Eyes and Ears
Health History
Which is part of the eye assessment?
Diagnostic positions test
PERRLA
Snellen
Assessment of the Eyes and Ears
If a client has a vision of 20/40, it means the client can see items clearly at 20 feet, which most people can see clearly at 40 feet.
The numerator (top number) indicates how far the client is standing from the chart. The denominator (bottom number) identifies the distance a normal, average eye could have read that same line.
Equipment
To look into a client’s ear, the nurse would use an otoscope.
An ophthalmoscope is used to look into the eyes.
The Health History
The health history collects subjective data about the individual’s medical history, lifestyle choices that may impact the health of both the eyes and ears, and knowledge deficits to address with health education.
The nurse uses data collected from the health history to determine the focus and depth of assessment of each system.
Eyes:
Ask about:
vision difficulty, including decreased acuity, blurring, and blind spots
eye pain, burning, or itching
strabismus or diplopia
redness or swelling
watering or discharge
history of ocular problems
glaucoma
use of glasses or contact lenses
medications, systemic or topical
history of smoking
vision loss
date of last eye exam
Ears:
Ask about:
earaches and ear infections
discharge from the ears
hearing loss and environmental noise
tinnitus and vertigo
cleaning of the ears
Lifestyle
Interviewing the client regarding their lifestyle provides important data that will help the nurse assess the impact on eye and ear health. The information gathered during the interview will guide the nurse in providing the most relevant education and interventions.
Risk Factors
Risk factors for eye diseases and vision loss may include:
family history of eye disease
advancing age
untreated strabismus
frequent or unprotected ultraviolet light exposure
increased intraocular pressure (glaucoma)
lifestyle behaviors (e.g., smoking, alcohol use)
chronic diseases such as hypertension, diabetes mellitus, and renal dysfunction
Risk factors for hearing impairment may include:
genetic predisposition for hearing loss
loud environments (e.g., high volume music, factory work, gun use)
chronic ear infections
cerumen buildup
advancing age
Hearing Loss
Loud noises, cerumen buildup, and chronic infections can contribute to hearing loss.
Preparing to Assess
Tools needed to assess the eyes include:
Snellen eye chart
ophthalmoscope
opaque card or occluder
penlight
Tools needed to assess the ears include:
otoscope
Inspection: Eyes and Ears
When inspecting the eyes, ask yourself:
Are the eyes positioned appropriately within the socket without bulging?
Are the lids droopy?
Do the eyes follow or track your movements as you do your examination?
Does there appear to be enough moisture in the eye, or is there any drainage?
What is the color of the sclera (white) and conjunctiva (the pink area surrounding the eye)?
When inspecting the ears, ask yourself:
Is the size and shape of the auricle symmetrical?
What is the ear position and alignment on the head?
What is the skin condition (including color and any lumps or lesions)?
Are there any hearing devices, such as a hearing aid?
Is there any ear drainage or odor?
Does the client have any piercings, discs, or tattoos?
Parts of the Eye
The pupil is at the center of the eye, surrounded by the iris. The white space around the iris is called the sclera.

Parts of the eye: pupil, sclera, iris
Eye Assessments: Inspection and Testing
Inspection:
The sclera (the area surrounding the iris) should be white. Erythema or jaundice could indicate other health issues. The conjunctiva, which is the mucus membranes on the inner portion of the eyelid, should be pink and moist. Pale conjunctiva could indicate anemia, and erythematous conjunctiva could indicate infection.
PERRLA:
You will use the mnemonic PERRLA when completing the eye assessment. Pupils are generally the same size, but slight variations in size, up to 1 mm, may be normal. The pupils should be round and change in size when exposed to light or when focus changes to an object that is nearer or farther.
Review the video to understand the PERRLA mnemonic.
P: Pupils are equal in size
E: Pupils are round
R: React to light, constricting when exposed
R: React to accommodation, changing size when focusing on near and far objects
L: Light reflex is present
A: Accommodation is intact, allowing for smooth transition between distances.
Pupil Gauge:
A pupil gauge measures the size of the pupil in millimeters. The normal pupil diameter is 3, 4, or 5 mm.
Miosis is pupils smaller than 2 mm or pupils that do not dilate when light is removed.
Mydriasis is pupils that are 6 mm or larger or pupils that do not constrict when light is applied.
Visual Acuity
Do you remember being in school and having to have an eye exam? They would make you put a spoon or other device over one eye and read letters of various sizes on a chart.
The school nurse was assessing your vision acuity using a Snellen chart. Normal vision is 20/20, which means you can see objects clearly from 20 feet away.
So, what does it mean if you have 20/30 vision? This means that you can see items clearly at 20 feet, which most people can see clearly at 30 feet. So, in essence, the higher the second number, the worse the vision. However, if you have 20/10 vision, you can see at 20 feet what most people see at 10 feet.
The use of the ophthalmoscope is an advanced technique.
Pupil Size
Which pupil diameters are considered normal?
Normally, the resting size of a pupil is 3, 4, or 5 mm. The size of the pupil decreases in response to light and increases in response to darkness.
If the pupil is outside this range, the nurse should investigate further.
Inspection and Palpation: Ears
To examine the ears, the only tool needed is an otoscope, which is used to examine the ear canal and tympanic membrane (ear drum). Assessment of the ears includes inspection, palpation, use of the otoscope to visualize within the auditory canal, and testing.
Inspection:
Start the ear assessment with inspection and look for:
symmetry
general size and shape (malformations of the ear can indicate renal problems)
redness or discharge from the ear
piercings, wounds, nodules, or lesions (the ears can be a commonly missed location of skin cancer, or nodules known as tophi may indicate renal impairment)
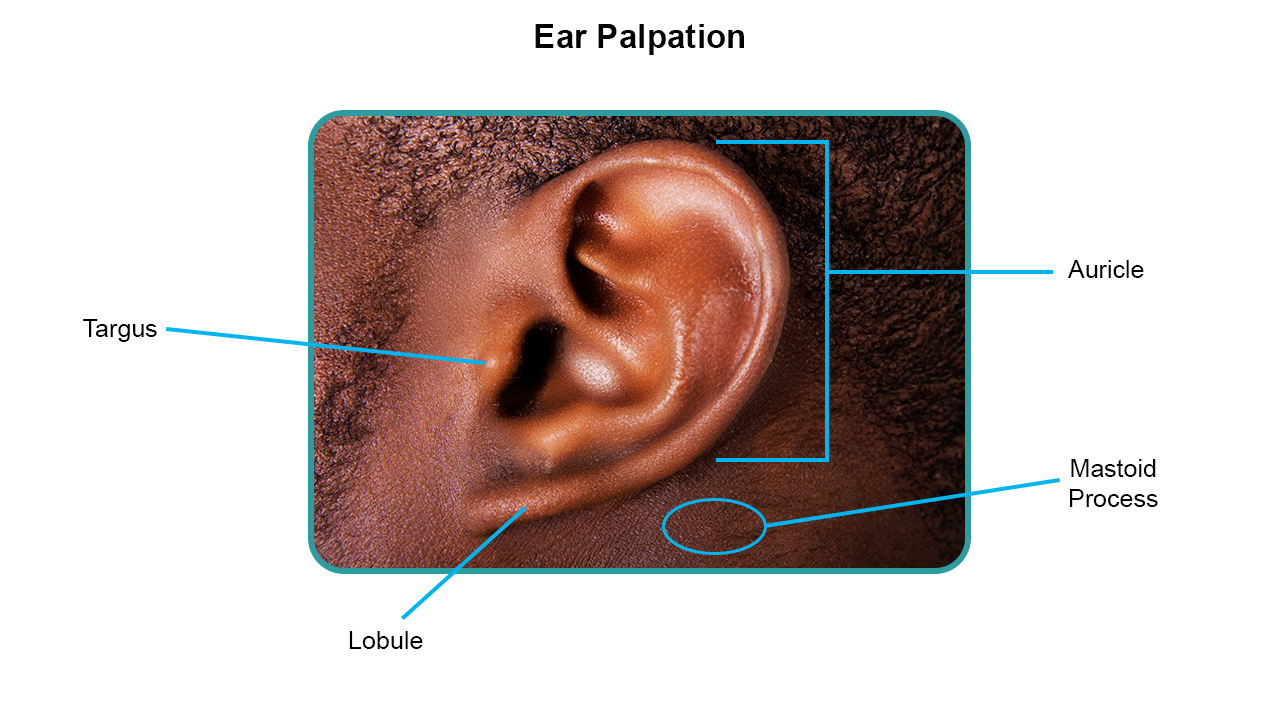
Palpation:
Palpate both ears for tenderness in each of the following locations:
auricle
lobe
tragus
mastoid process
Otoscope:
Looking into the ear canal with an otoscope will allow you to visualize the external auditory canal, cerumen (if any), the tympanic membrane, and two of the ossicles of the ear. Remember to pull the pinna up and back for adults and pull it down for children under the age of 3.
Assessment with the otoscope includes:
presence of occlusion (cerumen buildup, bony growths, or foreign objects)
color, integrity, and transparency of the tympanic membrane (expect pearly gray, translucent, and intact)
identify erythema (redness), discharge, or other signs of inflammation
Auditory Acuity
If the client has current hearing loss, audiometric testing should be done. If not, then perform the whispered voice test and tuning fork tests. Select each tab to review information on these tests. The techniques are also described in your textbook.
Whispered Voice Test
The whispered voice test is used to detect high-tone loss. Stand about 2 feet behind the client. To test one ear at a time, instruct the client to place one finger on the tragus, pushing it in the auditory meatus to occlude sound. Move your head 1 to 2 feet from the person's ear. Slowly whisper three random numbers and letters, such as “3, S, L.” Ask the client to repeat each number/letter correctly after you say it. A passing score is the correct repetition of 4 of 6 numbers/letters.
Tuning Fork Tests
Tuning fork tests can help the nurse identify if the client has conductive hearing loss or sensorineural hearing loss.
The Rinne test assesses air conduction to bone conduction (AC:BC). Air conduction should be about twice as long as bone conduction of sound. A normal finding for the Rinne would be documented as AC>BC at 2:1. An abnormal Rinne test would require additional testing to confirm.
The Weber test should demonstrate that sound is heard equally in both ears when a vibrating tuning fork is placed in the center of the top of the head. An abnormal test would demonstrate that the sound is louder in one ear. In conductive hearing loss, the sound would be louder in the “poorer” ear. With sensorineural hearing loss, the sound would be louder in the unaffected ear.
Pinna Position
When looking into the ear canal with an otoscope, remember to pull the pinna up and back for adults and pull it down for infants and children under the age of 3. This will straighten out the ear canal and allow for visualization of the tympanic membrane.
Developmental Influences: Eye
The health of the eyes is influenced by multiple factors, including the process of aging. Review the information for details about age-related eye health.
Infants and Children
The eyes should be examined within a few days after birth and at every well-child visit thereafter.
The child's age determines the screening measures used.
At birth, eye function is limited but matures fully during the early years. Peripheral vision is intact in the newborn infant.
By 3–4 months of age, the infant establishes binocularity and can fixate on a single image with both eyes simultaneously.
The Aging Adult
Central acuity and peripheral vision may be diminished.
Changes in eye structure can cause distinct facial changes in the aging person. Loss of skin elasticity causes wrinkling and drooping; fat tissue and muscle atrophy also have an impact.
Lacrimal glands involute, causing decreased tear production and a feeling of dryness and burning.
In older adults, the most common causes of decreased visual functioning are:
cataract formation
glaucoma
age-related macular degeneration
diabetic retinopathy
Developmental Influences: Ear
The health of the ears is influenced by multiple factors, including the process of aging. Review the information for details about age-related ear health.
Infants and Children
Examination of the external ear is similar to that described for the adult. Determine if ear tubes have been placed prior to the assessment.
During the otoscope examination, remember that for ages less than 3, pull the pinna straight down; for children older than 3, pull the pinna up and back.
Use developmental milestones located in your text to assess the hearing of the infant.
The Aging Adult
An aging adult may have pendulous earlobes with linear wrinkling because of the loss of elasticity of the pinna.
The cilia lining of the ear canal becomes coarse and stiff, which may cause cerumen to accumulate and oxidize, which may greatly reduce hearing.
Developmental Changes With Aging
Which is a common age-related change in the ears? Coarse and stiff cilia
The correct answer is coarse and stiff cilia.
An aging adult may have pendulous earlobes with linear wrinkling because of the loss of elasticity of the pinna. The cilia lining of the ear canal becomes coarse and stiff, which may cause cerumen to accumulate and oxidize, which may greatly reduce hearing.
Abnormal Findings (Eyes and Ears)
Though most assessments of the eyes and ears lead to normal findings, the nurse needs to understand and recognize abnormal findings.
Abnormal findings of the eye include:
extraocular muscle dysfunction
external structure abnormalities
eyelid lesions
pupil abnormalities
visual field loss
vascular disorders
internal structure abnormalities
Abnormal findings of the ear include:
external structure abnormalities
hearing loss
ear lesions
internal structure abnormalities
Health Education
Data collected during the assessment of the eyes and ears provides information the nurse can use to help clients maintain or improve their health
Health Education (Eye)
Loss of eyesight can impact client independence, so quick and timely intervention is essential when changes are detected.
Education of proper care and protection of the eyes includes but is not limited to:
use of appropriate safety eyewear for sports and occupation
use of appropriate eyewear for sun exposure
annual eye visits to assess vision and age-related changes
reporting of changes to vision and eye function as soon as possible
Health Education (Ear)
Noise-induced hearing loss is usually permanent and progresses with each exposure. Client education should include:
use of proper ear protection when working around loud noises
never put foreign objects in the ear
do not use cotton swabs to probe or clean the ear canals
do not put cotton balls or liquids into the ear unless prescribed by a provider
treat ear infections as soon as possible
Hearing loss may be prevented by prompt treatment. When hearing loss is treated early, one may be able to prevent or delay problems. Impaired hearing may contribute to depression, social isolation, and loss of independence and has been associated with cognitive decline.
Documentation: Eye Assessment
Progress notes and Electronic records
It is essential to perform a thorough eye assessment during regular check-ups to identify issues such as refractive errors, cataracts, or glaucoma, which may require intervention.
Documentation: Ear Assessment
Progress notes and Electronic records
No signs of infection, inflammation, or drainage observed.
Tympanic membranes are intact and pearly gray, and there is no evidence of fluid behind the eardrum.
Patient denies any pain or discomfort in the ears.
Recognizing Cues
The client in the picture has an abnormality of which eye structure?

Older adult male with anisocoria
The client has abnormal pupils (anisocoria). Pupils should be approximately equal in size.
In low light, it is expected that both pupils are dilated to allow more light to enter the eye. In bright light, both pupils should be constricted to prevent too much light from entering the eye.
Analyzing Cues
What potential issues might the client have based on the assessment of their eyes? Select all that apply.
Older adult male with anisocoria
Other than physically looking out of proportion, the difference in pupil size (anisocoria) might affect the client’s vision. If one pupil cannot adjust to light like it usually does, the client might have trouble seeing clearly. The client might also experience pain due to the inability to prevent excess light from entering the eye. It is important to assess the cause of the pupil change. A dilated pupil on one side can also be a symptom of a neurological problem (swelling in the brain).
The cornea color will not change with pupil dilation; the pinna is part of the ear. Tinnitus is a ringing in the ears.
Prioritizing Hypotheses
What should the nurse address first?
Older adult male with anisocoria
The priority assessment is the pupil size differences (anisocoria), as this is not a normal finding in an eye assessment, and it may indicate a brain injury or serious eye disorders that could result in blindness.
The nurse may do a vision test to assess for vision changes, but the pupil size difference is the priority assessment.
With aging, a loss of skin elasticity causes wrinkling and drooping; fat tissue and muscle atrophy also may occur. These are normal findings in an older adult and not a priority assessment.
Planning Care: Generating Solutions
To assess for pupil accommodation, the nurse would expect to support the healthcare provider in which interventions? With each potential intervention, check if it is indicated or not indicated for the client.
Assessing pupil dilation using a penlight is indicated for this client, who has different pupil sizes, as pupil accommodation usually changes with the light.
An otoscope is used to examine the ear canal and is not indicated for an eye exam. The Rinne test is a hearing test and is not indicated for an eye exam.
Take Action
What is the top priority when caring for a client with unequal pupils?
The top priority is to assess for eye injury.
Reviewing medication can be done after the eye assessment. Some medications can cause pupils to be of different sizes. Eye drops are not usually ordered in the treatment of different-sized pupils and would not be the priority action. Tinnitus is a ringing in the ears.
Evaluate Outcomes
It is determined that the client has physiological anisocoria, a pupil size difference based on physiology (naturally different sizes). Select the assessment findings that indicate a physiological cause of pupil size difference and those that indicate a non-physiological cause.
Physiological anisocoria is when the pupils are naturally different in size. It is the most common type of anisocoria. The vision is unchanged from baseline, and the client’s confirmation of being “born this way” would indicate this as physiological.
Pathological changes include disease processes and injuries that have altered normal functioning. A head injury and neurological conditions that caused unequal pupil sizes would be considered pathological.
Education
The nurse is educating the client on ear care. Which statements from the client regarding ear care indicate understanding?
“Ear infections should be treated right away.”
“I should wear proper ear protection when working around loud noises.”
“I should not put any foreign objects in my ear canal.”
Client education should include:
Use proper ear protection when working around loud noises. Limiting time around loud noises is recommended, and always with ear protection.
Never put foreign objects in the ear.
Do not use cotton swabs to probe or clean the ear canals.
Do not put cotton balls or liquids into the ear unless prescribed by a doctor.
Treat ear infections as soon as possible.
The client should not use a cotton swab to clean their ears or expose themselves to loud noises (even temporarily) without ear protection.
Pupil Accommodation
The nurse is assessing for pupil accommodation in an adult client. The nurse would instruct the client to do which of the following?
Have the client focus on a distant object and then instruct them to shift their gaze to a near object.
Accommodation is the ability of the eye to change focus from near to distant and distant to near objects. It is tested by having the client focus on a distant object and then instructing them to shift their gaze to a near object.
The other tests do not assess for pupil accommodation.