Pharmacodynamics
extracellular receptors
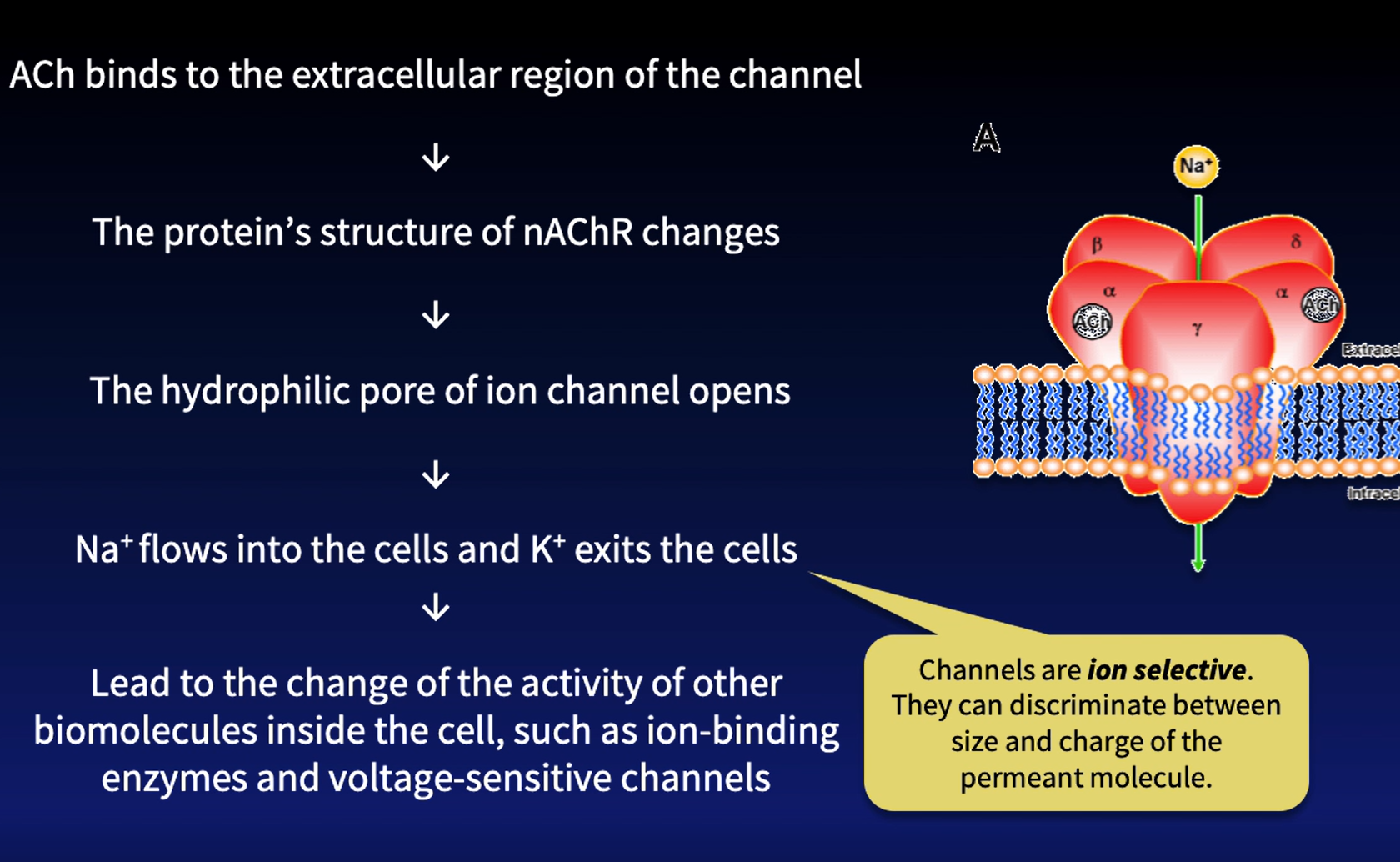
Ligand-gated Ion channels → modulated by drugs and endogenous ligands → causing conformational change to open or close the channel → made up of 4 polypeptide helices → reaction time: milliseconds
e.g: Nicotine Acetylcholine Receptor (nAChR) → recognize potassium (exits) and sodium (enters) → polarization and depolarization in nerve cells.
→ found in brain, salivary glands and smooth muscle (urinary bladder)
→ endogenous ligand: acetylcholine → neurotransmitter meant for muscle movements
→ function: nerve-muscle communication → controls muscle contraction
G-Protein Coupled Receptors (Many scientists are still exploring the different receptors and their relationship with the body) → reaction time: seconds
metabotropic receptors / 7-transmembrane receptors (1/3 or ½ of marketed drugs act on GPCRs)
endogenous ligand → peptides/ligands/lipids/sugars/drugs/proteins → all binds to GPCRs.
The 7 helices that form the N-terminal (outside) and C-terminal (inside) are able to conform to the shape/size of many ligands
G-protein → alpha, beta and gamma subunit → binds to GTP and GDP (initially bind to it)
guanosine triphosphate unit and guanosine diphosphate.
e.g. Muscarinic Acetylcholine Receptor → M1 to M5 → main focus: M3
found in brain, salivary glands and smooth muscle (urinary bladder) & EYES
both modulated by acetylcholine
Stimulate secretion of salivary gland, regulates contraction of smooth muscle
Mechanism of e.g.
inactive → bound to GDP. active → bound to GTP
In the absence of ACh, G-protein complex binds to nearby 7TM when it is bound to GDP via the alpha subunit.
/
In the presence of ACh → conformational change on molecular level → activates G-protein, GDP replaced by GTP on the alpha-subunit , leading to the dissociation of the G-protein into its active components, allowing for downstream signaling pathways to be initiated.
dissociation→ meaning of complex compounds etc.. being broken down into simpler components.
benign prostate hyperplasia → causes the person to feel increased urge to urinate → M3 is still working properly, however because of the enlarged prostate pressing on the bladder, the body feels that the bladder’s capacity to hold urine is lower → both M3 and the enlarged prostate will press down and cause the urinary bladder to contract MORE.
Main purpose of M3 Acetylcholine receptor → reduce the activity of M3 in someone who has an enlarged prostate to reduce muscle contraction in the urinary bladder to reduce the urge to urinate.
inducing action means to “cause” something or an action to occur in the body in response to the stimulus.
Receptor Tyrosine Kinase → very wide/large receptor in the body → reaction time: hours
ligand-binding domain is made up of at least 1000 amino acid residues and an intracellular domain of various sizes and functions.
receptors that are meant for many growth factors
controls cell division, growth, differentiation, inflammation, tissue repair, apoptosis(intentional/controlled cell death) and many immune responses.
process of differentiation → it is the process where unspecialized stem cells that are produced in the body are specializing into different specialized cells that perform specialized functions (for e.g. RBCs and WBCs and Platelets)
e.g. Insulin Receptors or (Another): Cytokine Receptors
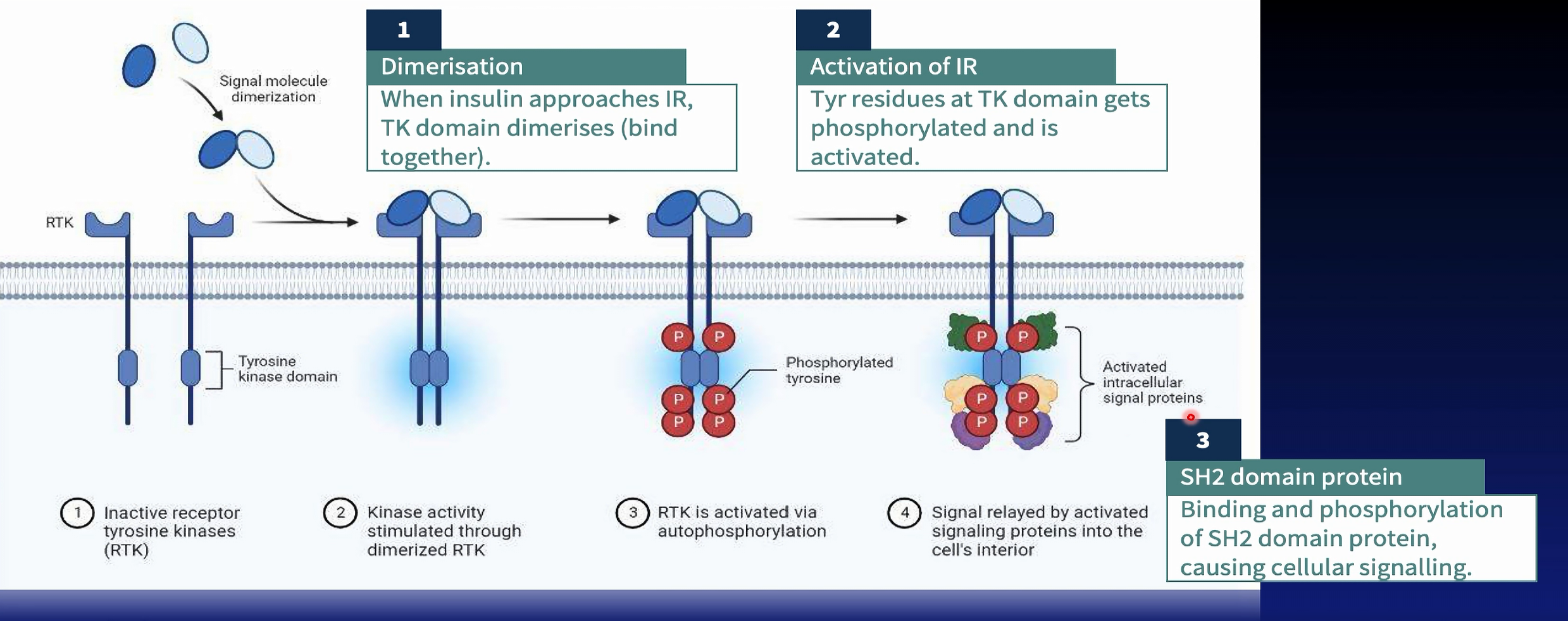
when activates by insulin → phosphorylation → cascading signals → glucose metabolism → lowers blood sugar
location: adipose tissue, hepatocytes, skeletal muscle
endogenous ligand → hormones released by beta cells of the pancreas
function: allows uptake for excess blood glucose from the bloodstream into the skeletal muscle to convert glucose in glycogen to reduce blood sugar.
EVEN IF patients do not feel better after taking the medication, they still have to continue the routine and use of the medication due to the delayed onset of action of the medication due to its nature.
Not all drugs will act on proteinaceous target → all the reactions are not on proteins.. but simply just chemical or direct reactions with other targets that might not necessarily be proteins
targeting RNA → directly acts/intercalates on DNA to prevent proper unwinding of template and non-template strands in tumorigenic cells to prevent formation of cells that cause bone sarcomas → this treats bone cancer (Doxorubicin)
Physical Interactions → directly absorbs toxins onto charcoal to expel it out of the body to remove causative factors
chemical interactions → antacids → neutralizes excessive hydrochloric acid to relieve gastric and heartburn or symptoms from GERD
Drug-Receptor Interactions
bioavailability and half-life of the drug affects how much drug will be present in the systemic circulation
Induced-fit model → 3D shape that interacts via intermolecular forces of attraction between drug and amino acid residue on the ligand-binding site of receptor. The ligand-binding domain adjusts to bind to substrate → ensure precise fit → receptors only bind with chemical structure of drugs that are closely related to the endogenous ligand that interacts with the ligand-binding domain
DR interactions are selective and specific. It only happens when it is exact → determines efficacy and potency.
types of non-covalent → ionic, hydrogen, dipole-dipole, pi-pi interactions and van der waals forces (highest → lowest)
how do we envision the structure and induced-fit?
structure-activity relationship → the structure is obtained via x-ray crystallography → qualitative and quantitative understanding of IMF → affects binding affinity
identify → functional group of the drug and the domain, physicochemical properties (size, shape and lipophilicity) and spatial arrangement (is the atoms filling the gap)
this is needed to create specific and selective drugs to only interact with that particular drug receptor
Two State Receptor Model → activated and inactivated state
both are reversible and work towards equilibrium
inactive receptor → constitutive receptor activity (receptors still have some activity at its baseline) → might not be enough to cover the body’s needs → drugs or endogenous ligands are still needed to either stimulate or inhibit the activity of the receptor.
if there is too little activation, equilibrium will push towards R* in order to activate the receptor’s activity/signals adequately (MCR)
eventually, endogenous ligands detach when adequate activity is going on.
Agonists and Antagonists
Parkison’s disease → clinical example (too little signal that results in the disease. There is a lack of dopamine signalling)
Hypertension → clinical example (too much signaling that results in the disease. There is too much signals to increase blood pressure in the body)
Binding Affinity, Efficacy and Potency
Binding Affinity → the tendency of a drug to bind to the receptor .
influenced by.. → formation of [DR] or detachment into [A] and [R]
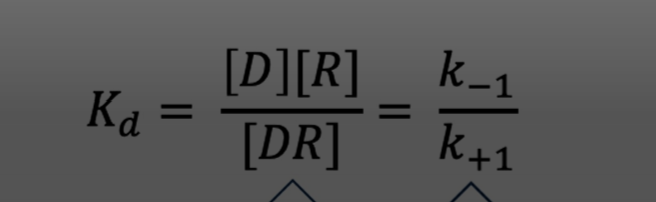
Dissociation constant [Kd}→ measures drug required to occupy 50% of receptors in the body.
Affinity is inversely proportion to Kd → if you need a high amount of drug to occupy 50% of receptors, it means that the affinity of the drug to the receptor is not very strong → meaning low drug-receptor affinity.
HOWEVER.. Affinity has little relevance in a clinical setting compared to a laboratory setting — affinity does not tell us what the drug can do.. hence measuring the level of therapeutic effect or the potency that a drug has is more important and clinically relevant than the affinity of the drug
Kd = concentration of free drug at half-maximal binding between [D] and [R] → 50% is bound, 50% will also be free.
Bmax → maximum binding possible between the drugs and receptors available in the body → this is why some drugs are or work “stronger/more potent” than others.
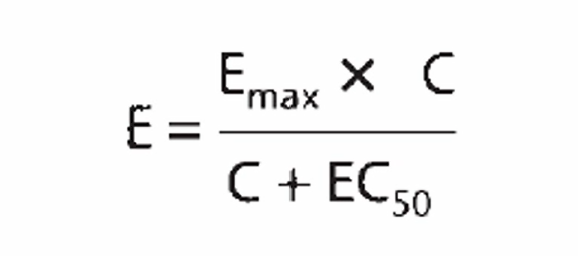
Potency → measures that drug’s biological effects in a person → instead of measuring formation of AR, we measure the response of the body towards the drug.
Antagonist → when there is TOO MUCH signaling, use this to reduce of prevent activation/stimulation of signals → inhibitory concentration 50
Agonist → used when there is TOO LITTLE signaling, use this to increase the activation/stimulation of signals → effective concentration 50
affinity measures that efficacy of the drug from the receptor perspective (how well do you bind) while potency measures efficacy of the drug from the organ system perspective.
potency allows us to have a baseline comparison between potencies of different drug with similar biological effects
Efficacy → the tendency of the drug to activate the receptor to alter the biological response of the body → applies to agonistic drugs. [the part where, whether AR causes a response]
Emax → measures the tendency to activate receptors to alter biological response.
Antagonist → have zero efficacy to measure → efficacy-zero
Efficacy → obtainable by direct reference to dose-response curve
The Outcome of [DR] Interactions.
agonists → binds and activates the receptor to cause/elicit tissue response → intrinsic activity that induces biological effect of the same or higher level than the endogenous ligand
Types of agonists
full → maximum
partial → increase 50%
inverse → brings it “down”
Depression → lack of adrenaline, dopamine and serotonin → 5HT-1A receptor in the post-synaptic neuron → serotonin is release by the pre-synaptic to regulate mood, focus and emotions
Location → hypothalamus, hippocampus, amygdala, spleen and kidney
serotonin → emotional stability, focus, happiness and calamity
function → control cognitive function, mood and emotional states → lack of it causes low mood, insomnia, apathy, sadness.
people with depression have lower activation of 5-HT → causing low mood etc..
treatment: Gepirone → mimics 5-HT to surge and bring up activation to 100% (full agonist)
treatment: Buspirone → doesn’t surge it up all the way to 100% but rather 75% (partial)
treatment: Inverse Agonist → reduces the activity (there is no such treatment → doesn’t make sense to have it
prozac is different from all of this → instead of increasing the activation using drugs → it increases the production of serotonin neurotransmitters.
Spare Receptor Theory → the initial theory was that in order to get 100% surge, you need to bind to ALL receptors, but it was proven to be wrong.
full → you don’t need 100% occupancy of receptors to achieve an increase to 100% activation → in reality you only need around 30% occupancy to reach it (e.g.) → number of receptors in the body is actually MORE THAN ENOUGH to induce maximum response → the drug is able to elicit 100% response as it has high enough intrinsic activity.
partial → 100% occupancy of receptors, doesn’t necessarily give you the maximum response → due to limited intrinsic activity by the drug.
competitive antagonism → reduces occupancy of agonist, lowering formation of DagonistR and activating it → if we increase the agonist, it can overcome competitive antagonism at high concentration to go over the blockade.
dose response curve will shift to the right if this happens → dose of the agonist has to increase, but the % increase of the response will remain the same → this is applicable when people are on many medications (promiscuous antagonists) and activate the spare receptors → you will have mixture of effect on the molecular level → this pulls the curve down potentially.
effect of the antagonist on the agonist → the efficacy doesn’t change (Emax) → competition is overcome
HOWEVER → potency will decrease → more drug (agonist) is needed to elicit the same effect of the increase up to 100% in biological response
Non-competitive Antagonism → binds to the allosteric site of the receptor → changes the 3D shape of the active site → irreversible or nearly irreversible due to formation of covalent bonds between antagonist and allosteric site.
dose response curve → the graph is shifts to the right and then it has a lower maximum efficacy
efficacy → lesser [DR] complex = lesser [DR*] → Maximum Biological Response/Activity is attenuated/lowered
potency → irreversible change to ligand-binding site , More [D] still needed, hence potency decreases drastically.
pharmacodynamic drug interaction → many drugs’ activity might interact with each other and limit each others’ effect.