Wk 4
Physio techniques in ICU intubated patients
positioning
manual hyperinflation and ventilator hyperinflation
strageties to improve serction movement
high flow nasal prongs
positioning
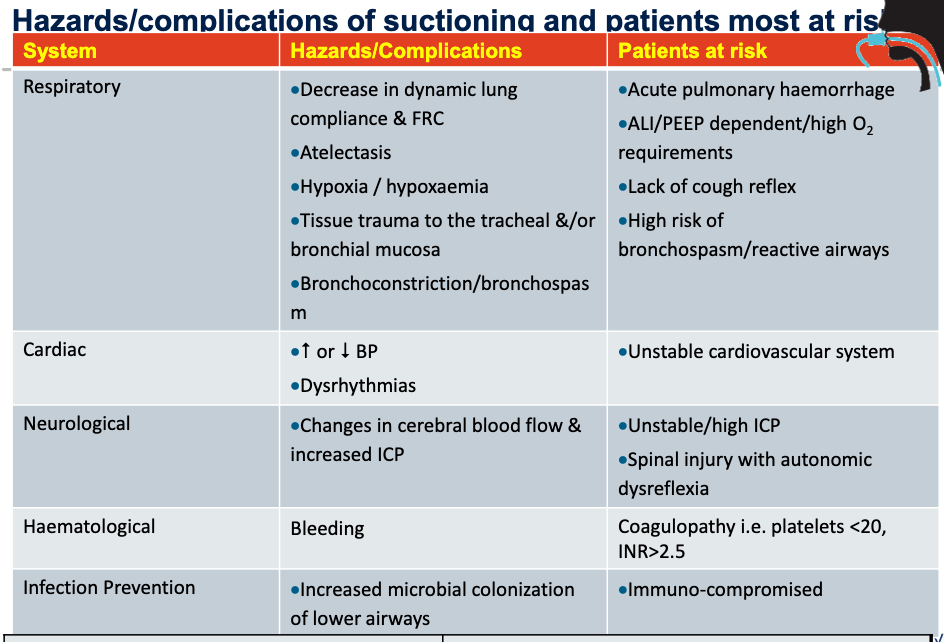
suctioning
manual techniques
mobilisation
MHI
Positioning
rationale:
improve gas movement (positioning
secretion movement (postural drainage)
spontaneuos breathing
preferentially distributd to dependent lung regions
positive pressure ventilation
preferentially distributed on non-dependent lung regions
Effects of positioning (gas movement)
increase negative intrapleural presssure in non-dependent lung region
gravity helps open air spaces by passively strechign the lungs
increase stretch/surfactant production → decrease surface tension
increases compliance of affected area that was placed uppermost
Food for thought re effects of positioning
differentiate between immediate and longer-term outcomes
can reduce V/Q matching n short term, as perfusion to dependent region and ventialtion to non-depedent
Effects of positioning (secretion movement)
drainage of secretion
head down tilt
can be hindered by ‘cardiovascualr instability’
defined as events which may threten or produce tissue ischaemia: such as AP <60-65,,Hg, recent BP variability, arrhythmias)
Positioning
SCI
strict positioning regime for management of MSK system
skeletal traction
limitation to position changes
ABI
influenced by changes in ICP
craniectomy - no bone
chest drains/UWSD
cardiac disease
Hyperinflation: gas and secretion mvoement
application of a larger than Vt breath with an anaesthetic or resuscitation circuit
Steps
deep breath
increase volume of the lungs, expanding the lung to produce more surfactant to increase compliance, and reduce surface tension
slow inspiration
reduces effect of airway resistance on distribition of ventilation
inspiratory hold
utilises collateral ventilation channels
Rapid release for expiration
annular two-phase gas-liquid flow
Monitoring during MHI
SpO2
HR/BP/MAP/ECG
airway pressure
auscultation
CPP and ICP
Ventilator hyperinflation
as per manual hyperinfaltion but performed via mechanical ventilator
can be performed in either volume or pressure cycled modes of ventilation
carefully titrated large Vt given to PIP 40cmH2O
6 sets of 6 breaths
VHI or MHI
no disconnection requried for VHI - maintenance of PEEP, avoids potential de-recruitment
some evidence that PEFR’s are greater with mapleson than lardel circuits, and that more secretions claeared with mapleson C than laerdal circuit
Precautions and contraindications
unstable respiratory system
unstable cardiovascular system
undrained pneumothorax
very stiff lungs
hyperinflated patients
raised intracranial pressure
saw-tooth pattern on the pressure → loose secretion build-up in endotracheal tube or condensate in tubing
Monitoring
SpO2
RR
pattern of braething
sputum colour
sputum amount
sputum viscosity
ECG
BP
MAP
Evidence
wearing protective gear during suctioning
tracheal suctioning should only be performed when clinically necessary for patinet and not dictated by routine
take maximum 15 secodns with negative pressure applied
effective cough should be produced
Concensus
clear explantion regardiing the procedure and the prcess should be give
clinical stability and the need to repeat suctioning depends on the amount of secretions and patient stability
the upper airway shoudl be suctioned as requried to remove oral secretions above the tracheostomy cuff
Pre-oxygenation
evidence does not support use of routine pre-oxygenation prior to suctioning
recommeneded in patients who are hypoxemic or at risk of significan desaturation during or after suctioning
Saline is not recommended, might casue reducetion in oxygen saturation five minutes after the suctioning
ICU acquired weakness
post-intensive care syndrome
poor physical, functional and cognitive outcomes
using early ICU exercise/mobilisation
positive effects shown
Considerations:
cardiovascular and neurological stability
physiological reserve
extent of injury/impairment
physiological reserve
extendt of injury/impairment
medical limitations