Lecture 3 – The Placenta
Functions of the Placenta
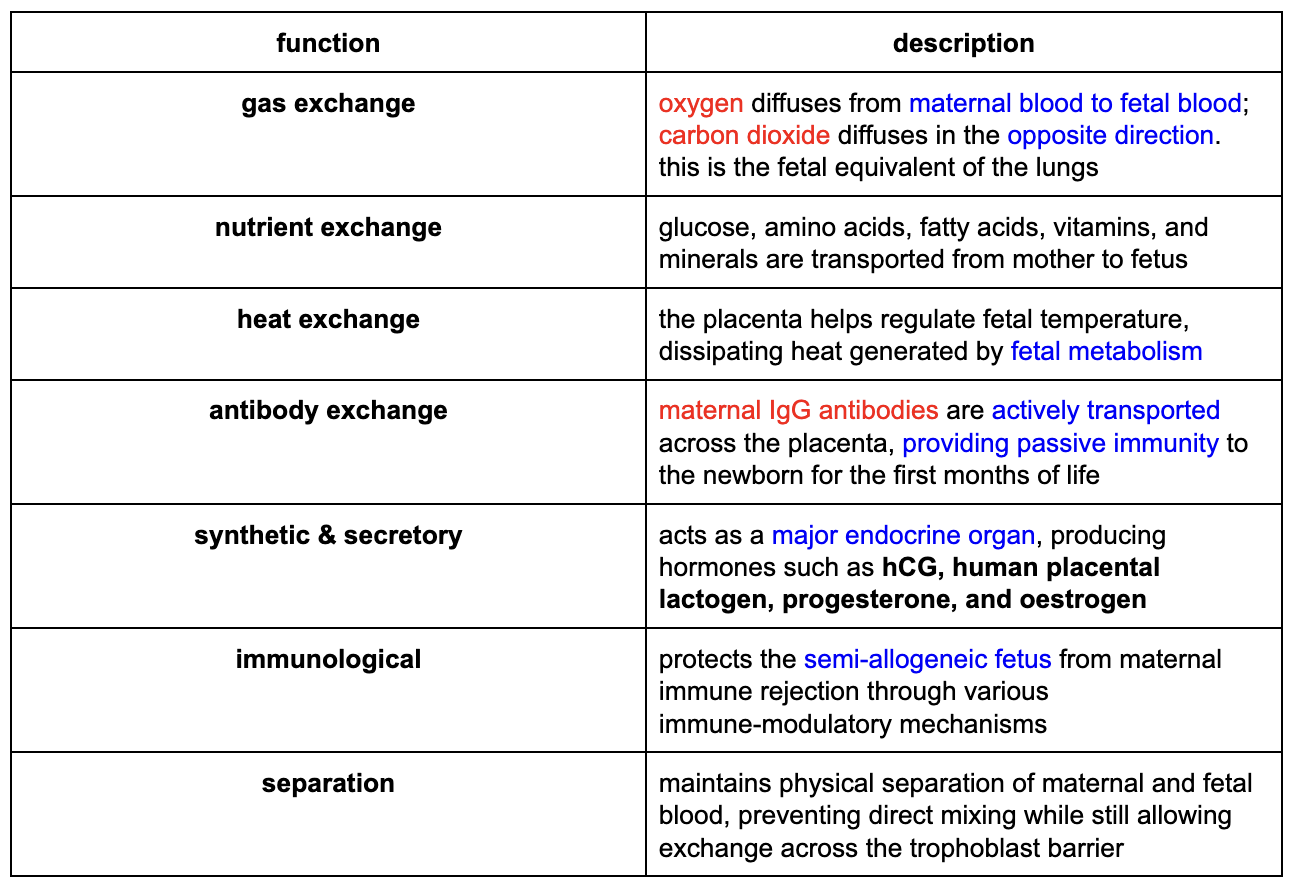
The placenta is a temporary organ that serves as the interface between the mother and the fetus, performing multiple critical functions that would otherwise be carried out by the fetus’s own organs after birth. It’s both an organ of exchange and a complex endocrine gland.
Trimesters of Pregnancy
understanding placental development requires knowledge of the timeline of pregnancy:
1st trimester
conception to 12 weeks
this is the period of organogenesis and the critical period for establishment of the placenta
2nd trimester
13 to 24 weeks
rapid fetal growth
placenta becomes fully functional and continues to mature
3rd trimester
25 weeks to term (36 to 40 weeks)
continued growth and maturaion
fetus gains weight and the placenta reaches its maximum exchange capacity
Early Placental Development: From Implantation to Villi
placenta development begins immediately after implantation and proceeds through distinct stages
lacunar stage (days 8 to 12)
the primitive syncytiotrophoblast invades the endometrial decidua
it forms spaces called lacunae (gaps) within the syncytial mass
the trophoblastic protrusions between lacunae are called trabeculae
these lacunae tap into maternal blood vessels, establishing the first flow of maternal blood into the developing placenta
marks the beginning of the intervillous space
villous period (from ~day 12)
primary villi (~day 12): cytotrophoblasts proliferate and invade the trabeculae, forming primary villi which are solid columns of cytotrophoblast covered by a continuous layer of syncytiotrophoblast
secondary villi (~day 14): cells of the extraembryonic mesenchyme invade the core of the primary villi, converting them into secondary villi with a mesenchymal core
tertiary villi (18 to 20 days): fetal blood vessels form within the mesenchyme of the secondary villi. these are now tertiary villi, the functional exchange units of the placenta. from this point onward, almost all villi are tertiary. the vessels within them connect to the developing umbilical vessels, establishing the fetal-placental circulation
Key Cell Types of the Placenta
villous cytotrophoblast (VCTB)
these are the progenitor cells of the trophoblast lineage
lies as a single layer beneath the syncytiotrophoblast, particularly prominent in the first trimester
proliferate and fuse to maintain the overlying syncytiotrophoblast
syncytiotrophoblast (STB)
this is the outer, multi-nucleated surface layer of the villi
it’s in direct contact with maternal blood in the intervillous space
the STB does NOT divide
it’s constantly renewed by the fusion of underlying cytotrophoblasts
responsible for nutrient and gas exchange as well as hormone production
extravillous cytotrophoblast (EVT)
these are differentiated cytotrophoblast that have migrated out of the villous placenta and into the maternal decidua
they form columns from anchoring villi and invade the decidua and the walls of the maternal spiral arteries, remodelling them into low-resistance, high-flow vessels to supply the placenta
Types of Chorionic Villi
two main types of villi are present in the mature placenta, distinguished by their function:
anchoring villi
these villi extend form the chorionic plate (fetal side) down to the decidua basalis
at their tips, cytotrophoblast break through the syncytiotrophoblast, proliferate, and spread laterally to form a continuous cytotrophoblast shell that anchors the placenta to the maternal tissue
columns of EVTs continuously stream out from these villi to invade the decisudea and spiral arteries during the first and second trimesters
floating villi
these are the majority of villi
they’re suspended in the intervillous space and don’t have direct contact with maternal tissues
they’re the primary sites for the exchange and barrier functions of the placental
maternal blood bathes these villi, and fetal blood circulates within their capillaries,
allowing for efficient diffusion and transport
Formation of the Definitive Placenta
The early placenta forms as a sphere of villi surrounding the embryo. As gestation progresses:
villi on the sides and the luminal aspect regress and disappear, forming the smooth chorion
only the villi basal to the implantation site continue to grow and branch
this results in a discoid, or disc-shaped, definitive placenta
the placenta takes its definitive structure by approximately 12 weeks gestation
Maternal Contributions: The Decidua
the maternal component of the placenta is derived from the endometrium, which undergoes significant changes under the influence of progesterone. this transformation is called the decidual reaction
decidual reaction
endometrial stromal cells become swollen, accumulate glycogen and lipids, and the tissue becomes oedematous
this provides a nutrient-rich environment for the implanting embryo
in humans, this reaction begins spontaneously during the secretory phase of each menstrual cycle and is enhanced after implantation
regions of the decidua
decidua basalis
the portion of the decidua that lies directly underneath the implantation site
it forms the maternal part of the placenta and is intermingled with the anchoring villi
decidua capsularis
the portion of the decidua that lies over the implantation site, covering the developing embryo and facing the uterine cavity
decidua parietalis
the decisua lining the rest of the uterus, not involved in the implantation site
fusion
as the fetus and amniotic cavity enlarge, the decidua capsularis is pushed against the decidua parietalis, and the two eventually fuse, obliterating the uterine cavity by the end of the first trimester
Spiral Artery Transformation
a critical function of extravillous cytotrophoblasts is the invasion and remodelling of the maternal spiral arteries
EVTs migrate from the anchoring villi, travel through the decidua, and penetrate the walls of the spiral arteries.
They replace the maternal endothelial lining and disrupt the smooth muscle layer.
This transforms the narrow, high-resistance spiral arteries into wide-bore, low-resistance vessels that are incapable of vasoconstriction.
This ensures a high-volume, continuous flow of maternal blood into the intervillous space to meet the metabolic demands of the growing fetus.
Failure of this transformation is associated with serious pregnancy complications, including pre-eclampsia and fetal growth restriction (FGR).
Umbilical Cord
The umbilical cord connects the fetus to the placenta.
Derived from the yolk sac and allantois. The vessels are derived from the allantois.
Contains two umbilical arteries and one umbilical vein.
Umbilical Arteries: Carry deoxygenated blood and waste products from the fetus to the placenta.
Umbilical Vein: Carries oxygenated blood and nutrients from the placenta to the fetus.
Wharton's Jelly: The vessels are embedded in a gelatinous, protective connective tissue called Wharton's jelly, which contains myofibroblasts and mucopolysaccharides. This prevents compression, kinking, and occlusion of the cord.