Pharmacology - lecture 15 - Drug Treatment of Depression
Learning Outcomes
After this lecture, students should be able to:
Define clinical depression and describe key symptoms.
Outline the "monoamine theory of depression" and explain the clinical actions of current antidepressant drugs including MAOIs, TCAs, SSRIs, and SNRIs.
List the main problems with the monoamine theory of depression.
Recognize the challenges associated with the development of drugs to treat psychiatric disorders, including depression.
Clinical Depression
Also known as major depressive disorder.
Classification: Psychiatric, affective disorder.
Prevalence: Second leading cause of disability in adults (following cardiovascular disease).
Age of Onset: Average age is mid/late 30s.
Gender Ratio: F:M ratio is approximately 2:1.
Sub-classes:
Endogenous: No obvious stress trigger.
Reactive: Identifiable stress trigger.
Diagnosis: Continuation of symptoms for more than 2 weeks.
Symptoms of Clinical Depression
Emotional Symptoms:
Sadness or low mood.
Loss of enjoyment in previously pleasurable activities (anhedonia).
Low self-esteem, feelings of hopelessness, worthlessness, and guilt.
Suicidal thoughts.
Biological Symptoms:
Significant changes in weight (either gain or loss).
Sleep disturbances (insomnia or excessive sleep).
Fatigue or loss of energy.
Cognitive slowness or lethargy.
Diagnosis Requirement: At least 5 symptoms must be present.
Neurobiological Basis of Depression
Regions Involved:
Anterior cingulate cortex
Cortical and sub-cortical limbic regions:
Hippocampus: Involved in memory processing and emotional regulation.
Hypothalamus: Regulates mood, appetite, and energy levels.
Amygdala: Regulates emotions such as fear and aggression.
Prefrontal cortex: Cognitive processing related to feelings of worthlessness and guilt, influences personality and social behavior.
History of Antidepressants
Iproniazid: First antidepressant discovered by chance during tuberculosis treatment.
Initially did not cure TB but improved patients' mood, appetite, and sleep.
Mechanism: Blocks the enzyme monoamine oxidase (MAO) which breaks down key neurotransmitters.
Monoamine Hypothesis of Depression
Proposed by Schildkraut (1965):
Suggests that a decrease in monoaminergic transmission (serotonin, norepinephrine, dopamine) is responsible for depression.
These pathways are crucial for regulating mood and behavior.
Monoamines innervate forebrain areas and frontal cortex involved in mood/behaviour.
Evidence for and Against Monoamine Hypothesis
For:
Lower levels of monoamine metabolites found in the cerebrospinal fluid (CSF) of depressed patients.
Mood improvement is observed with drugs that increase levels of norepinephrine, serotonin, and dopamine.
Reduced reuptake
Reduced intracellular breakdown
Monoamine depletion (e.g., from reserpine) can induce depressive symptoms.
Against:
Some drugs that elevate monoamine levels do not show antidepressant effects (e.g., amphetamine, cocaine).
Monoamine levels increase quickly upon antidepressant administration, but clinical improvement takes 2-4 weeks.
Suggestion that initial monoamine increases lead to secondary neuroplastic changes over time.
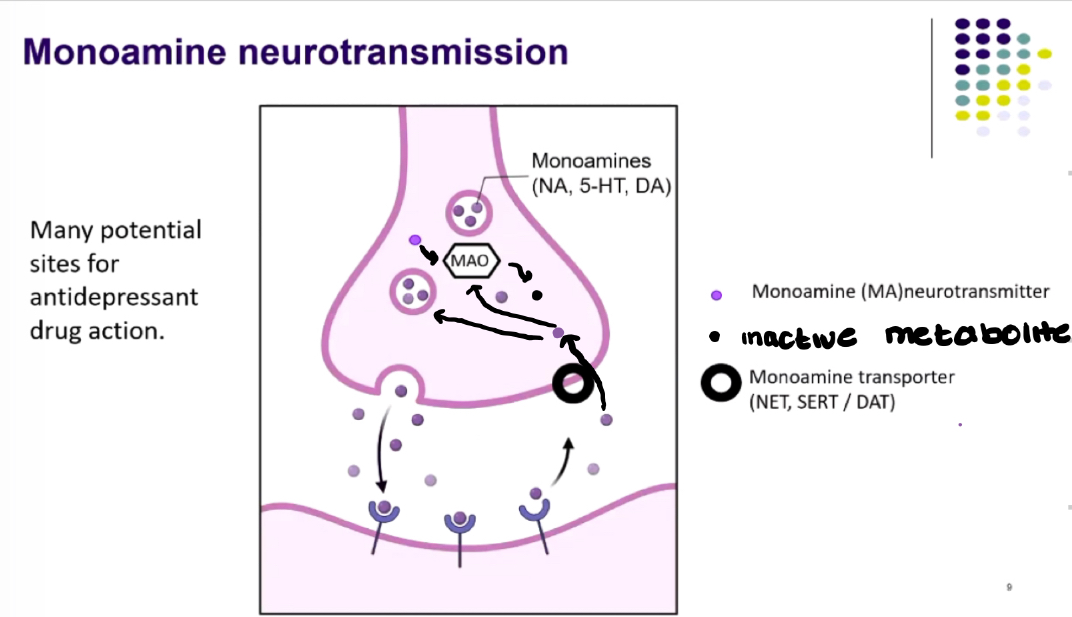
Monoamine Neurotransmission
Monoamines: Norepinephrine (NA), serotonin (5-HT), dopamine (DA).
Inactive metabolites arising from these neurotransmitters are important indicators.
Impacts of drugs occur at various sites affecting neurotransmitter transporters and receptors.
Development of Antidepressants
All antidepressants are rooted in the monoamine hypothesis, showing similar clinical efficacy.
Effectiveness varies, with 30-40% of patients not improving.
Choice of drug influenced by:
Patient's treatment history.
Suicide risk assessment.
Profile of adverse effects.
Types of Antidepressants
MAO Inhibitors (MAOIs): Phenelzine
Mechanism: Blocks breakdown of monoamines, allowing monoamines to build up.
Increase of post-synaptic monoamine receptors activated.
Dietary restrictions: Avoid tyramine-rich foods to prevent hypertensive crisis.
Usage: Prescribed when other types have failed.
Tricyclic Antidepressants (TCAs): Amitriptyline
Mechanism: Blocks reuptake of monoamines, increasing levels in the synaptic cleft.
Currently more used for chronic pain treatment due to dangerous cardiovascular side effects.
Serotonin and Noradrenaline Reuptake Inhibitors (SNRIs): Venlafaxine
Mechanism: Selectively blocks reuptake of NA and 5-HT.
Side effects: Panic attacks and increased blood pressure.
Selective Serotonin Reuptake Inhibitors (SSRIs): Fluoxetine
Blocks reuptake of 5-HT.
Most prescribed class of antidepressants.
Highly selective for serotonin reuptake.
Noradrenaline Reuptake Inhibitors (NRIs): Reboxetine
Mechanism: Selectively blocks reuptake of NA.
Usage: Generally reserved for cases where SSRIs are ineffective.