Ab Psych Chapter 5: Anxiety Disorders - Panic Disorder & OCD
- Having panic attacks does not mean you have panic disorder
- Panic disorder typically develops in late 30s.
- More highly reported among Native Americans and then White individuals, then Hispanic, Black, and Asian/Pacific Islander
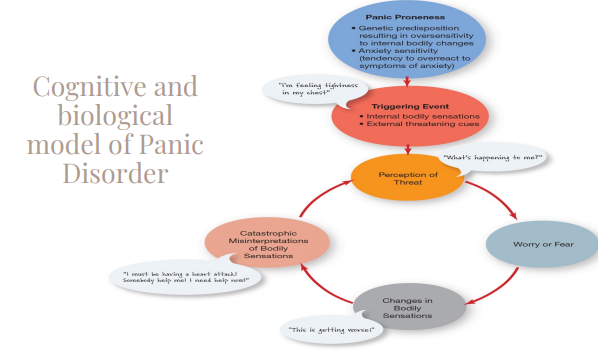
- Cognitive Biological model of Panic Disorder:
- Starts with a genetic predisposition resulting in oversensitivity to internal bodily changes
- Anxiety Sensitivity: fear of arousal-related bodily sensations arising from beliefs about the meaning of anxiety sensations. Fear of fear itself
- reciprocal relationship of cognition and biology
- Transdiagnostic mechanism: it’s relevant to many disorders besides panic disorder
- Panic disorders are comorbid with agoraphobia
- Second is the triggering event, so external threatening cues or internal bodily sensations that work with the panic proneness to cause a perception of threat.
- Sympathetic nervous system is activated and your fight or flight kicks in, increases in bodily sensation are mistakenly interpreted as a threat; can cause panic attack
- Combination of factors above mentioned that work together, which prime you to experience a panic attack.
- Biological Factors:
- Neurotransmitters gamma-aminobutyric (GABA) and serotonin, imbalances in these causes heightened anxiety.
- Genetic variants of genes of neurotransmitter system may influence development of pure and comorbid panic disorder.
- Biological challenge studies - Individuals with panic disorder are more likely than controls to experience anxiety/panic symptoms during biological challenge
- Treatment:
- Medication - Antidepressant and benzodiazepines
- Work to normalize activity of specific neurotransmitters
- Has some bad side effects - can aggravate symptoms
- Medication helps to manage symptoms; it is not a cure
- Cognitive Behavioral Therapy - Combines various techniques like self monitoring, coping skills training, breathing retaining, relaxation training, exposure, decatastrophizing
- Has better short and long term outcomes compared to medication
- gold standard for panic disorders
- Agoraphobia: Marked fear of anxiety about two or more of the following situations:
- Using public transportations, being in open spaces, being in enclosed places, stranding in line or being in a crowd, being outside or home alone
- People predisposed to panic disorder are likely to develop agoraphobia.
- Obsessive-Compulsive and Related Disorders
- DSM Criteria: Presence of obsessions, compulsions, or both.
- The obsessions or compulsions are time consuming, or cause clinically significant distress or impairment in social, occupational, or other important areas of functioning.
- The obsessive-compulsive symptoms are not due to physiological effects of a substance or medical condition.
- The disturbance is not better explained by the symptoms of another mental disorder.
- Obsessions are defined by BOTH:
- Recurrent and persistent thoughts, urges, or images that are experienced at some time during the disturbance as intrusive and unwanted, and that in most individuals cause marked anxiety or distress.
- The individual attempts to ignore or suppress such thoughts, urges, or images or to neutralize them some other thought or action (i.e., performing a compulsion)
- Compulsions are defined by BOTH:
- Repetitive behaviors or mental acts that the individual feels driven to perform in response to an obsession or according to rules that must be applied rigidly.
- The behaviors or mental acts are aimed at preventing or reducing anxiety or distress, preventing some dreaded event, or situation; however, these behaviors or mental acts are not connected in a realistic way with what they are designed to neutral or prevent or are clearly excessive.
- People with OCD generally recognize their obsessive thoughts are irrational
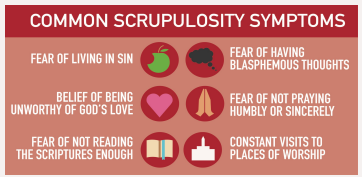
- OCD can take various forms: Contamination, Aggressive/harm, Sexual, Religious (scrupulosity), Symmetry, Sensorimotor (ex: being preoccupied with how often you swallow)
- Most prevalent in 18-29 (1.5%) and 30-44 (1.4%) year olds
- Comorbid with anxiety disorders, dispersive disorders, and other compulsive disorders.
- Theoretical Perspectives on OCD:
- Cognitive - Faulty interpretations turn intrusive thoughts into obsessions. Five types of intrusive thoughts into obsessions are as such:
1. Threat overestimation: e.g., profanity in church → eternal damnation 2. Thought-action fusion: Belief that thinking about something makes it more likely to happen. e.g., bad thoughts = bad deeds 3. Mental control: Must get thoughts out of head to avoid doing something bad! 4. Intolerance of uncertainty: need perfect certainty that the fear won’t come true to continue with routine 5. Perfectionistic beliefs: e.g., one impure thought → whole service is ruined
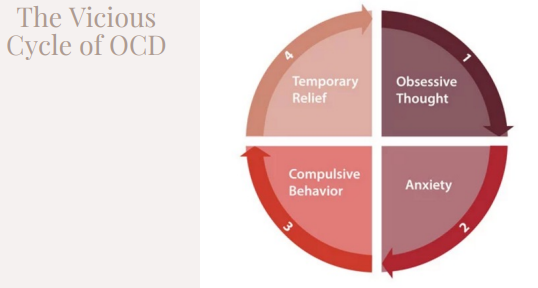
- Learning Perspective - Compulsions are negatively reinforced
- Biological Perspective - Gene variations may affect chemical balance and lead to over-arousal of “worry circuit”.
- Treatment for OCD:
- Exposure with response prevention (ERP): Exposure involves repeated and prolonged exposure to the stimuli or situation that evokes obsessive thoughts. And Prevention involves preventing the compulsive behavior from occurring.
- Client learns to tolerate anxiety
- 60 to 80% of people treated with ERP show reductions in symptoms
- Cognitive Behavioral Therapy: Focused on correcting cognitive distortions and overestimation of consequences.
- Medication: Antidepressant medications (SSRIs) can be effective in treating OCD.
- Psychotherapy is typically more effective than medication along
- Combination treatment may boost effectiveness of drug treatment alone.
- Body Dysmorphic Disorder: Preoccupation with imagined or exaggerated physical defect (skin blemish, wrinkling, swelling of the face, moles or spots). Flaw usually doesn’t exist or is exaggerated, feel ugly and deformed, and extreme fear they will be judged negatively due to this flaw.
- BDD is considered an obsessive-compulsive related disorder because you are having obsessions with perceived defect. May feel compelled to check self in mirror. Other compulsions may be related to fixing, covering, or modifying perceived defect
- BDD Stats: Prevalence among U.S. adults = 2.4%. Median age of onset = 15 years, Comorbid with substance use, OCD, and social phobia. High rates of suicidal ideation and attempts among both adolescents and adults with BDD. Recovery takes a very long time.
- BDD Risk Factors: Genetic factor - BDD more likely in those whose relatives also have this or another OC-related condition
- Certain personality traits (e.g., perfectionism)
- Culture and environment (societal expectations of beauty)
- Negative life experiences (e.g.,
childhood bullying and trauma)
- Treatment for BDD:
- Exposure with response prevention (ERP)
- Exposure: intentionally revealing the perceived defect in public
- Response prevention: avoid mirror checking or excessive grooming
- ERP generally combined with cognitive restructuring
- Evaluate distorted thoughts and beliefs about appearance in light of evidence
- Hoarding Disorder: Excessive acquisition of and difficulty discarding possessions, resulting in a cluttered space
- Clutter results in distress, and often interpersonal conflict and danger
- Affects 2-6% of the population, more prevalent in adult population
- Difficult to treat
- Why is hoarding disorder considered an obsessive-compulsive related disorder?
- Obsessions may involve recurring thoughts about acquiring objects and fears over losing them.
- Compulsions may involve repeatedly rearranging stacks of possessions and refusing to discard them
- But… it differs from OCD: OCD has a more distressive component. In OCD, one can’t control their compulsions and have to perform that behavior, while in hoarding it is less.
- Trichotillomania:
- Repetitive hair pulling that results in noticeable hair loss
- Scalp, eyebrows, and other places of the body
- Excoriation
- Recurrent skin picking, sometimes resulting in sores, infections, and scars