Fluoride CDH
3 conditions in order for caries to form:
Susceptible Host- Teeth, Xerostomia, Lack of Fluoride
Bacteria- Primarily Streptococcus mutans, then lactobaccillus
Diet- Primary Sucrose
To Reduce Decay, make an effort
Increase resistance of teeth- fluoride
Reducing Bacteria by mechanical means
Diet modification
Mechanisms of Action
Partial replacement of hydroxyapatite with fluorapatite
Fluorapatite crystals are larger, more perfect, LESS Soluble
Calcium, Phosphate, and fluoride are needed for crystal re-growth
Bacterial Metabolisms reduced
Bactericidal (high conc. and low pH of fluoride)
Bacteriostatic (low concentration)
Fluoride alters ability of S. mutans to produce caries-causing acid
Remineralization- low conc, used daily
fluoride increases remineal. and decreases demineral (these areas soak up more)
Remineralized areas are stronger than regular enamel
Other agents that help remineral: ACP and MI paste (minimal intervention) Has recaldent to help with remineralization, white spot lesions, sensitivity. One study found no significant differences w helping WSL from ortho between varnish, MI paste compared to standard OH with regular toothpaste
Modification of tooth morphology
- teeth have slightly smaller, more shallow fissures (systemic fluoride)
Increased rate of post-eruptive maturation
- Newly erupted teeth have hypomineralized areas. Fluoride helps accelerate maturation.
Effects of Water fluoridation:
Perm teeth: 27% caries reduct.
Prim teeth: 40% caries reduct.
Mixed (8-12yrs): 20-40% caries reduct.
Smooth Surface: 86% reduct.
Occlusal Surfaces: 37% reduct.
Root Caries: 50% reduct (from topical effect of water fluoridation)
95% few caries in max ant. teeth
75% fewer permanent 1st molars extracted
less malocclusion
the chance for kids never having a cavity in their permanent teeth is abt 6x greater in the fluo. community than a fluo. deficient one
Adults benefit too: lower DMFT scores, less cemental caries, possibly fewer bone fractures
Research has established that:
body has an efficient excretory mechanism for fluoride (ppl on renal dialysis should not have fluoridated water water)
no skeletal damage from f. water
no impairment of general health at .8ppm
caries inhibitory effects well documented
.7ppm f.water for all climates!
Compounds used to fluoridate water:
Sodium Silica fluoride, Sodium fluoride, fluosilicic acid
Outermost layer of enamel has the highest concentration of fluoride in enamel
- Topical Fluoride is more effective soon after tooth eruption
Pulpal surface of dentin has the Highest Concentration of fluoride in dentin (From systemic)
UPTAKE:
- depends on the level of fluoride in the oral environment and the length of time of exposure
- Hypomineralized Enamel absorbs fluoride in greater quantities than sounds enamel
Fluoride in Biofilm and Saliva
Saliva and biofilm are reservoirs for fluoride; saliva carries minerals available for remineralization when needed
Fluoride helps to inhibit demineralization when it is present at the crystal surface during an acid challenge
Fluoride enhances remineralization forming a condensed layer on the crystal surface, which attracts calcium and phosphate ions
High Concentrations of fluoride can interfere with the growth and metabolism of bacteria
Dental biofilm may contain 5-50ppm fluoride. Varies greatly and constantly changing
Fluoride Toxicity:
When ingested, 90-95% of fluoride is absorbed through the stomach
most common side effect is NAUSEA
CLD ( certain lethal dose ) is based on kilograms of body weight
Adulta: CLD is 5-10g of NaF at one time
Children CLD is .5-1g (500-1,000mg)
Depending on weight and size, safely tolerated dose (STD) is ¼ the CLD
Chronic long term: Bone fluorosis, skeletal damage, (4-8ppm over 20+ yrs) (osteosclerosis is mild form)
Fatal Lfuoride poisoninf: accidental ingestion from large quantities of fluoride, e,g, in insecticides
Fluoride in dental products can be potentially hazardous to kids
Acute toxic dose symptoms: nausea, vomiting, hypersalivation, abdominal pain, in severe cases : muscle cramping, bronchospasm, ventricular firbrilation and cardiac arrest. NOT HYPOTENSION OR CONSTIPATION
Tx of Fluoride Toxicity
Induce emesis
administer milk, antacids (fluoride- binding liquids)
Take to the hospital
Use mineral free water for kidney dialysis patients
Do not store large amounts of fluoride at home and keep out of reach of children
MAX AMOUNT OF DIETARY FLUORIDE SUPPLEMENTS DISPENSED AT 1 TIME : 264 mG NaF, 120mg fluoride ion)
Enamel Fluorosis
Enamel Hypocalcification resulting from ingestion of excessive fluoride ion content during enamel calcification
Flurosis from excessively fluoridated water (2ppm) may require water to be defluoridated
Well water may have fluoride
Home filtrations systems may remove fluoride
Daily ingestion in excess of .10mg of fluoride (from all dietary and non-dietary sources) per kilogram of body weight is generally accepted to cause fluorosis
*Typical ribbon of toothpaste- 1mg of fluoride, kids 4-6 may swallow up to 50%
Grade of Fluorosis
Questionable: a few white specks
Very Mild: Small, opaque, paper white areas involving less than 25% of the surface
Mild: White opacities more extensive, but don’t include more than 50% of the surface
Moderate: Distinct brown staining, the tooth is worn and hypoplastic. All enamel surfaces are affected and discrete or confluent pitting is present
Mild Enamel Fluorosis
in order for hydroxyapatite to become incorporated within enamel matrix it has to degrade, then it gets rid of by-products
Excessive fluoride interferes with this process; crystals can’t get incorporated, accounts for white fluorosed areas
Severe Enamel Fluorosis
Brittle, hypoplastic
Toxic damage to ameloblasts
Why not fluoridated water?
lack of education
apathy. political inexperience
Lack of $$$ for initial set-up
Antifluoridatinonists’ activity
Violation of personal freedom
Tips for promoting water fluoridation
work w known officials and leaders in the health and welfare, inclu. members of professional groups.
Assess the leaders’ initial knowledge of and attitudes’ toward fluoridation
Provide needed education subtly and slowly
Activities should be directed toward the decision making group, rather than toward the public in general
Methods of fluoride administration
a. Community Water Fluoridation- Most cost- effective method
b. Dietary fluoride Supplements- Tablets, drops, vitamin preps (Poly-Vi-Flor and Tri-vi- Flor)
Dosage based on concentration of fluoride given in water and age of child
Supplements are not given to pregnant women
baby exclusively breast-fed: .25mg fl supplement starting at 6 mons
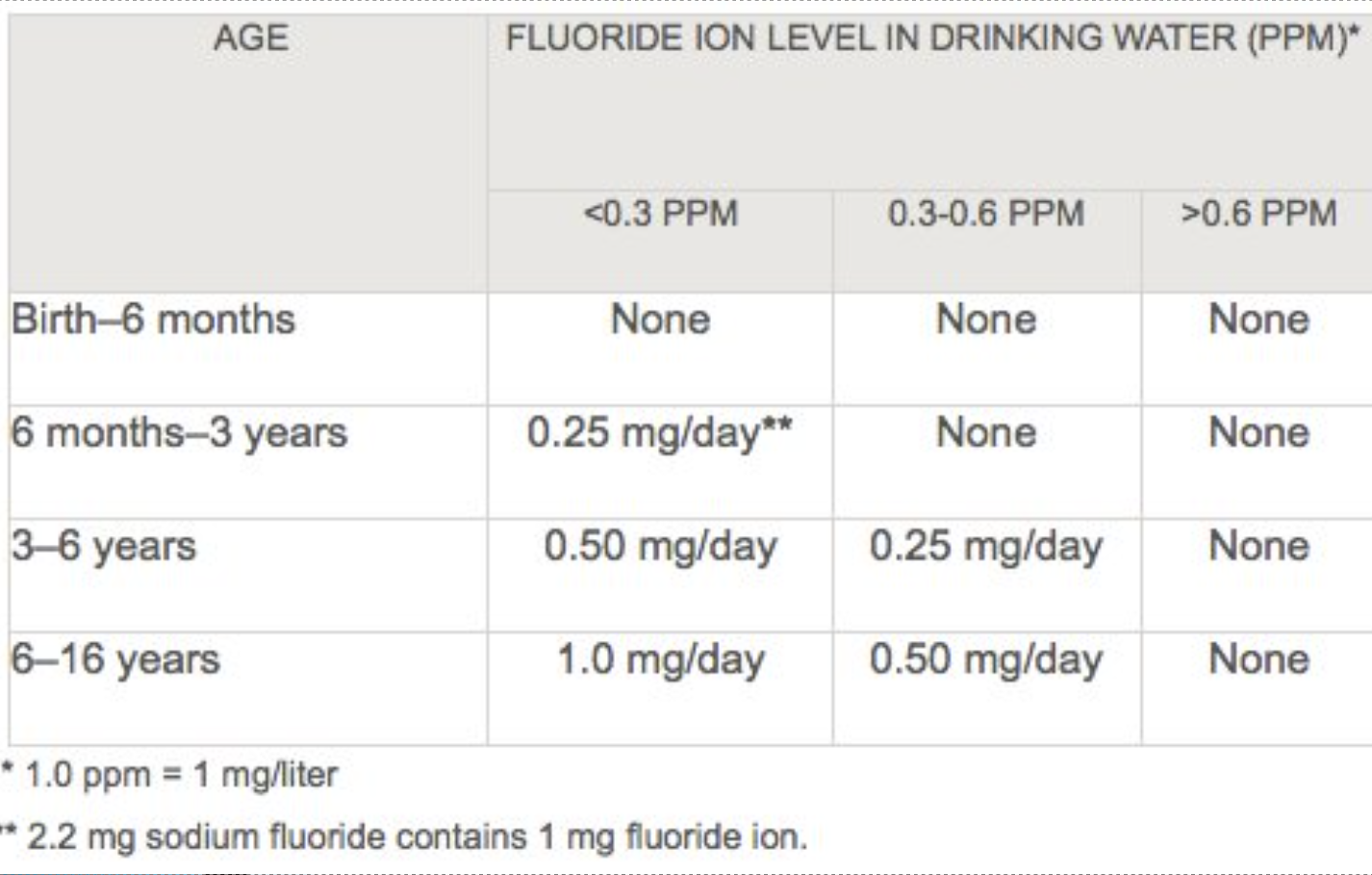
Fluoride Supplementation Chart
Birth - 6months: <0.3PPM, 0.3-0.6PPM, and >.6PPM — NONE
6mons - 3 yrs: <0.3PPM — .25mg/day ; .3- .6PPM, >.6PPM — NONE
3-6 yrs: <.3PPM — .50mg/day ; .3-.6 PPM — .25mmg/day ; >.6 PPM — NONE
6-16 yrs: <.3PPM — 1.0mg/day; .3-.6PPM — .50mg/day; >.6 PPM— NONE
School Based fluoride tablet programs
provide topical and systemic benefits; -30% caries reduction
inexpensive, requires little time; teachers can administer and the RDH can monitor the program
RX needed
Voluntary Participation
School Water Fluoridation
Fluoridated at 4.5 times that of community water
Disadvantage: children do not receive benefits until they begin school and while they’re in school
Caries reduction - 25%
Cost effective, but being replaced with fluoride mouthrinse programs for kids older than 6
Fluoride Mouthrinses
20%-50% caries reduction
NaF (sodium fluoride)
.2% used weekly (900ppm)
0.05% used daily (200ppm)
Not Rxed for kids under 6yrs
Rxed for pts with high caries susceptibility
.2% used for school-based weekly rinse program
low potency rinses available OTC
Rx for a non-fluoridated community: fluoride tablets K-8th grade; weekly fluoride rinses for grades 9-12
E. Profesional Gel Applications
Least cost effective as a public health measure
Neutral Sodium Fluoride (NaF)
2% concentration; pH 7.0; 9,040ppm
applied at 4 appt.s intervals (coinciding with eruption of teeth (3, 7, 10 and 13)
store in polyethylene container
Neutral Na Fluoride Cont’d
Good for sensitivity and pts with extensive restorations
must be applied for 4 mintues
“foams” appear to not be as effective
Thixotropic- materials are odd solids and fluids that change their viscosity when loaded by stress by becoming less viscous
Amounts in trays:
5ml for larger pt
2ml for small kids
Fluoride Varnish
24,000 ppm; 5% NaF or 2.26%F
FDA approved for desensitization but ADA endorses for caries control
helpful for kids at high risks for caries
less systemic absorption than gel trays
needs saliva to activate (unlike other fluroides, don’t need to dry teeth)
avoid hot, hard foods, alcohol, brushing, flossing 4-6 hrs after application
PROF. application 2x yr or every 3 months for pts. with high risk of caries NOT FOR HOME USE
Stannous Fluoride (SnF2)
8% or 10% concentration require single application; 19,300ppm
disadvantages: short shelf life; bitter taste; staining of teeth, silicates, decalcified and carious areas; gingivsl rxns; stannous ions cause atifacts on films if given prior to radiographs
Bacteriostatic- 1.64% used for subgingival irrigation
SnF2 is a good desensitizing agent
Acidulated Phosphate Fluoride (ADF)
1.23% orthophosphoric acid; 12,000 ppm pH of 3.5% (lower pH promotes uptake)
Store in polyethylene container
No clinical support for 1 minute gel of foam
contraindicated for porcelain, sealants, composites, implants, pts with mucositis. Note: Newer micro-filled composites are not as sensitive to APF agents
Home Fluoride Gels (tray and brushing methods)
Agents 1.1 NaF ex: Prevident or Fluoridex 5,000 cream
0.4% SnF2 ex: Gelkam
0.5% APF
Target Population: Kids over 6yrs w rampant caries or high risk for caries; contraindicated for kids under 6
also for adults with high caries susceptibility; denitinal hypersensitivity; xerostomia; root caries; ortho appliances; overdentures; recurrent decay
Fluoride Dentifrices
1,000-1500ppm
Agents: NaF; Snf2: Na MFP (monofluorophosphate) NOT APF
recommended for all patients, but uses caution w kids younger than 6 (peasize) toddlers (thin film of paste)
20-30% caries reduction
Other weapons for caries control
nanosilver rinse by elementa
Loloz with cavibloc
Xylitol products
Acp Amorphous, Calcoum Phosphate
Recaldent (in MI paste, Trident gum) ** derived from milk protein and should not be given to pts with a milk allergy
Basic Bites dental chews- designed to mimic saliva; arginine bicarbonate, calcium carbonate, xylitol ** offers options for those folks who oppose fluoride for whatever reason
Other therapeutic effects for plaque control
plaque inhibiting agents
chlorhexidine- .12% bacteriocidal; alters taste, stain, more calc, mucositits, inactivated by SLS, contains alcohol, Rx: rinse ½ ozfor 30 sec 2x daily (12hr substantivity) Can be used for caries control- High risk pts.
phenolic- related essential oils rinse (listerine)
sanguinarine (viadent) rinse and dentifrice
cetylpyridium chloride (scope, prohealth, cepacol)
glycine and erythritol powder- periodontal air polishing
Desensitising Agents
Fluoride! ( stannous is good for sensitivity) MOA: occludes dentinal tubules
Potassium Salts (potassium nirate, oxalate, chloride and citrate)
[ Sensodyne; Crest Hypersensitivity] MOA: Reduce depolarization of nerve membrane
Strontium chloride: pt ed: plaque control dietary issues, avoid tartar control dentifrices
Professional desensitization
dentin bloc agents prior to instrumentation: rubber cup polishing with desentizing agent( colgate sensitive pro-relief, sensodyne or novamin technology)
5% NaF Varnish application os sensitive areas at end of tx ( off label use as an anti-caries agent)
SDF
SDF (38%)-2014 approved for tx of dentinal hypersensitivity
SDF off label use for caries: silver (antimicrobial), Fluoride, and ammonia; arrests enamel, dentinal, and root caries
Dry tooth, apply for 1min, apply varnish to rest of mouth
Some studies suggest a 2nd application a week after inital application (1x wk for 3 wks)
applied every 6months for 2-3 yrs, 10 yr success and arrest rate for 90%
SDF plus potassium iodide solution (riva star)
Calculus Reducing Agents
Tartar control dentifrices
Sodium pyrophosphate salts
Sodium hexametaphophostae helps reduce new stain and calc formation
zinc salts
Whitening agent
OTC dentifrices claim whitening for removal of stained biofilm
some OTC dentifrices have a mild peroxide agent
carbamide peroxide (10%-22%)
Hydrogen peroxide (5-5%- 7.5%)
Hypersensitivity issues
“Bleachorexia”
Pit and Fissure sealants
Popularity in dental public health
mechanical barriers
need to be reapplied like fluoride
sealant tx can resutl in incipient caries reversal
37-50% phosphoric acid create mechanical tags or microspores
success depends upon dry field
Triage for sealing teeth
right after fully erupted
teeth w deep occlusal surfaces
6yr molars and 12 yr molars (1st grade and 7th grade)
Caries Risk!
Low SES
Past Caries or caries experience of mother, caregiver, or other sibs
low fluoride exposure
dietary factors: sugary foods or drinks; eating disorders— older kids
special health care needs
dental home (est. pt of record in a dental office)
visible plaque
Dental/ ortho appliances
salivary flow/ meds that result in xerostomia or caries
clinical or radiographic caries
restroations
unusual tooth morphology
low oral pH
High Microbial Count
CAMBRA- caries management by risk assessment
Rx 5,000 ppm cream: rxed for adults and children 12yrs of age older. Children 12-16 brush 2x per day, expectorate and rinse (over age 16 and adults: do not rinse) ** fluroride rinses are NOT recommended for kids under 6 yrs of age
Supplemental dietary fluorides are indicated for kids at high caries risk living in areas of under-fluoridated drinking water
Reductions in caries for topical fluorides:
daily OTC toothpaste — 24%
daily RX (5,000 ppm) cream — 37%
daily fluoride rinse — 26%
semiannual professional gel — 21%
semiannual professional varnish —37%