How Does the Heart Beat – Quick Review
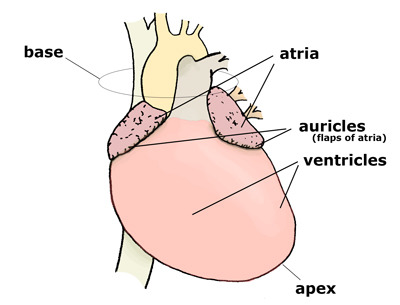
Cardiac Muscle Structure and Pump Function
Spiral fibre orientation "wrings" blood from apex to base.
Intercalated discs: desmosomes (strength) + gap junctions (electrical sync).
Two cell types: contractile (99 %) vs autorhythmic (1 %).
Specialized protein ; elevated plasma levels diagnose myocardial infarction.
Dual Circulation & Ventricular Differences
Right heart → pulmonary circuit; mean pressure .
Left heart → systemic circuit; mean arterial pressure .
Both eject ; left ventricle thicker due to higher resistance.
Pacemaker (Autorhythmic) Cells
Generate spontaneous action potentials (auto-rhythmicity).
Pacemaker potential phases:
• Phase 1: Na⁺ influx + ↓K⁺ efflux → slow depolarisation.
• Phase 2: T-type channels open → reach threshold.
• Phase 3: L-type channels open → rapid upstroke.
• Phase 4: K⁺ channels open, Ca²⁺ channels close → repolarise to .
Conduction Pathway & Intrinsic Rates
SA node: (primary pacemaker).
AV node: ; Bundle/ Purkinje: .
Route: SA → interatrial & internodal tracts → AV (delay) → Bundle of His → branches → Purkinje → ventricles.
Fibrous AV ring insulates atria from ventricles ensuring one-way spread.
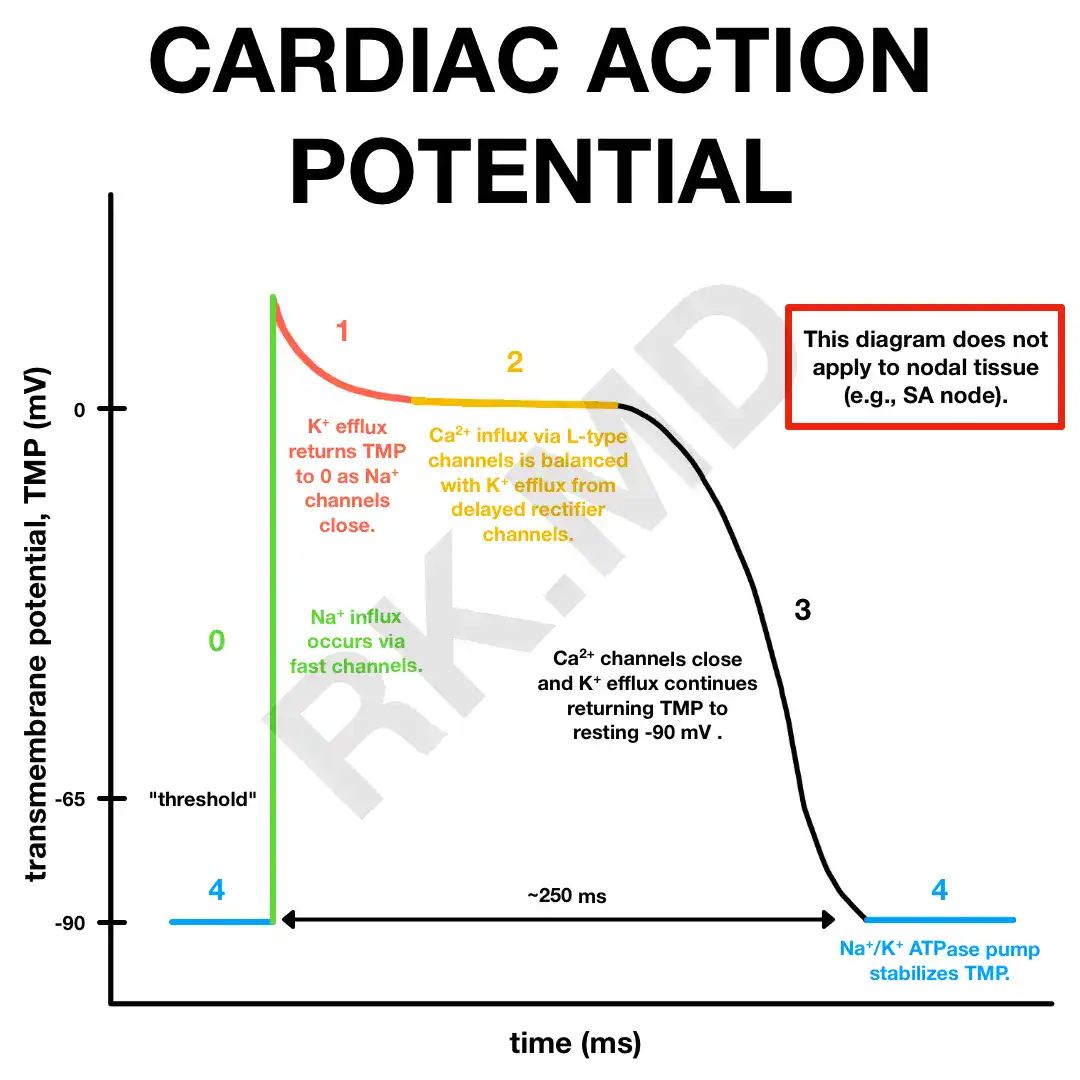
Contractile Cell Action Potential
Phase 0: Fast Na⁺ influx.
Phase 1: Transient K⁺ efflux.
Phase 2 (plateau): Slow L-type Ca²⁺ influx ≈ K⁺ efflux.
Phase 3: Ordinary K⁺ channels open → repolarisation.
Phase 4: Leaky K⁺ channels maintain .
Long refractory period prevents tetanus.
Excitation–Contraction Coupling
AP → T-tubules → Ca²⁺ influx via L-type channels.
Triggers Ca²⁺-induced Ca²⁺ release from SR.
Ca²⁺ binds troponin → cross-bridge cycling → contraction; removal → relaxation.
Force & Stroke Volume Control
Intrinsic: Starling law – ↑EDV stretches fibres toward optimal length → ↑stroke volume.
Extrinsic: Sympathetic ↑Ca²⁺ entry → stronger, faster contractions; Parasympathetic mainly lowers rate.
Autonomic Regulation of Heart Rate
SA intrinsic firing ≈ .
Resting HR (≈ ) set by dominant vagal tone (test with atropine → HR rises).
Sympathetic stimulation ↑HR & conduction velocity.
Clinical Notes
: Bradycardia ↓HR → ↓CO → potential hypotension.
Weakened/dilated heart (e.g., chronic alcohol) ↓contractility → ↓SV, ↓BP.
Cardiac Muscle Structure and Pump Function
Spiral fibre orientation "wrings" blood from apex to base.
Intercalated discs: desmosomes (strength) + gap junctions (electrical sync).
Two cell types: contractile (99 %) vs autorhythmic (1 %).
Specialized protein ; elevated plasma levels diagnose myocardial infarction.
Dual Circulation & Ventricular Differences
Right heart pulmonary circuit; mean pressure .
Left heart systemic circuit; mean arterial pressure .
Both eject ; left ventricle thicker due to higher resistance.
Pacemaker (Autorhythmic) Cells
Generate spontaneous action potentials (auto-rhythmicity).
Pacemaker potential phases:
Phase 1: Na
influx + ↓K
efflux → slow depolarisation.Phase 2: T-type channels open → reach threshold.
Phase 3: L-type channels open → rapid upstroke.
Phase 4: K
channels open, Ca²⁺ channels close → repolarise to .
Conduction Pathway & Intrinsic Rates
SA node: 70\100\ \text{AP/min} (primary pacemaker).
AV node: 40\60; Bundle/ Purkinje: 20\40.
Route: SA → interatrial & internodal tracts → AV (delay) → Bundle of His → branches → Purkinje → ventricles.
Fibrous AV ring insulates atria from ventricles ensuring one-way spread.
Contractile Cell Action Potential
Phase 0: Fast Na
influx.Phase 1: Transient K
efflux.Phase 2 (plateau): Slow L-type Ca²⁺ influx K
efflux.Phase 3: Ordinary K
channels open → repolarisation.Phase 4: Leaky K
channels maintain .Long refractory period prevents tetanus.
Excitation
Contraction Coupling
AP → T-tubules → Ca²⁺ influx via L-type channels.
Triggers Ca²⁺-induced Ca²⁺ release from SR.
Ca²⁺ binds troponin → cross-bridge cycling → contraction; removal → relaxation.
Force & Stroke Volume Control
Intrinsic: Starling law – ↑EDV stretches fibres toward optimal length → ↑stroke volume.
Extrinsic: Sympathetic ↑Ca²⁺ entry → stronger, faster contractions; Parasympathetic mainly lowers rate.
Autonomic Regulation of Heart Rate
SA intrinsic firing .
Resting HR (\approx \ 60\80) set by dominant vagal tone (test with atropine → HR rises).
Sympathetic stimulation ↑HR & conduction velocity.
Clinical Notes
: Bradycardia ↓HR → ↓CO → potential hypotension.
Weakened/dilated heart (e.g., chronic alcohol) ↓contractility → ↓SV, ↓BP.