DVT and PE
Deep Vein Thrombosis (DVT) and Pulmonary Embolism (PE)
Learning Objectives
Differentiate between:
Superficial venous thrombus
Deep vein thrombosis (DVT)
Understand Virchow’s Triad:
Venous stasis
Endothelial damage
Hypercoagulability
Anticipate anticoagulant therapy for:
VTE prophylaxis
Therapeutic anticoagulation
Compare and contrast anticoagulant therapies and nursing plans.
Implement nursing interventions aimed at preventing DVT.
Understand diagnostic tests for evaluating venous thrombosis.
Venous Thrombosis
Definition
Formation of a thrombus (clot) with vein inflammation.
Types
Superficial vein thrombosis:
Common in greater or lesser saphenous veins (thigh is greater and lesser is back of calf).
Deep vein thrombosis (DVT):
Most often in iliac and/or femoral veins.
Form on endothelium.
Preferred term: Venous thromboembolism (VTE).
Venous Thrombosis Characteristics
Known as a Fibrin clot:
Rich in fibrin and red blood cells (RBCs).
Fibrin is a protein responsible for blood clotting.
Occurs at low shear force on intact endothelial wall.
Easily mobilized; not tightly bound, thus leading to emboli.
Etiology of Venous Thrombosis
Virchow’s Triad: Factors Leading to Thrombosis
Venous Stasis:
Causes: Dysfunctional valves, inactive extremity muscles.
Risks: Obesity, pregnancy, chronic heart failure, long travels without exercise, prolonged surgery/immobility.
Endothelial Damage:
Causes (direct): Surgery, burns, IV catheter, trauma, prior VTE.
Causes (indirect): Chemotherapy, diabetes (glucose molecules larger), sepsis (increased lactic acid, etc).
Hypercoagulability of the Blood:
Increases activity of platelets in blood/makes blood thicker.
Factors Include:
Smoking (increases fibrinogen, homocysteine levels, activates intrinsic coagulation).
Estrogen-based oral contraceptives.
Postmenopausal with oral hormone therapy.
Family history of VTE and cancer.
Cancer
>35 years old.
SCDs are NOT PRN → if they’re ordered, keep them on unless ambulating or pt refuses.
Superficial Vein Thrombosis
Superficial leg veins most common
Clinical Manifestations
Symptoms include:
Palpable, firm, cordlike vein.
Itchy, painful, red, and warm area.
Mild fever, leukocytosis; associated with varicose veins.
Risk Factors
Increased age, pregnancy, cancer, obesity, estrogen therapy, recent surgeries, long-distance travel, history of CVI or VTE = all falls into Virchow’s Triad.
Superficial Vein Thrombosis: Interprofessional Care
Diagnosis and Treatment
Diagnosis: Venous ultrasound.
Treatment options for clots < 5 cm and near saphenousfemoral junction:
Oral/topical NSAIDs (help with pain).
Graduated compression stockings (helps bring blood flow back up).
Warm compresses (increases blood flow to decrease stasis and help healing with more WBCs)
Elevate limb above heart.
Mild exercise.
Deep Vein Thrombosis (DVT)
Deep veins of arms or les, pelvic, vena cava and pulmonary system.
Manifestations
Symptoms include:
Unilateral edema.
Pain and tenderness upon palpation.
Dilated superficial veins.
Full sensation in thigh or calf (feeling “heavy”, “tight”, or “full”)
Paresthesias (nerve compression), redness, warmth, fever > 100.4°F as body tries breaking down clots.
May develop lipodermaosclerosis
Changes skin pigmentation to be darker (brown discoloration), swollen limb, leathery skin from extreme swelling.
DVT Diagnostic Studies
Blood tests:
ACT, aPTT, INR, bleeding time, Hgb, Hct, platelet count (concerned about low count because there could be a clot then concerned about high due to potential of developing clot from hypercoagulable state), D-dimer (sees if clotting is happening in body in PVT, DVT).
Platelets will be low/lower than normal if there’s a clot.
Noninvasive:
Venous compression ultrasound, duplex ultrasound.
Invasive:
CT venography (go in and inject dye), MR venography, contrast venography.
Worried about kidney failure patients when using contrast dye.
DVT Complications
Pulmonary Embolism (PE).
Chronic Thromboembolic Pulmonary Hypertension → leads to death from HF for pulmonale.
Postthrombotic Syndrome (PTS).
VTE Interprofessional Care
Prevention and Prophylaxis
VTE prophylaxis is a core healthcare measure developed by TJC. (Means every patint must have a VTE prophylaxis).
Prevents clot formation.
Interventions Based On:
Bleeding and thrombosis risk, patient history, medications, and patient preferences.
Key measures:
Early, progressive mobilization (if they can, pts should be up in a chair when eating or walking).
Graduated compression stockings.
Intermittent pneumatic compression devices (IPCs).
VTE Medications
Types of Anticoagulants
Vitamin K Antagonists (Warfarin):
Takes 48-72 hours to be effective; monitor INR. Used longterm. Need a bridge therapy until INR in therapeutic range.
Antidote: Vitamin K.
Monitor: INR and PT balance.
Pts must maintain consistent diet of green leafy vegetables.
Thrombin Inhibitors:
Includes unfractionated heparin (UH), low molecular weight heparin (LMWH).
Affects plasma antithrombin coagulation pathway;
Antidote: Protamine Sulfate
Unfractioned Heparin: Heparin different size
Monitor for heparin-induced thrombocytopenia (HIT).
This means the heparin is working too well and now pt is at bleeding risk
low molecular weight: same sizes and remains consistect.
Factor Xa Inhibitors:
Direct oral anticoagulants (DOACs): Apixaban, Rivaroxaban.
No dietary restrictions or lab monitoring required.
VTE in Nursing Management
Anticoagulant Therapy
For prophylaxis: Adjust based on risk level.
For treatment: Adjust based on INR and patient conditions.
Thrombolytics: Indicated for patients with low risk of bleeding and extensive VTE.
Surgical and Interventional Options
Open venous thrombectomy and IVC filter for high-risk PE.
Percutaneous interventions involving catheter-directed thrombolytics.
Nursing Management: DVT and PE
Patient Support
Address anxiety, pain, and educate on long-term anticoagulant therapy.
Prevention Measures
Use of IPC devices, early ambulation, and teaching patients about VTE prevention.
Pulmonary Embolism (PE)
Etiology and Pathophysiology
Blockage of pulmonary arteries by thrombus, fat, air embolus, or tumor tissue.
Leads to lung tissue death.
Most often affects lower lobes due to them being smaller.
Commonly originates from DVT (VTE = spectrum from DVT to PE).
Most Common Causes: deep veins of legs, femoral or iliac veins, right side of heart (Afib causes risk of PE or stroke due to vascular stasis), and pelvic veins (especially after surgery or childbirth).
Superficial doesn’t normally become a PE → they don’t break off as often as a DVT does.
Less Common Causes: Central venous catheter or arterial lines (breaks off and causes PE from blood clotting around it and breaking off), fat (fractured long bones with more yellow marrow and breaks off), air (IV → air embolus from too much air), vegetation on heart valves, amniotic fluid, cancer (tumor tissue growing in lungs and blocking off vasculature).
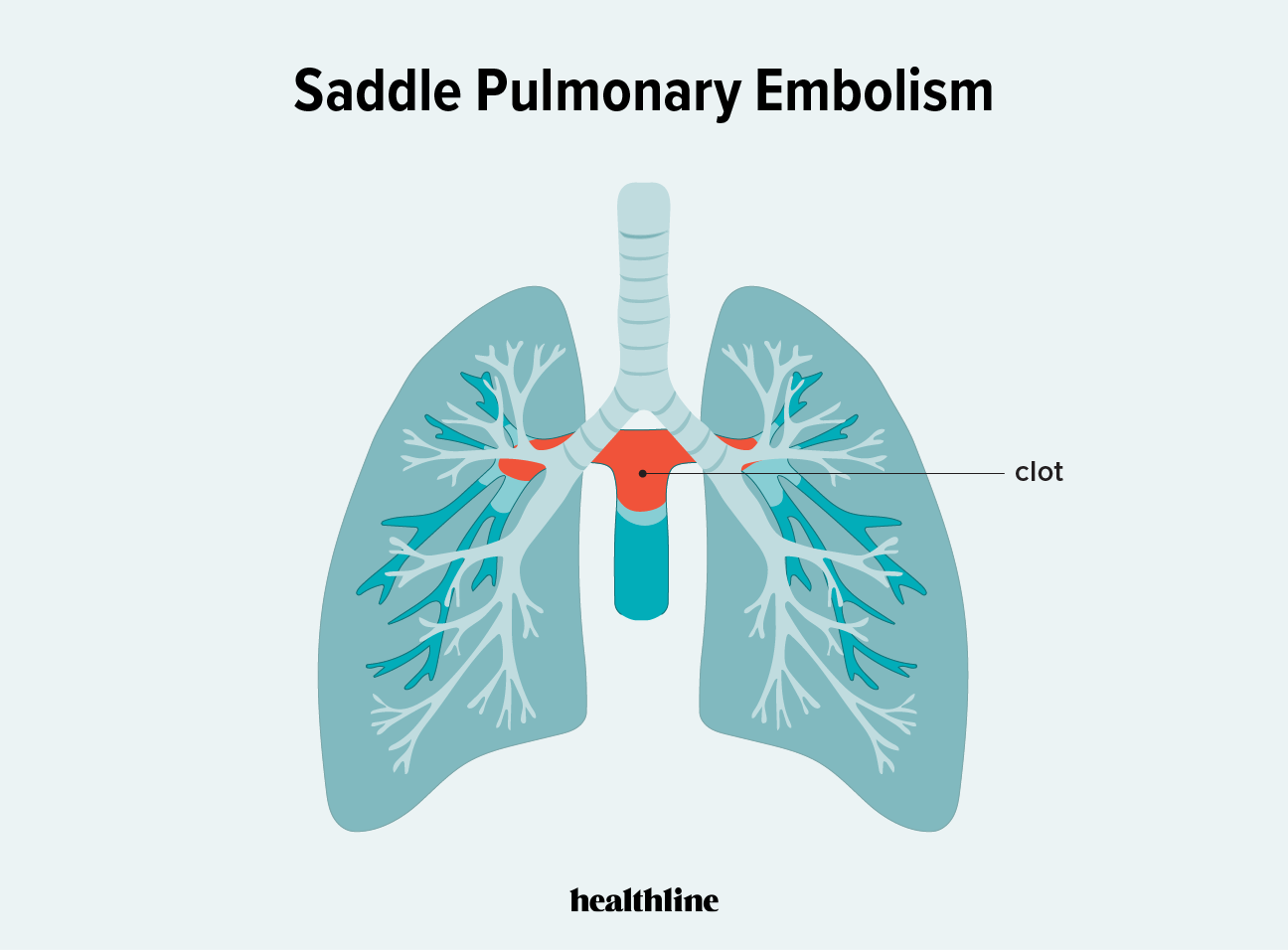
Saddle Embolus: Large thrombus that sits in the bifurcation (both branches) of the pulmonary arteries and block off blood flow to both lungs.
Worse outcome (life-threatening)
Risk Factors
Include immobility
History of VTE
Recent surgery within 3 months (especially pelvic and lower extremity)
Likelihood of developing blood clot is about 60% for patients that have a total knee replacement.
Cancer
Obesity
Hormonal therapies
Smoking
Heart failure
Pregnancy
Clotting disorders
Clinical Manifestations
Depends on type, size, and extent of emboli.
Larger Emboli: Sudden onset
Smaller Emboli: Gradual onset
Dyspnea most common
Mild-moderate hypoxemia
Determined by ABGs → SPO2 in blood.
Other: Tachypnea, cough, chest pain, hemoptysis, crackles, wheezing, fever, tachycardia, syncope (not perfusing brain/lacking blood flow to brain), pulmonic heart sounds.
Symptoms caused by decreased perfusion
Massive PE: Altered mental status (deoxygenation), hypotension, impending doom, cardiorespiratory arrest/death.
Complications
Pulmonary Infarction: Death of lung tissue.
PE decreases blood flow to lung tissues and causes alveolar lung necrosis and hemorrhage.
Pulmonary Hypertension: Increased pressure in pulmonary artery.
Commonly due to back up of blood from a large PE and/or multiple PEs.
Scarring after multiple prior PEs
Ex. If someone has a DVT that’s slowly breaking off it can lead to scar tissue.
Right ventricular hypertrophy (Cor pulmonale)
Cor pulmonale (right sided HF) symptoms: Dependent pitting edema → weeping edema if it worsens.
Pt already has respiratory symptoms like dyspnea since it started as a PE, but Cor pulmonale develops into the “rest of the body” HF symptoms.
Diagnostic Studies for PE (3)
D-Dimer: Indicates fibrin degradation, often elevated.
Also performed for normal VTE or DVT.
CT Angiography (CTA): Looks at vasculature through chest cavity/lungs. Requires IV contrast. GOLD STANDARD.
Worried About: Kidney failure patients & shellfish allergy.
Ventilation-Perfusion (V/Q) Scan: Assess ventilation and perfusion.
Perfusion Scanning → radioscopic injection; looks at pulmonary circulation (not nephrotoxic, it takes a chest scan and looks at where vasculature goes).
Ventilation Scanning → Pt breathes in radioactive gas to visualize air distribution.
Intubated and sedated patients unable to participate.
Important but Non-Diagnostic Studies
ECG (nonspecific ST segment and T wave changes)
Hypoxia → Depressed ST segment
Chest x-ray (atelectasis or pleural effusion from immune system activation to break down PE by sending more WBCs and fluid to that area)
Lactic acid if worried about alveolar necrosis.
H&H if worried about hemorrhage.
Platelets generally low in patients who are bleeding.
Troponin levels usually high
Levels increase when there’s cardiac ischemia (not enough oxygen to heart muscle)
BNP
Determines if there’s stretch from potential fluid volume overload
Interprofessional Care for PE
Immediate Management
Start anticoagulation immediately (prevents clot from getting bigger and decrease risk of emboli)
3 Phases (dependent on cause):
Initial: First 7 days
Longer: Up to 6 weeks
Extended: 6 months and beyond
Support cardiorespiratory status (varies by size and location of PE).
Oxygen → ABG tells provider what type of oxygen is needed.
Mild Hypoxemia: nasal cannula or face mask.
Extreme Hypoxemia: Mechanical ventilation or hiflow
Pulmonary hygiene (IS, ambulation, position into semi-high fowlers)
Obstructive Shock: IV fluids (not for HF patients nor elevated BNP), vasopressors (helps perfuse major organs)
HF: Diuretics
Check BNP and see if patient has peripheral edema
Pain: Opioids
Make sure respiratory rate (O2) is good
Respiratory acidosis risk
Monitor coagulation levels closely and adjust treatment accordingly.
Surgical and Med Therapy
Anticoagulant Medication (immediate):
LMWH (Lovenox): Weight based
Molecules are all the same size (more predictable, no lab monitoring)
Unfractionated IV Heparin:
Warfarin (Coumadin):
Takes several days to reach therapeutic levels.
Admission 3 months or longer.
Fibrinolytic Agents (dissolves clot): High risk for bleeding
Tissue Plasminogen Activator (tPA)
Alteplase (Activase)
Pulmonary embolectomy for massive PE (removes PE)
For hemodynamically unstable patients (not well perfused → present with altered mentation and cyanosis, monitor vital signs)
Contraindicated: thrombolytic therapy.
Inferior vena cava filter to prevent migration of clots in pulmonary system
Used if they deliver a PE related to a DVT
It can get full especially in patients where a lot of clots are breaking off and may end up needing an embolectomy or tPA.
Medications: Antiplatelet and anticoagulants (dual)
IVC introduces something new to body that body will try to fight off = need antiplatelets.
Percutaneous Catheter Embolectomy:
Patient Education and Follow-Up
Prevention #1:
Intermittent pneumatic compression devices (SCDs)
Early ambulation
Anticoagulation
High risk pts also encouraged to take antiplatelets like low-dose baby aspirin (81mg).
Immediate Treatment:
Bed rest in semi-fowler’s position to bring more oxygen
Assess cardiopulmonary status
Listen to lungs and heart, check cap refill, check for edema, cyanosis.
Administer: Oxygen, IV fluids and medications (question these orders as needed, ex. HF pts → fluid restriction).
Monitor For:
Coagulation (specific to medication)
Warfarin → Check INR
Heparin → aPTT or factor Xa
Anticoagulants → kidney function
Complications
Heparin-Induced Thrombocytopenia (HIT)
Generalized bleeding (from the gums, ears, eyes, nose)
Hemorrhagic stroke (from anticoagulants)
Monitor neurologic function & pupil response.
Nursing Management:
Fall precautions once out of bed (bleeding risk = immediate fall risk)
Patient emotional support
Patient Education: Long-term anticoagulant therapy (3+ months), importance of follow-up exams, VTE prevention.