Immunology Take home questions
Animals often present with wounds from a variety of circumstances

Are bacteria likely to contaminate these?
Yes
Which type of bacteria? extracellular or intracellular?
Extracellular most likely (intracellular bacteria live in cells so are unlikely to be part of a containment)
Outline how the host system responds
consider cell types, cell products, timing, location of responses, cell migration, interaction between cells, etc
Acute inflation - increase blood supply, activate vasculature, proinflammatory cytokines (IL-6, IL-1, IL-12, IL-23, TNF, etc)
Resident neutropihls and macs - recognize (PAMPs), kill, activates (by NK IFN-g and PAM recognition), make cytokines (IL-12, 23, TNF, etc)
complement - opsonize (C3b and C4b) and recruit (C3a and C5a)
Preexisting antibody may also opsonize
More neuts and macs recruited, and production initiated
DCs recognize via PAMPs and opsonins (C), travel to LN - look for a date with T cell and B cell.
Naive Ts circulating - find a match - stay in lymph node (surface markers change)
Replicate and move towards B cells zones to provide help
B cells concurrently start making IgM (good C fixer)
Produce appropriate cytokines (IFN-g) to promote isotype switch to opsonizing IgG
B cells undergo somatic hypermutation to optimize specificity of response - switch from IgM to IgG (C fix and opsonize)
Ts and antibody to site of infection (activated vasculature) - IFNg for mac activation, ab to opsonize (neutralize at mucosal sites), IL-17 for neut recruitment and activation
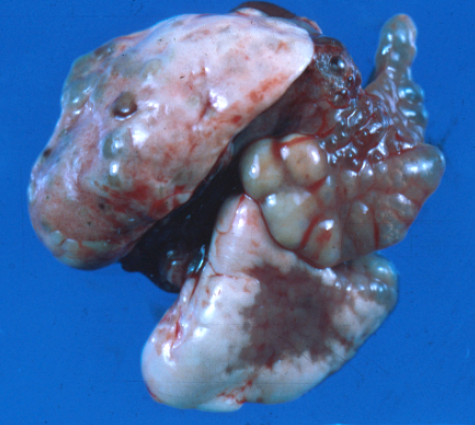
What is your presumptive diagnosis
 Abscess
AbscessDid the immune system work in this case? why or why not?
The immune system did work in the sense that all of the steps in thelast slide, happened, the recruited neutrophils are doing their hardest to kill the bacteria, antibody is opsonizeing, etc. The body also “walled” off this infection to prevent spread and damage systemically.
In some cases, these may resolve on their own, but not always, so in the latter case, one might conclude that it didn’t work completely.
We would want to intervene with lancing, cleaning, antibiotics, etc
What diagnostics would you perform to confirm, what would you expect to see and how does this fit with our discussion of the immune response to extracellular bacteria?
several options to include 1) lancing which reveals pus, 2) smear of aspirate that would show neutrophils and maybe bacteria, 3) CBC which might show elevations in neutrophil numbers and 4) culture
Remember the first line of defense against extracellular bacteria are neutrophils and plenty have been recruited to this abscess. What we don’t see is all of the action in the regional lymph node that is helping with this recruitment and defense
How would you treat this?
lance, clean, antibiotics, follow-up
When you see neutrophils, think extracellular bacteria first
The cat owner asks about a lump under the chin, and you wow them with your description of the immune system dating game and how that mass represents a reactive lymph node. Howevery, they have a relative with lymphoma and remain concerned, so you aspirate the node, you see this - what are the cells at the arrows and why are they there?
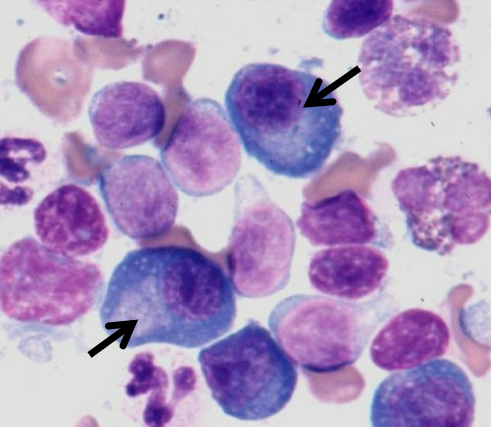
Plasma cells! The DC/T cell dating is ongoing
T cells that find a match hang out and proliferate - then help B cells that are specific for that antigen proliferate and ultimately become plasma cells (antibody factories) that are characterized by large golgi apparatuses (the light blue areas adjacent to the eccentric nuclei). The golgi is where the antibody chains are carboxylated and linked together.
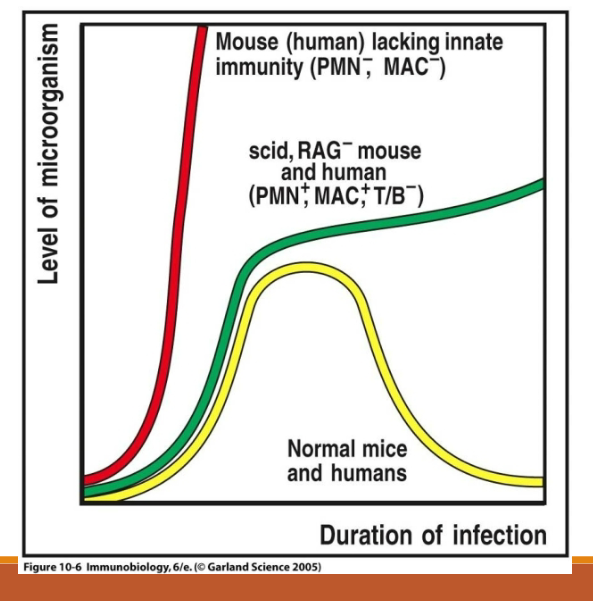
Which of the following would you expect to be MOST susceptible to extracellular bacterial infections and why?
Animals deficient in neutrophil function
Animals deficient in T cells
Animals deficient in B cells
Animals deficient in macrophage activation
All of these animals would likely to be more susceptible to extracellular bacteria, but those with defects in innate immunity (neutrophils and macrophages) would likely to be most susceptible)
A nude mouse is deficient in T cells; why might it be more susceptible to staphylococcal infections?
Most penetrating wounds, even if contaminated don’t result in abscesses.
Cat bites are notorious for causing abscesses due to the presence of certain bacteria (pasturella multocida) in the oral cavity - bacteria have nice immune evasion mechanisms that allow them to colonize and cause disease. Staphylococcus aureus is a common skin inhabitant that normally doesn’t cause disease.
This is a nude mouse that has no T cells. Therefore it cannot provide B cell help.
As a result, no T cell dependent antibodies are produced (there still may be some T cell independent antibody production) which are important in opsonization of encapsulated bacteria like Staph.
These mice are therefore very susceptible to staphylococcal furunculosis (abscesses of the hair follicles.
_____________________________________________________________________________________
Class 3: immune response to microbes take home questions
How does the response to intracellular bacteria differ from that which occurs against extracellular bacteria?
same for intracellular vs extracellular fungi?
With IC bacteria, humoral immunity is less effective because it can’t get into the cells.
IF IC bacteria escape into the cytoplasm, CD8+ cells become an important adaptive immune component
Macrophage activation important in both
Neutrophils (and Th17 cells/IL-17 ) important in both, but especially EC bacteria and fungi
What does AIDS (lack primarily of CD4+ T cells) tell us about susceptibility to extracellular vs. intracellular bacteria?
AIDs patients are particularly susceptible to IC bacteria (although both can occur)
Highlights need for T cell help in activating macrophages and highlights how well the innate system works against EC bacteria
You are presented with a 4 yo heifer that died following a prolonged period of wasting and chronic diarrhea. On necropsy you find a thickened ileal wall. Being a closet pathologist, you get your own histology sections prepared and see marked mucosal granulomatous (dominated by macrophages) inflammation.
What type of infection do you suspect?
What additional stains do you perform?
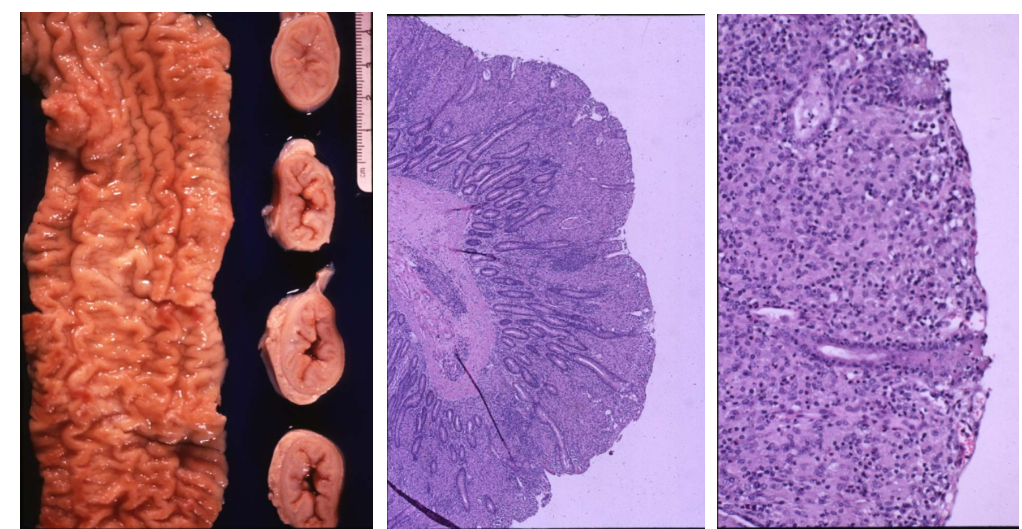
When macrophages dominate an inflammatory infiltrate, think fungus or mycobacterium sp., an intracellular bacterium.
This macrophage-based response is typically Th1; if Th2 occurs, bacteria may replicate uncontrolled. You can stain histologic sections using fungal stains and stains for mycobacterium (an acid fast for the latter).
You are presented with a MIssouri dog with clinical signs of pneumonia
On radiographs you note multiple tiny masses in the lungs.
On cytologic preps of lungs, you note a number of macrophages including giant cells.
What types of pathogens make it onto your differential diagnosis list?
What further diagnostics can you do
Lung biopsies or necropsy if the dog succumbs might show granulomatous or pyogranulomas (macs + neuts) with giant cells - again, if you see macrophages, think mycobacterium and fungi - giant cells can occur as well.
You can again stain sections to look for either.
if this is a dog is in Missouri, think fungal diseases like blastomycosis or histoplasmosis
Which of the following would you expect to be MOST susceptible to fungal and intracellular bacterial infections and why?
Animals deficient in macrophage activation
Animals with macrophage defects would most likely be susceptible, but defects in T cell help (AIDs patients) could also render animals susceptible.
B cells least likely but still possible.
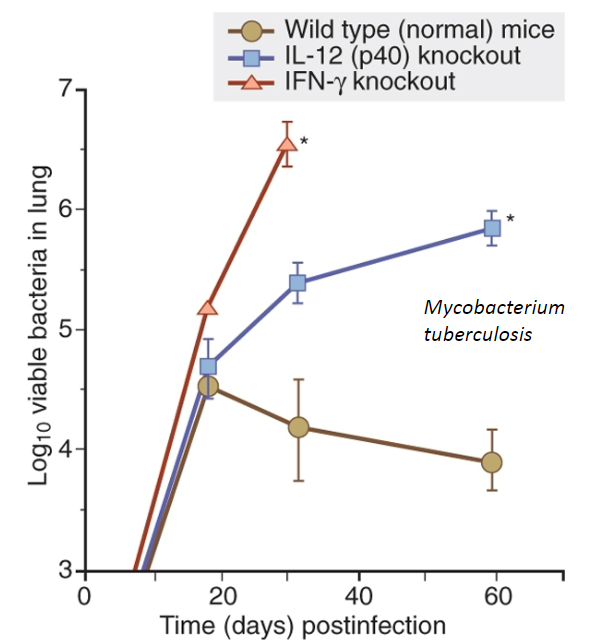 6. Outline how the host immune system responds to an intracellular infection
6. Outline how the host immune system responds to an intracellular infection This one is more complicated in that it depends on factors such as what cell the bacteria occupies and what part of the cell (livesin phagosome, phagolysosome, cytoplasm)
Know that bacteria like mycobacterium have evolved mechanisms to live in phagocytes like macrophages. The phagocytes respond to this infection by becoming activated through receptor recognition and cytokines like IFN g (sources include NK cells early and Th1 cells later).
Activation of macrophages may allow for some killing but bacteria are not eliminated.
Macrophages may proliferate which is somewhat paradoxical in that it provides more homes for the bacteria (but its better than nothing).
DCs may take up antigens from dead cells or bacteria and present to T cells which polarize to Th1 and produce IFNg to help macrophages.
T cells may help B cells to make antibody, but the latter is not super important because it can’t get into the cell (it may help with bacteria that are transiently outside of the cell) activation. Similarly, complement may not be as effective as it is for extracellular bacteria.
For intracellular bacteria that live in the cytoplasm (listeria the example in class), their antigens may be presented to T cells in the context of MHC 1 which results in the production of cytotoxic T cells that can then kill infected cells.
The macrophage activation component described for mycobacterium is also ongoing in the disease.
This dog suffered from severe burns - what part of the immune system is now severely impaired?
Burn patients have lost one of the most important and often underappreciated components of the immune response: physical barrier
What physical defense may have failed in this infection?
 - Ciliary function - rat with chronic mycoplasma (not mycobacterium) infection
- Ciliary function - rat with chronic mycoplasma (not mycobacterium) infection -immune system cannot eliminate mycoplasma colonize ciliated epithelium - rat attempts to eliminate by producing more mucus - bronchioles dilate and fill with mucus as cilia cannot push out bacteria
-end with bronchiectasis