Chapter 8- Health Team Communications
Key Vocab
Assessment- collecting information about the person
Evaluation- to measure if the goals in the planning step were met
Implementation- to perform or carry out nursing interventions in the care plan
Medical record- the legal account of a person’s condition and response to treatment and care. It is a permanent legal document
Nursing Diagnoses- a health problem that can be treated by nursing measures
Nursing Process- the method nurses use to plan and deliver nursing care. Its 5 steps are assessment, nursing diagnoses, planning, implementation, and evaluation. (ANDPIE)
Objective Data- information that is seen, heard, felt, or smelled by an observer; signs
Observation- using the 5 senses to collect information
Progress note- describe the care given and the person’s response
planning- setting priorities and goals
recording- the written account of care and observations ( charting)
reporting- the oral/vocal account of care and observations
Subjective data- things a person tells you, you cannot observe through your senses; symptoms
Key ABRVS
ADL- Activities of Daily Living
BMs- Bowel Movement
MDS- Minimum Data Set
Communication is needed for coordinated and effective care.. health team members share info on..
What was done for the person
What needs to be done for the person’s response to treatment
CNA- position the person, record the care you gave. The nurse reports
Parts of a Medical Record
Admission record | Legal name, birthdate, age, sex, address (legal info) |
Advance directives | Person’s wishes about end-of-life care |
health history |
|
Nursing assessment | Data collected by the nurse |
Nursing care plan | a guide to the person’s care |
Nursing progress notes | the care given and the person’s response, and progress |
flow sheets/ graphics | charting measurements |
medical administration record (MAR) electronic MAR | a record of drugs ordered, given, and not taken |
Physical Examination | info recorded during the physical exam. done by a doctor, APRN, or PA |
Orders | directions from the doctor, APRN, or PA about tests and care measures |
Progress Notes | Reports from the health team (doctor, etc) |
Lab results | results of blood, urine, or other bodily fluids/tissue |
Legal and Ethics
Agencies have policies on who can see them..
who records
When to record
ink color
abbreviations
How to make and sign entries
How to correct errors
You have a legal duty to keep information confidential. If not involved in a person’s care, you have no right to read the person’s chart. Doing so is an invasion of privacy
The Kardex
A kardex summarizes information in the medical record. It is not a permanent legal record, just a summary.
CNA’s roles
CNAs only do the implementation step in the “Nursing Process.”
Your assignment sheet will tell me what to do, and my observations will be used to help the nurse reevaluate
You do NOT assess
See how the person lies, sits, and walks
color of skin
Listen to the cough and breathe
Objective data are signs
Subjective data is symptoms (things you cannot observe through your senses)
Signs/ observations to report immediately
vital signs above or below normal rnages
bleeding
dizziness
change in a person’s mobility/ function
Diagnoses
Nursing Diagnoses- these deal with the person’s physical, emotional, social, and spiritual needs. These can change as information changes
Medical Diagnoses- the identification of a disease or condition given by a doctor
Long Term Care
The person and family have the right to take part in planning conferences
Interdisciplinary Care Planning (ICDP Conferences)- these are held to form care plans for new residents
Problem-focused conference- used when 1 problem affects a person’s care
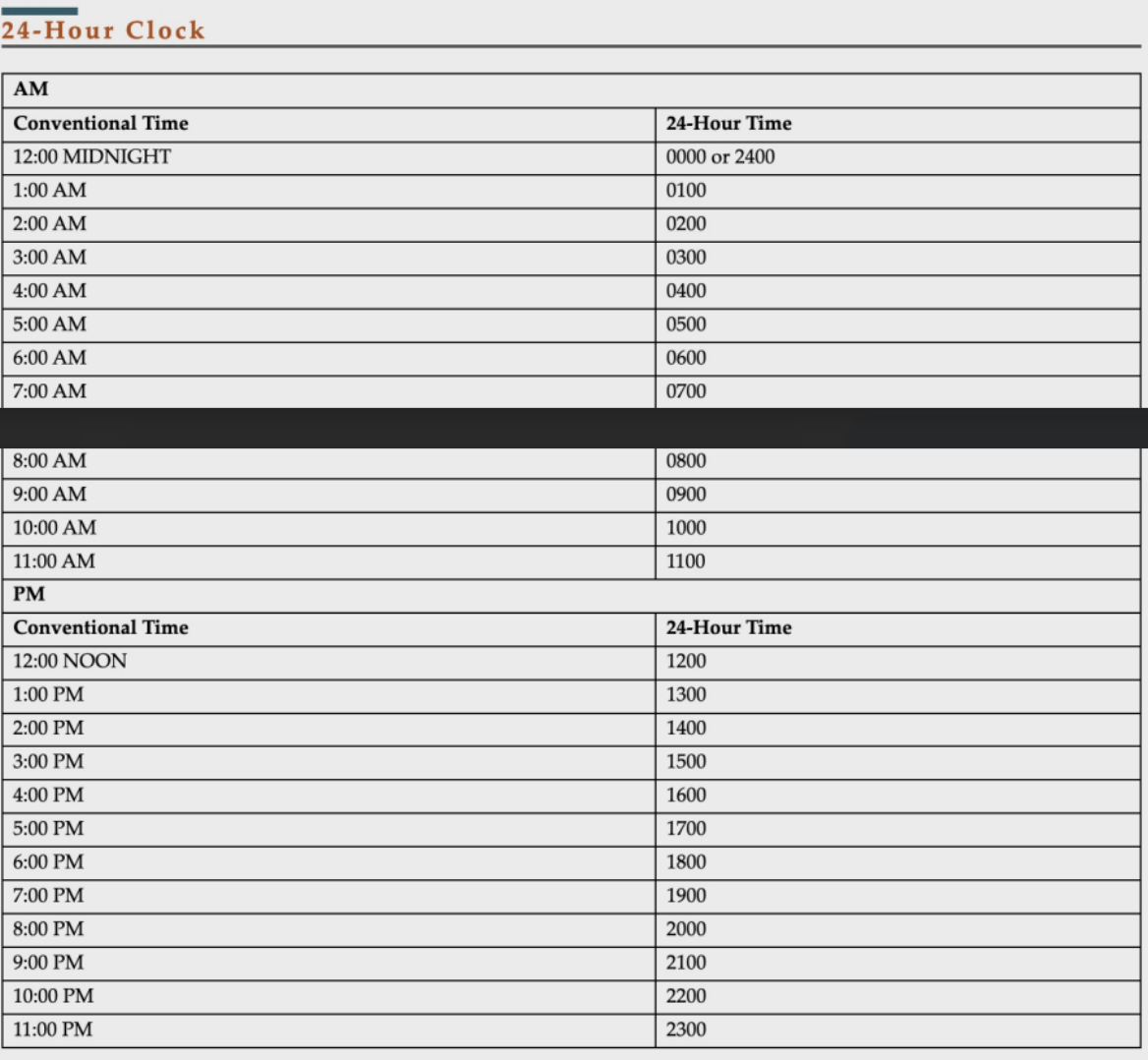
Reporting/ recording time
Must use military time!!!
Reporting
You report when…
When the nurses ask
Before leaving the unit
before the end of shit
End of shift report
The nurse reports about…
The care given
The care to give during other shifts
The person’s current condition
likely changes in the person’s condition
new or changed order
Rules for Recording
Include the date and time for each. (24-hour time)
Correct spelling, grammar, and punctuation
Record only what YOU did/observed yourself
be accurate, concise, and factual
If quoting, use the person’s EXACT words with quotations
chart that you told the nurse, what you said, and what time you said it
record safety measures (call light in reach, etc)
Sign and save all entries
On the computer…
Only log in with YOUR username and password. Do not use another person’s.
On paper…
Do not use whiteout
If you make a mistake, draw a line through the incorrect part
Date and initial the line
Electronics
DO NOT tell anyone your username or password.
Log off after making an entry
If documents need to be shredded, place such documents in a wastebasket marked (Confidential information)
Do not email information
Answering Phones
Hospital Setting
Answer the call after the 1st ring if possible. Be sure to answer after the 4th ring
Give a courteous greeting
Note this info:
caller’s name and phone number (area code + extension number)
the date and time
Who the message is for
Do not put callers with an emergency on hold
Home Care
Answer the patient’s phone with “hello” to protect the patient
Review Questions
F
T
F
T
T- F
T
F
F
T
F
D
C
C
A
D
A
C
A
B
C
B
D
A
A
C
24/25 = 96% = A