CHN Part 1
WHAT IS THE JOHARI WINDOW MODEL?
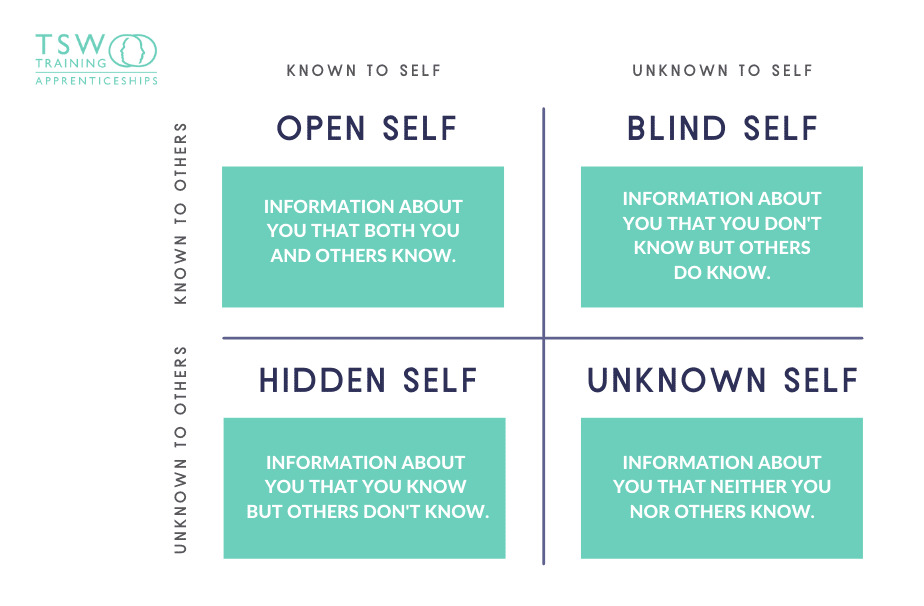
The Johari Window improves self-awareness and mutual understanding between individuals within a group. It is particularly helpful for leaders who want to understand how people perceive them.
It was devised by American psychologists Joseph Luft and Harry Ingham in 1995 while researching group dynamics at the University of California Los Angeles. The model was first published in the Proceedings of the Western Training Laboratory in Group Development by UCLA Extension Office in 1995, and was later expanded by Joseph Luft. The model name is derived from combining the two names Joseph and Harry.
WHY USE THE JOHARI WINDOW MODEL?
The effectiveness of your leadership will be limited by your Self-Awareness. Improving self-awareness will help you listen, be more present and be better in tune with the person or group you are leading.
The Johari Window model develops internal and external self-awareness. It helps you become aware of how others see you in contrast to how you see yourself.
A good outcome is a perfect alignment between how you see yourself and others see you. This happens when you are a very open leader who has worked with a stable group for some time.
A common outcome is a difference between how you see yourself and others see you. There are values important to you that others are unaware of. There are also values you demonstrate that other people see but you are not aware of.
The Johari window helps create this awareness of these contrast. With this knowledge, you can work to increase your open area. Where how you see yourself aligns with how others perceive you. This is done by discussing the results with the group and seeking greater understanding.
WHAT ARE THE FOUR QUADRANTS OF THE JOHARI WINDOW?
DEFINITION OF TERMS
COMMUNITY
Seen as a group or collection of locality-based individuals interacting in social units, and sharing common interests, characteristics, values, and/or goals.
Definition of Community According To:
ALLENDER
“a collection of people who interact with one another and whose common interests or characteristics form the basis for a sense of unity or belonging.”
LUNDY AND JANES
“a group of people who share something in common and interact with one another, who may exhibit a commitment with one another and may share geographic boundary.”
CLARK
“a group of people who share common interests, who interact with each other, and who function collectively within a defined social structure to address common concerns.”
SHUSTER AND GOEPPINGER
“a locality-based entity, composed of systems of formal organizations reflecting society’s institutions, informal groups and aggregates.”
COMMUNITY ORGANIZING
Community organizing as a process consists of steps or activities that instill and reinforce the people’s self-confidence on their own collective strengths and capabilities (Manalili, 1990). It is the development of the community’s collective capacities to solve its own problems and aspire for development through its own efforts.
Community organizing is a continuous process of educating the community to develop its capacity to assess and analyze the situation (which usually involves the process of consciousness raising), plan and implement interventions (mobilization), and evaluate them.
Community Organizing is a process of educating and mobilizing members of the community to enable them to resolve community problems. It is a means to build the community’s capacity to work for the common good in general and health goals.
Community organizing and community health nursing practice have common goals: People empowerment, development of self-reliant community, and improved quality of life. As a result, they become the health care professionals’ partners in health care delivery and overall community development.
HEALTH
Definition of Health According To:
WHO – “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity.”
Murray – “a state of well-being in which the person is able to use purposeful, adaptive responses and processes physically, mentally, emotionally, spiritually, and socially.”
Pender – “actualization of inherent and acquired human potential through goal directed behavior, competent self-care, and satisfying relationship with others.”
Orem – “a state of person that is characterized by soundness or wholeness of developed human structures and of bodily and mental functioning.”
TYPES OF COMMUNITY
Two main types of communities (Maurer & Smith, 2009):
Geopolitical communities AKA Territorial Communities
most traditionally recognized
defined or formed by both natural and man-made boundaries and include barangays, municipalities, cities, provinces, regions and nations.
Phenomenological communities AKA Functional Communities
refer to relational, interactive groups, in which the place or setting is more abstract, and people share a group perspective or identity based on culture, values, history, interest and goals
CHARACTERISTICS OF A HEALTHY COMMUNITY
According to Hunt, 1997; Duhl, 2002
Shared sense of being a community based on history and values.
General feeling of empowerment and control over matters that affect the community as a whole.
Existing structures that allow subgroups within the community to participate in decision making in community matters.
Ability to cope with change, solve problems and manage conflicts within the community through acceptable means.
Open channels of communication and cooperation among the members of the community
Equitable and efficient use of community resources, within the view towards sustaining natural resources.
A healthy community is, in fact, the context of health promotion defined in the Ottawa Charter (WHO, 1986) as “the process of enabling people to increase control over and to improve their health.”
A healthy city is one that is continually creating and improving those physical and social environments and expanding those community resources that enable people to mutually support each other in performing all the functions of life and developing to their maximum potential. It aims to:
Achieve a good quality of life
Create a health-supportive environment
Provide basic sanitation and hygiene needs
Supply access to health care
EIGHT SUB-SYSTEMS OF A COMMUNITY
Physical Environment
Safe water and clean air, healthy workplaces, safe houses communities and roads contribute to good health
Education
These includes laws, regulations, facilities, activities affecting education, ratio of health educators to learners, distribution of educational facilities, who utilizes these, what informal educational facilities and activities exist in the community. Low education levels are linked with poor health, more stress and lower self-confidence.
Safety and Transportation
Safe and healthy residents lead to stronger, more resilient communities. People feel safe when they are respected, valued, and have access to a full range of health, social, natural, and educational resources. Transportation is a critical factor that influences people’s health and the health of a community. Investments in sidewalks, bike lanes, trails, public transit, and other infrastructure that supports physical activity can result in improvements to individuals’ health and decreased health care costs.
Politics and Government
Politics and government is the working hand in the community, wherein it is the one responsible in delivering the services to the people. Political structures present in the community, decision-making process/pattern leadership observed, etc.
Health and Social Services
Access and use of services that prevent and treat disease influences health. Health facilities and activities distribution, utilization, ratio of providers to clients served; priorities in health, programs develop, and social services for the marginalized sector of the community.
Communication
Systems, types of communication existing, forms of communication, be it formal or informal; etc. Communication is developmental and it transfers ideas to all areas of life; home, community, work, and beyond. Through this collaboration and cooperation occur.
Economics
Economy is the realized social system of production, exchange, distribution, and consumption of goods and services of a country or other area. Occupation, types of economic activities, income, etc. Higher-income and social status are linked to better health. The greater the gap between the richest and poor health, the greater differences in health.
Recreation
Recreational activities/facilities; types, consumers, appropriateness to consumers, etc. Recreation or fun is the expenditure of time in a manner designed for therapeutic refreshment of one’s body and mind.
COMPONENTS OF COMMUNITY
A community can be described as a complex whole resulting from the combination of the environment, people health, quality of life, and economics. The functionality of a community depends solely in these key elements. Thus, the components of the community are as follows:
The environment
The people
The economy
The culture
The health
The quality of life
DETERMINANTS OF HEALTH AND DISEASE
The health status of a community is associated with several factors:
Health Care
Access
Economic Conditions
Social
Environmental Issues
Cultural Practices
ROLE OF THE NURSE IN COMMUNITY ORGANIZING
The complex nature of the health needs of communities calls for a holistic response from public health nurses. This in effect demands not only collaborative interventions but at the same time the nurse working with communities is expected to demonstrate competencies demanded by different settings and situations of his/her clientele. The Philippine Professional Regulatory Board of Nursing (NNCCS, 2012) expects beginning professional nurses to be able to perform three roles: that of health care provider, manager leader, and researcher. But a community and public health nurse takes on additional roles, owing to the realities of changing times and age.
HEALTH CARE PROVIDER
Caring is the essence of nursing and has been widely accepted in all settings. The use of the nursing process applied in the natural environment of the client pertains to this role. Examples include the occupational health nurse conducting a physical examination of an employee, a school nurse providing first-aid to student who sustained a cut and a nurse taking the history of a pregnant woman in the village clinic.
HEALTH EDUCATOR
Communication information to help patients make an informed choice regarding their health is a key activity in public health works. It is hoped that awareness will impact people’s behavior to achieve in their own hands. Instructing patients how to take their prescribed medicine or sharing information about the benefits of healthy lifestyle illustrates this role.
PROGRAM IMPLEMENTER
Nurses working under local government units deliver healthcare to the grassroots. This also requires that programs initiated by the national government thru the Philippine Department of Health (DOH) are executed at all levels. This includes immunization which offers protection against infectious diseases. The nurse works with the rural health midwife in conducting routine vaccination in communities to achieve herd immunity and contribute to the over-all goal of reducing child mortality. Likewise, submitting reports per standards of documentation on targets reached and missed is part of this role of the nurse in community/public health.
COMMUNITY ORGANIZER
Working with people in communities and providing them ownership of their healthcare needs and to act collectively on their issues best captured by this role of the nurse in public health.
MANAGER/LEADER
Community and public health work deal with competing claims specifically on utilization of limited resources. Hence, the nurse employs principles of management to maximize resources effectively and efficiently. Budgeting, inventories, scheduling and staffing, conducting training sessions are likewise included under this role.
RESEARCHER/EPIDEMIOLOGIST
The nurse is regarded as the health monitor of the community. Together with the rural health midwife, they keep track of illnesses encountered in their areas of jurisdiction and submits report to health authorities as required by law. In the event of an outbreak, community/public health nurses work with other professionals and agencies in conducting investigation to identify etiology of epidemic and ultimately identify potential solutions to halt the progress of the problem. Apart from collecting actual data for research, the nurse utilizes research findings to promote evidence to convince decision makers to enact policies for health.
CLIENT ADVOCATE
The community/public health nurse takes a proactive stance in ensuring that the right to health of the population he/she works with is realized and protected. To do this, he/she engages stakeholders in clamoring and lobbying for policies that impact health of communities. The nurse in the field also initiates organizing activities to form coalitions and linkages to foster awareness of people to various health-related issues.
CORE PRINCIPLES IN COMMUNITY ORGANIZING
PEOPLE ORIENTED
People and means are ends of development
Community development is the process and the outcome
PARTICIPATIVE
Community is prime-mover & determinants rather than beneficiary of health efforts, critical for success.
Evident in involvement: well-informed, aware of their potentials for participation
Decision making is in hand of ordinary people not among elite
Distinction in not made among different groups & different personalities.
DEMOCRATIC
Empower disadvantaged population
Allows people to recognize, analyze needs & articulate aspirations
Decisions are from whole people/common people than the elite or leader alone
DEVELOPMENTAL
Directed in changing underlying situation
Through empowerment of marginalized people. Community gains insights, hones capabilities & develops. Later take leads in wholistic improvement of community.
PROCESS-ORIENTED
It is a process of change, allows community to internalize it & embrace process, requires time. It is dynamic with evolving community situation & monitoring & periodic review.
GOALS OF COMMUNITY ORGANIZING
PEOPLE’S EMPOWERMENT
process of community organizing allows people to develop their capacity to maximize control over situation. Start placing control over own hands.
BUILD PERMANENT STRUCTURES & PEOPLE’S ORGANIZATION
Establish & sustain permanent structures that will support their needs
IMPROVE QUALITY OF LIFE
Manifested by collective involvement in decision making & community action on matters that would impact their lives
COMMUNITY ORGANIZING PARTICIPATORY RESEARCH
History: COPAR
Introduced in 1990’s in social psychology, approach that encourages recipient of benefits (family, providers, policy makers) to partake in research & work together as full partners in community organizing
Later, it becomes an approach for community development, a tool for community organizing participatory action research or COPAR
A Participatory Action Research (PAR) Approach
BASIC VALUES IN COMMUNITY ORGANIZING
Human Rights
Universal principle anchored on belief of worth & dignity of people. Right of life, self-determination & development.
Social Justice
Equitable access to opportunities, equitable distribution of resources & power
Social Responsibility
People should reach out through & move jointly with others in meeting common needs & problems
CRITICAL ACTIVITIES IN COPAR
Integration
involves living with the people. Understanding their problem, undergoing their hardship, sharing their hopes & aspirations to help build mutual trust & cooperation
Social Investigation
also known as community study
systematic, scientific process of collecting & analyzing data to draw a clear picture of the community
Tentative Program Plan
Community chooses one issue to work to start community organizing
Groundwork
Going from place to place, motivating people on a one-on-one basis to act on the issue chosen
Meetings
People jointly ratify what have been decided individually
Gives people collective action and confidence
Role Play
Acting out meeting that would takes place amongst people and government representatives
Mobilization or Action
Actual exercise of people power
Evaluation
Measures the outcome of the activities versus objective
Reflections
Dealing with deeper, ongoing, concerns to look at positive values a community organizer is trying to build in the organization
METHODS USED IN COPAR
Action-Reflection-Action-Session
Consciousness Awareness
Participatory and Mass-Based
Group-Centered and not Leader-Oriented
COMPARISON OF TRADITIONAL RESEARCH APPROACH & COPAR
Traditional | COPAR | |
Decision-Making: | Top-Down (decision comes from the leaders) | Bottom-Up (decision comes from the people) |
Emphasis: | Expert/Nurse Driven Process Much premium is given on data or output | Community-Driven Process Premium is placed on the process |
Roles: | Nurse (N) is researcher, Community (C) as objects/subject of research – respondents Data Analysis (PAR) – by N & presented to people | N is facilitator; C as researcher Data Analysis – by community collectively |
Methodology: | Research Tool & Methodology are predetermined/ pre-packaged by the nurse | Research tool & method – identified and developed by community |
Output: | Submitted to agency, published, recommendations based on finding | Conclusion/ documentation made by C. leads to agreed C. actions/projects. Then whole research continues until it becomes part of C. life toward C development. C members formulates recommendations |
COMMUNITY DEVELOPMENT
It means improvement access to resource (including health resources) that will enable the people to improve their standards of living and overall quality life
Is the end goal of community organizing and all efforts towards uplifting the status of the poor and marginalized
Entails a process of assessment of the current situation, the identification of needs, deciding on appropriate courses of actions or response, mobilization of resources to address these needs, and evaluation by the people