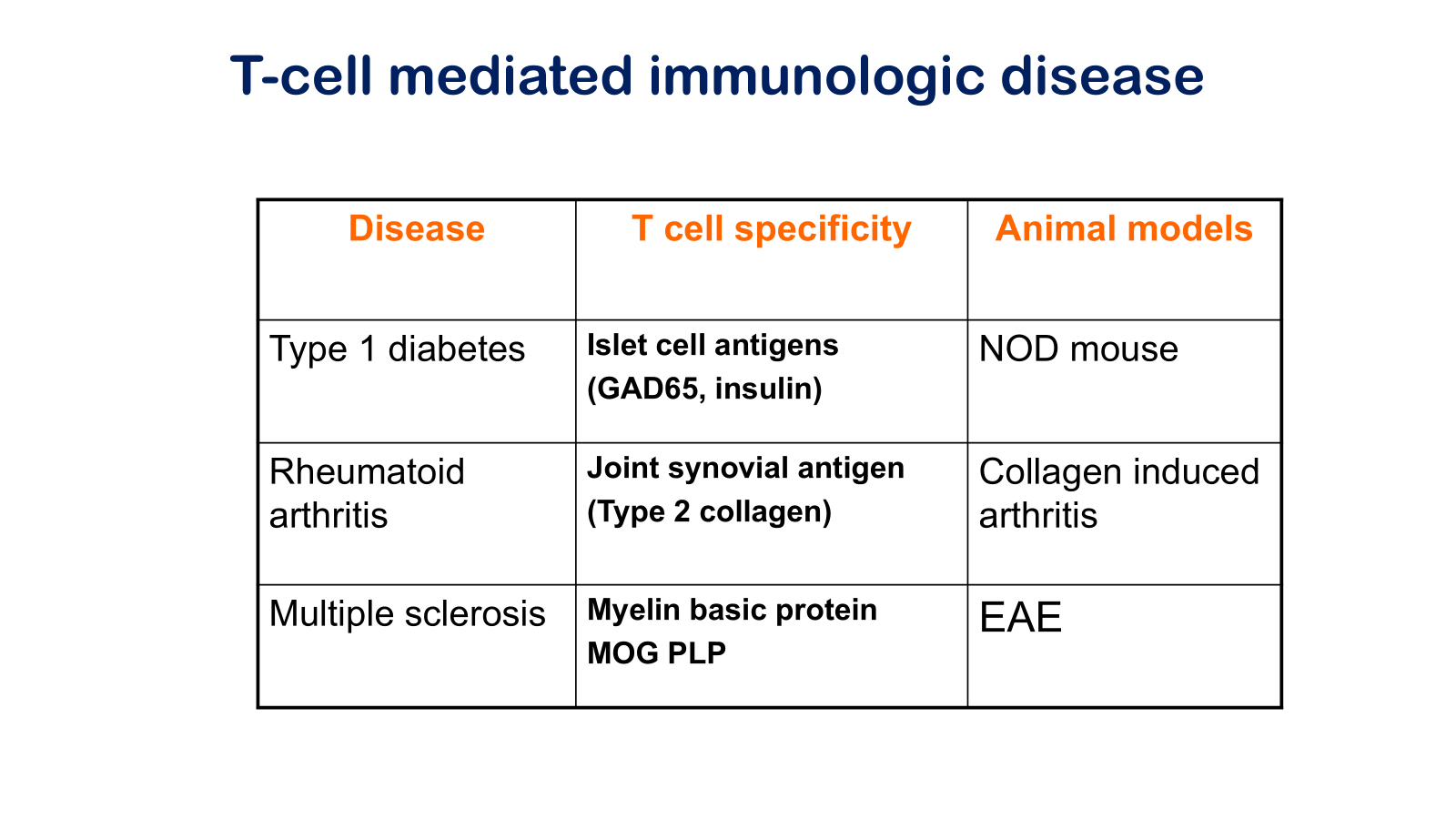
Experimental autoimmune encephalomyelitis
Myelin oligodendrocyte glycoprotein
Non-obese diabetic mouse
Glutamic acid decarboxylase 65
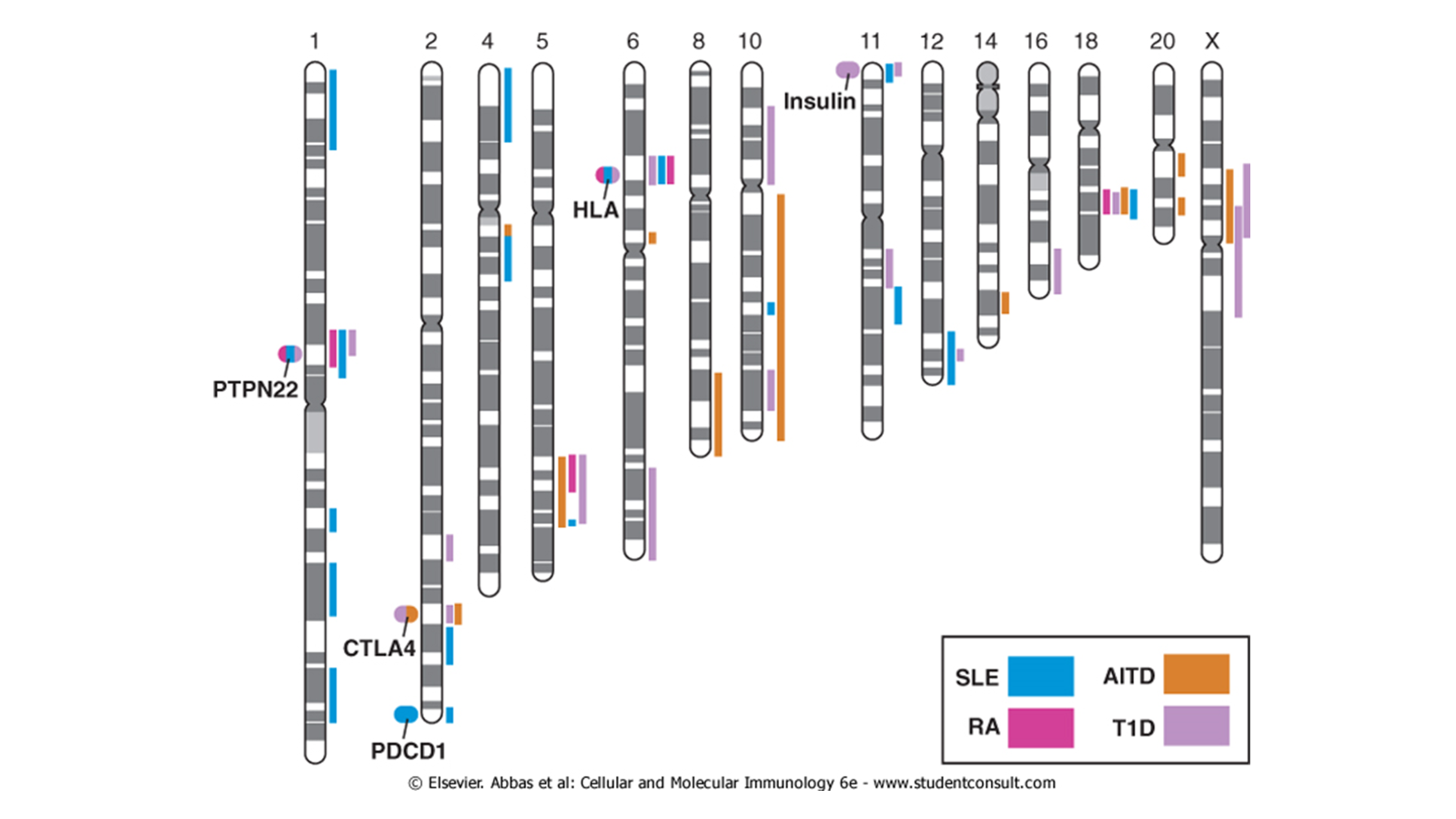
Susceptibility loci for autoimmune diseases. The chromosomal loci associated with some autoimmune diseases are shown. The location of candidate genes of immunologic interest are indicated as ovals on the left of the chromosomes. These ovals are color coded to indicate the diseases to which the genes are linked. SLE, systemic lupus erythematosus; AITD, autoimmune thyroid disease; RA, rheumatoid arthritis; T1D, type 1 diabetes
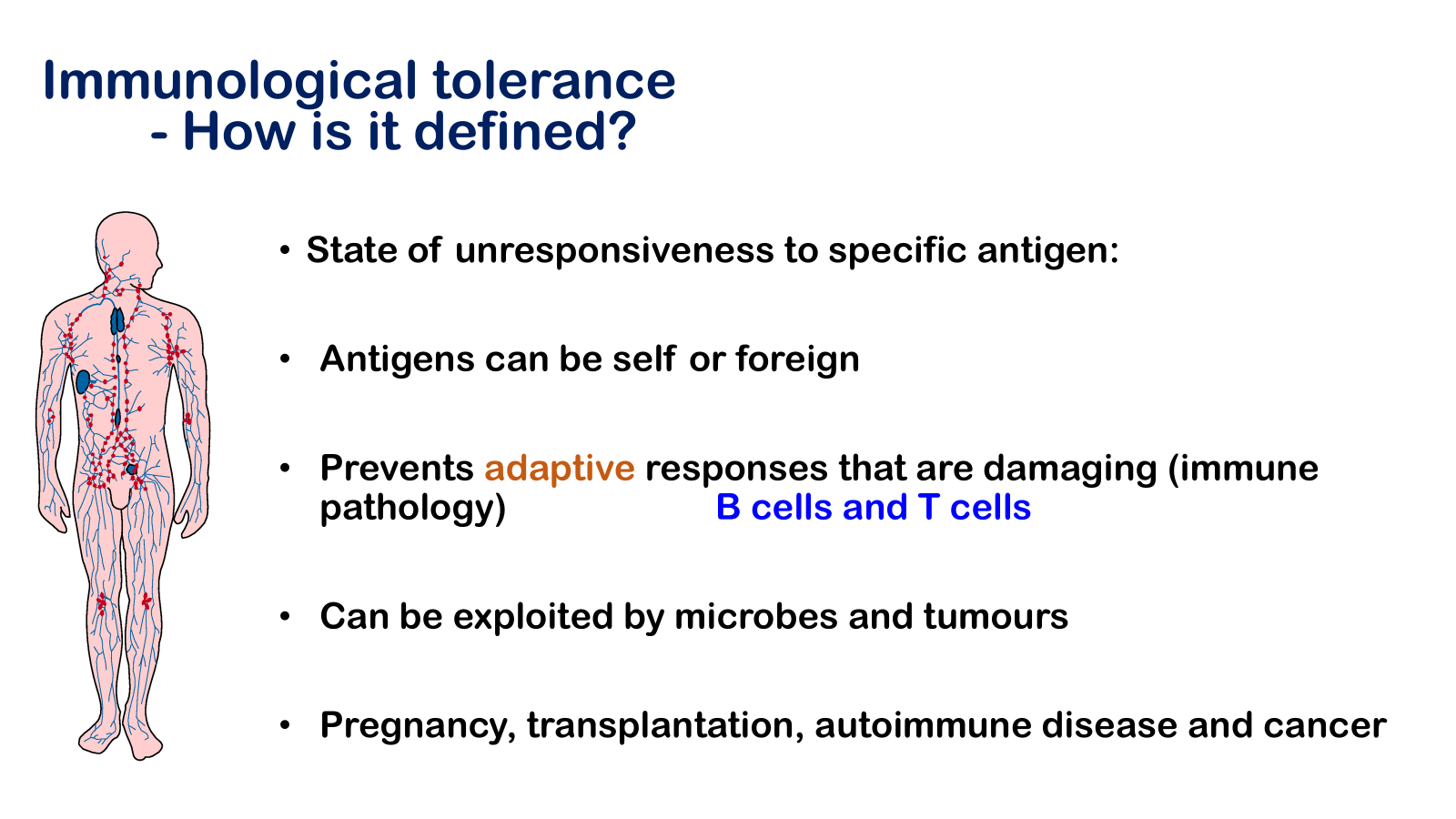
“Immunological tolerance” may be described as a state of indifference or non-reactivity towards a substance that would normally be expected to excite an immunological response. The term first came to be used in the context of tissue transplantation immunity, i.e. of the form of immunity that usually prohibits the grafting of tissues between individuals of different genetic make-up; and it was used to refer only to a non-reactivity caused by exposing animals to antigenic stimuli before they were old enough to undertake an immunological response.