Ch.16 Labor and Birth Processes Lecture notes (completed)
Overview of Labor and Birth Processes
The Five Major Factors Affecting Labor (The Five Ps)
Passenger (Fetus and Placenta): The movement of the fetus through the birth canal is determined by several factors: fetal head size, fetal presentation, fetal lie, fetal attitude, and fetal position.
Passageway (Birth Canal): Composed of the mother's rigid bony pelvis and the soft tissues of the cervix, pelvic floor, vagina, and introitus.
Powers (Contractions):
Primary Powers: Involuntary uterine contractions that signal the beginning of labor. These are responsible for effacement and dilation of the cervix.
Secondary Powers: Once the cervix is dilated, voluntary bearing-down efforts (pushing) by the mother augment the force of the primary powers.
Position of the Laboring Woman: The woman's position affects her anatomical and physiological adaptations to labor. Common positions include side-lying, upright, squatting, and the lithotomy position.
Psychological Response: The mother's mental state, influenced by culture, expectations, past experiences, and support systems, affects her ability to cope with labor.
The Passenger: Fetal Skull and Presentation
Composition of the Fetal Skull:
The fetal skull is composed of several bones: Frontal bone, Parietal bone, Temporal bone, and Occipital bone.
Sutures and Fontanels: These allow the skull bones to overlap (molding) so the head can pass through the pelvis. Key structures include the Lambdoid suture, Sagittal suture, Coronal suture, and Frontal suture.
Fontanels: The Anterior fontanel (diamond-shaped) and the Posterior fontanel (triangular).
Fetal Presentation: Refers to the part of the fetus that enters the pelvic inlet first and lies closest to the internal os of the cervix.
Cephalic: Head first.
Breech: Buttocks or feet first.
Shoulder: The scapula is the presenting part.
Fetal Lie: The relation of the long axis (spine) of the fetus to the long axis (spine) of the mother.
Longitudinal/Vertical: Fetal and maternal spines are parallel.
Transverse/Horizontal: Fetal spine is at a right angle to the maternal spine.
Fetal Attitude: The relation of the fetal body parts to one another.
General Flexion: The fetus is curled into a "ball" with the back rounded, chin on the chest, and thighs flexed on the abdomen. This is the normal posture. The head needs to be flexed in order for the baby to be passed during labor/birth.
Abnormal Attitude: Extension of fetal joints can result in prolonged labor or the need for instrumental delivery.
Biparietal Diameter (BPD): The largest transverse measurement of the fetal head, approximately . It is a critical indicator of head size.
Fetal Position, Station, and Engagement
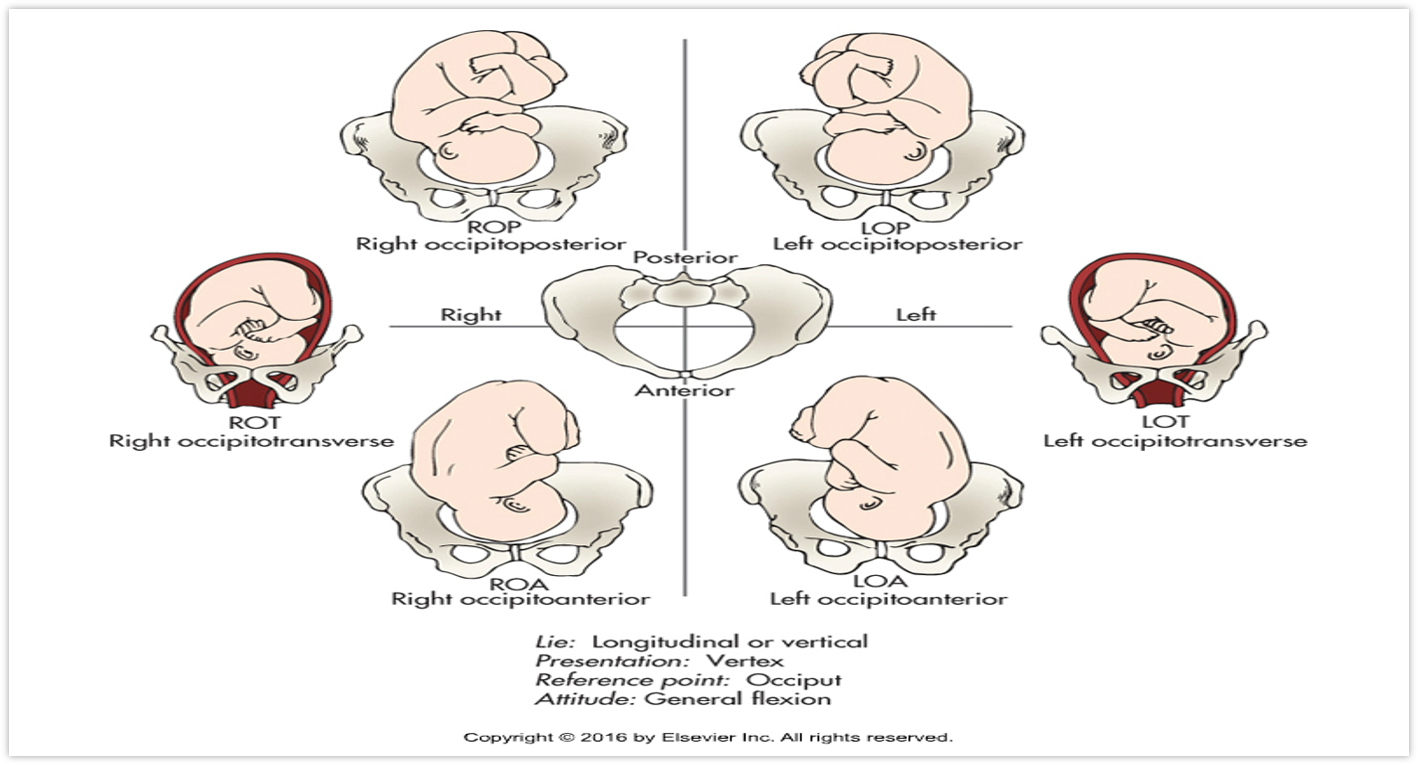
Fetal Position: The relationship of a reference point on the presenting part to the four quadrants of the mother's pelvis (e.g., Right Occipitoanterior - ROA, Left Occipitoposterior - LOP).
Reference Points: Occiput (O) for vertex, Sacrum (S) for breech, Mentum (M) for face/chin, and Sinciput (Sc) for brow/forehead.
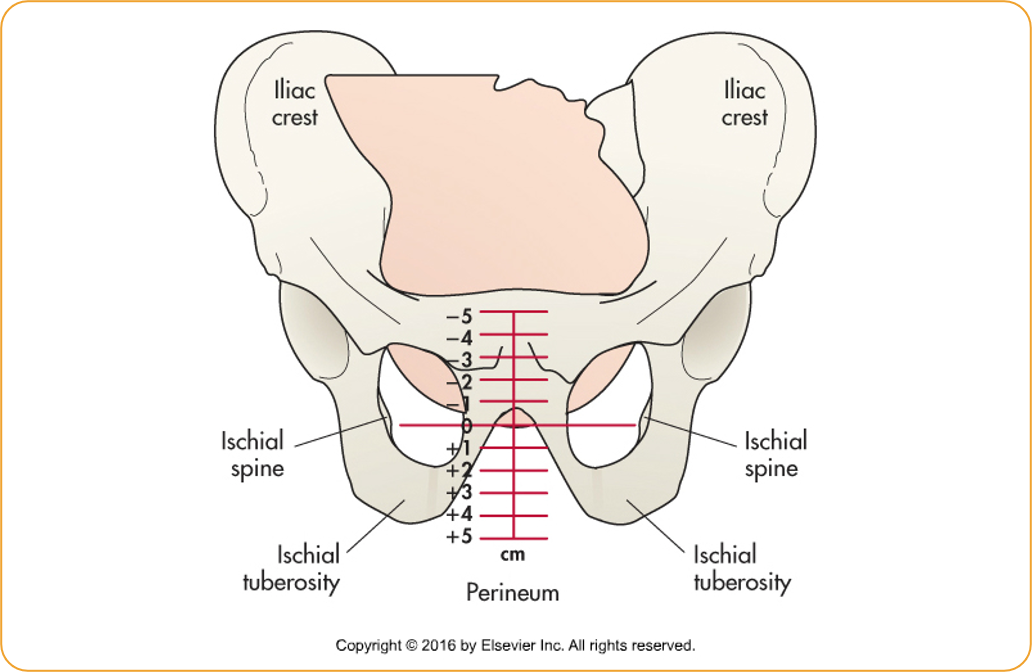
Station: The relationship of the presenting fetal part to an imaginary line drawn between the maternal ischial spines.
Measured in centimeters above or below the spines: to (above spines), (at spines), and to (below spines/nearing birth).
Engagement: Occurs when the largest transverse diameter of the presenting part (usually the BPD) has passed through the pelvic inlet into the true pelvis. This corresponds to a station of .This is a good sign that it is low.
Specific Fetal Presentations
Positions include: ROP (Right Occipitoposterior), ROT (Right Occipitotransverse), ROA (Right Occipitoanterior), LOA (Left Occipitoanterior), LOT (Left Occipitotransverse), and LOP (Left Occipitoposterior).
The Passageway: Bony Pelvis and Soft Tissues
Bony Pelvis Anatomical Structure: Composed of the ileum, ischium, pubis, sacrum, and coccyx.
Pelvis Divisions:
False Pelvis: The shallow upper section above the pelvic brim; it does not play a part in childbearing.
True Pelvis: The lower part involved in childbearing, further divided into the inlet (brim), mid-pelvis (cavity), and outlet.
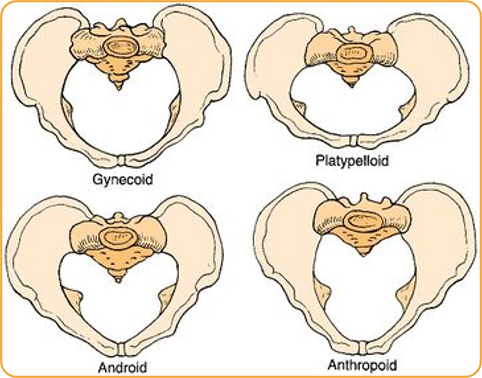
Pelvic Types:
Gynecoid: The classic female type ( of women).
Android: Resembling the male pelvis ().
Anthropoid: Oval shaped, wider anteroposteriorly ().
Platypelloid: Flat pelvis ().NOT IDEAL FOR CHILDBIRTH.
Soft Tissues of the Passageway:
Uterus: During labor, the uterine body differentiates into a thick, muscular upper segment and a thin, passive lower segment.
Cervix: Effaces (thins) and dilates (opens) to allow the fetus to pass.
Pelvic Floor Muscles: Assist the fetus in rotating into an anterior position.
Vagina and Introitus: Expand to accommodate the fetus.
The Powers: Uterine Contractions
Primary Powers (Involuntary):
Frequency: The time from the beginning of one contraction to the beginning of the next.
Duration: The length of a single contraction from start to finish.
Intensity: The strength of the contraction at its peak (acme).
Primary Function: Responsible for effacement (the shortening and thinning of the cervix) and dilation (the enlargement of the cervical opening).
Secondary Powers (Voluntary):
Invoked when the cervix is fully dilated ( or ).
Known as "bearing down," these are expulsive in nature as the mother pushes the fetus through the birth canal.
Contraction Cycle: Stages include Increment (building up), Acme (peak intensity, often reached at ), and Decrement (letting down). The resting phase follows each contraction.
Uterine Rings:
Physiologic Retraction Ring: Normal junction between upper and lower uterine segments.
Pathologic Retraction (Bandl) Ring: An abnormal junction associated with obstructed labor.
Process and Stages of Labor
Signs Preceding Labor (Box 16.1): Lightening (fetus dropping into the pelvis), lower back pain, and possible rupture of membranes (ROM).
True vs. False Labor:
True Labor: Regular contractions that induce progressive cervical changes (effacement and dilation).
False Labor: Irregular contractions with little or no cervical change.
The Four Stages of Labor:
First Stage: From the onset of regular contractions and effacement to full cervical dilation (6 cm).
Second Stage: From full cervical dilation () to the birth of the fetus.
Third Stage: From the birth of the fetus until the delivery of the placenta.
Fourth Stage: The period following placenta delivery up to hours after birth.
Mechanism of Labor: Cardinal Movements
Engagement: The greatest diameter of the fetal head passes through the pelvic inlet.
Descent: The continuous movement of the fetus through the birth canal (measured by station).
Flexion: The fetal chin moves toward the chest as the head meets resistance from maternal tissues, presenting a smaller diameter to the outlet.
Internal Rotation: The fetal head rotates to exit the outlet, which is widest in the anteroposterior (AP) diameter.
Extension (delivery of head): The occiput passes under the symphysis pubis; the face and chin emerge from the vagina.
Restitution: Once the head is delivered, it rotates briefly to align with the back.
External Rotation: The shoulders rotate to align in the AP diameter of the pelvis.
Expulsion: The anterior shoulder emerges first, followed by the rest of the body.
Maternal Physiological Adaptations to Labor
Cardiovascular/Respiratory: Increased pulse rate, blood pressure, and cardiac output during contractions.
Hematologic: Increased White Blood Cell (WBC) count (neutrophils) due to stress or tissue trauma.
Renal: Minor proteinuria () may occur due to muscle breakdown; fluid and electrolyte levels are altered by diaphoresis.
Integumentary: Stretching of vaginal introitus tissues occur.
Musculoskeletal: Mothers may experience back and joint aches due to increased joint laxity toward the end of term.
Gastrointestinal (GI): Motility, absorption, and gastric emptying are slowed during labor.
Endocrine: Labor is triggered by complex hormonal shifts, including a drop in progesterone and a rise in estrogen, prostaglandin (PGE), and oxytocin levels.
Review
Box 16.1