Somatic symptom and related disorders
Somatic symptom and related disorders Chapter 8. Somatic Symptom and Dissociative Disorders
Medically unexplained symptoms
Somatic symptom disorder
The experience of one or more debilitating somatic symptoms
Symptoms are accompanied by abnormal thoughts, feelings and behaviours
These abnormal reactions include disproportionate and persistent thoughts about the seriousness of symptoms; persistently high anxiety about one’s health or symptoms; and spending excessive time and energy over health concerns (e.g., excessive healthcare utilisation)
Conversion disorder
Disturbance in motor or sensory functioning
Not consistent with any recognised medical condition
Causes significant distress and/or impairment
Epidemics of conversion disorder, ‘mass hysteria’, occur periodically
One person becomes sick and the experience of symptoms, beliefs about the cause of symptoms, and anxiety about the symptoms generalises to others
Illness anxiety disorder
Preoccupation with having or getting a serious illness
Somatic symptoms not prominent
High levels of health anxiety and excessive health-related behaviours
The individual may worry about a particular disease/illness, or a number of different types
If a medical condition is present, the level of preoccupation is excessive
The treatment of somatic symptom and related disorders
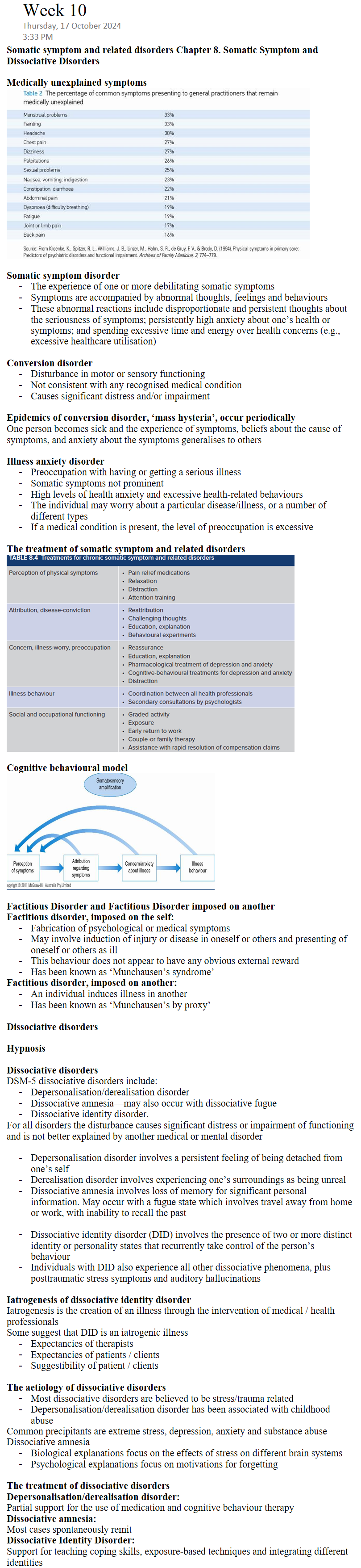
Cognitive behavioural model
Factitious Disorder and Factitious Disorder imposed on another
Factitious disorder, imposed on the self:
Fabrication of psychological or medical symptoms
May involve induction of injury or disease in oneself or others and presenting of oneself or others as ill
This behaviour does not appear to have any obvious external reward
Has been known as ‘Munchausen’s syndrome’
Factitious disorder, imposed on another:
An individual induces illness in another
Has been known as ‘Munchausen’s by proxy’
Dissociative disorders
Hypnosis
Dissociative disorders
DSM-5 dissociative disorders include:
Depersonalisation/derealisation disorder
Dissociative amnesia—may also occur with dissociative fugue
Dissociative identity disorder.
For all disorders the disturbance causes significant distress or impairment of functioning and is not better explained by another medical or mental disorder
Depersonalisation disorder involves a persistent feeling of being detached from one’s self
Derealisation disorder involves experiencing one’s surroundings as being unreal
Dissociative amnesia involves loss of memory for significant personal information. May occur with a fugue state which involves travel away from home or work, with inability to recall the past
Dissociative identity disorder (DID) involves the presence of two or more distinct identity or personality states that recurrently take control of the person’s behaviour
Individuals with DID also experience all other dissociative phenomena, plus posttraumatic stress symptoms and auditory hallucinations
Iatrogenesis of dissociative identity disorder
Iatrogenesis is the creation of an illness through the intervention of medical / health professionals
Some suggest that DID is an iatrogenic illness
Expectancies of therapists
Expectancies of patients / clients
Suggestibility of patient / clients
The aetiology of dissociative disorders
Most dissociative disorders are believed to be stress/trauma related
Depersonalisation/derealisation disorder has been associated with childhood abuse
Common precipitants are extreme stress, depression, anxiety and substance abuse
Dissociative amnesia
Biological explanations focus on the effects of stress on different brain systems
Psychological explanations focus on motivations for forgetting
The treatment of dissociative disorders
Depersonalisation/derealisation disorder:
Partial support for the use of medication and cognitive behaviour therapy
Dissociative amnesia:
Most cases spontaneously remit
Dissociative Identity Disorder:
Support for teaching coping skills, exposure-based techniques and integrating different identities