Innate Immunity: Recognition, Phagocytosis, Inflammation, and Lymphatic Interface and an Overview of Adaptive Immunity.
Introduction
This lecture delves into the core mechanisms of the innate immune system, the body's first and rapidly responding line of defense. We will cover:
The distinction between innate and adaptive immunity.
An overview of the key cellular players derived from hematopoietic stem cells.
The critical process of phagocytosis by cells like neutrophils and macrophages.
The molecular basis of pathogen and danger recognition via Pattern Recognition Receptors (PRRs) detecting PAMPs and DAMPs.
Detailed insights into major PRR families including Toll-like Receptors (TLRs), NOD-like Receptors (NLRs), and cytosolic sensors for viral nucleic acids.
The inflammatory response: its initiation, vascular and cellular components, key mediators, and resolution.
The role of the lymphatic system in immune surveillance and linking innate to adaptive responses.
I. Overview: Innate vs. Adaptive Immunity
The immune system is broadly divided into two interconnected branches:
Innate Immunity:
Speed: Rapid onset (minutes to hours).
Specificity: Relatively non-specific; recognizes broad classes of pathogens or danger signals.
Receptors: Germline-encoded pattern recognition receptors (PRRs).
Components: Cellular (phagocytes, granulocytes, NK cells, mast cells, dendritic cells, ILCs) and humoral (complement, acute phase proteins, antimicrobial peptides, cytokines, chemokines).
Memory: Generally lacks long-lasting immunological memory.
Function: Provides immediate defense, contains infections, and signals to initiate and shape the adaptive immune response. Inflammatory mediators can be directly or indirectly toxic to pathogens.
Adaptive Immunity:
Speed: Slower deployment (typically 7-10 days for a primary response).
Specificity: Highly specific; recognizes unique antigens on pathogens.
Receptors: Antigen receptors (TCRs on T-cells, BCRs/Antibodies on B-cells) are generated by somatic gene rearrangement, creating vast diversity.
Components: Primarily T-lymphocytes and B-lymphocytes.
Memory: Characterized by immunological memory, leading to faster and stronger responses upon re-exposure to the same pathogen.
Function: Provides targeted and powerful elimination of pathogens, and long-lasting protection.
Cellular Origins: All immune cells originate from Hematopoietic Stem Cells in the bone marrow, which differentiate into common myeloid and lymphoid progenitors.
Myeloid Progenitor: Gives rise to erythrocytes, megakaryocytes (platelets), neutrophils, eosinophils, basophils, monocytes (which become macrophages and some dendritic cells), and mast cells.
Lymphoid Progenitor: Gives rise to B-cells (which differentiate into plasma cells and memory B-cells), T-cells (CD4+ helper T-cells, CD8+ cytotoxic T-cells, regulatory T-cells), NK cells, and Innate Lymphoid Cells (ILCs).
II. Phagocytosis: Engulfment and Destruction
Phagocytosis ("cell eating") is a primary effector mechanism of innate immunity carried out by phagocytic cells, predominantly neutrophils and macrophages.
Steps in Phagocytosis:
Recognition and Attachment:
Pathogens are recognized either directly by PRRs on the phagocyte or indirectly through opsonins (e.g., complement C3b, antibodies).
Binding of opsonized bacteria (e.g., coated with C3b) to phagocyte receptors (e.g., CR1 for C3b) occurs. However, C3b binding to CR1 alone may not be sufficient to induce phagocytosis; co-stimulation, such as C5a binding to its C5a receptor (C5aR), is often required to fully activate the phagocyte for engulfment.
Engulfment: The phagocyte extends pseudopods around the bacterium or particle, internalizing it into a membrane-bound vesicle called a phagosome.
Phagolysosome Formation: The phagosome fuses with lysosomes (granules containing digestive enzymes and antimicrobial substances) to form a phagolysosome.
Killing and Digestion: Within the phagolysosome, the microbe is killed and degraded by:
Low pH: The environment becomes acidic.
Antimicrobial peptides: Lysozyme and defensins.
Enzymes: Various hydrolytic enzymes.
Reactive Oxygen Species (ROS): Produced by the NADPH oxidase enzyme complex (respiratory burst), generating superoxide anion (O2−), hydrogen peroxide (H2O2), and hypochlorite (HClO− via myeloperoxidase).
Reactive Nitrogen Species (RNS): Production of nitric oxide (NO) by iNOS, which can react with superoxide to form peroxynitrite (ONOO−).
Exocytosis: Residual waste material is expelled from the cell.
NETosis:
A specialized form of cell death in neutrophils where they release Neutrophil Extracellular Traps (NETs) – networks of DNA, histones, and antimicrobial proteins – that trap and kill pathogens.
Additional Roles of Macrophages:
Besides phagocytosis, macrophages are key in antigen presentation to T-cells (linking to adaptive immunity) and cytokine release to modulate the immune response.
III. Pattern Recognition: Sensing Danger
The innate immune system distinguishes pathogens and danger signals from host components through Pattern Recognition Receptors (PRRs).
PAMPs (Pathogen-Associated Molecular Patterns): Conserved molecular structures found on microbes but not host cells (e.g., LPS, peptidoglycan, flagellin, viral RNA/DNA).
DAMPs (Damage-Associated Molecular Patterns) / Alarmins / Danger Signals: Endogenous molecules released from damaged or dying host cells (e.g., ATP, uric acid, HSPs, self DNA/RNA in abnormal locations, granule contents). The "Danger Model" (Polly Matzinger) suggests the immune system responds primarily to danger signals. An effective immune response often requires both PAMPs and DAMPs for full dendritic cell maturation.
Major PRR Families:
A. Toll-like Receptors (TLRs):
Family of ~10 transmembrane receptors in humans, expressed on immune and non-immune cells.
Structure: Leucine-rich repeat (LRR) extracellular domain (for PAMP recognition) and an intracellular Toll/IL-1 Receptor (TIR) domain (for signaling). They function as homo- or hetero-dimers.
Ligands & Location:
Cell Surface TLRs:
TLR1/TLR2: Triacyl lipopeptides (bacterial).
TLR2/TLR6: Diacyl lipopeptides, LTA, Zymosan (fungal).
TLR2: Peptidoglycan.
TLR4 (with MD-2/CD14): LPS (Gram-negative bacteria).
TLR5: Flagellin (bacterial).
TLR10: Potentially anti-inflammatory, recognizes components from Listeria, Influenza.
Endosomal TLRs:
TLR3: dsRNA, siRNA (viral, self RNA).
TLR7 & TLR8: ssRNA (viral).
TLR9: CpG-DNA (bacterial/viral).
Signaling Pathways & Outcomes:
MyD88-dependent pathway (all TLRs except TLR3): Activates NF-κB and MAPKs (p38, JNK). Leads to production of pro-inflammatory cytokines (TNF, IL-1, IL-6, IFNγ), chemokines (e.g., CXCL8/IL-8), defensins, and iNOS. Primarily for bacterial and some viral responses.
TRIF-dependent pathway (TLR3 and endosomal TLR4): Activates IRF3. Leads to production of Type I Interferons (IFNα, IFNβ), crucial for antiviral responses.
B. Cytosolic PRRs: Detect intracellular pathogens or danger signals.
RIG-I-like Receptors (RLRs):
RIG-I and MDA5 detect viral dsRNA or ssRNA in the cytoplasm.
Signal via MAVS (on mitochondria) to activate TRAF3, IRF3/7 (for Type I IFN production) and NF-κB (for pro-inflammatory cytokines like TNF, IL-6).
Cytosolic DNA Sensors:
cGAS (cyclic GMP-AMP Synthase): Detects cytosolic DNA.
Activates STING (Stimulator of Interferon Genes) pathway, leading to IRF3 activation (Type I IFNs) and NF-κB activation (TNF, IL-6).
C. NOD-like Receptors (NLRs):
Cytosolic PRRs sensing intracellular PAMPs or DAMPs. Subfamilies include NLRA, NLRB, NLRC (e.g., NOD1, NOD2 for peptidoglycan fragments), and NLRP (NLRP1-14).
NLRP3 Inflammasome:
NLRP3, upon sensing various PAMPs or DAMPs, assembles with ASC (adaptor) and pro-caspase-1 to form the NLRP3 inflammasome.
Active Caspase-1 cleaves pro-IL-1β and pro-IL-18 into their mature, active forms.
Caspase-1 can also mediate pyroptosis, a pro-inflammatory form of cell death.
IV. Inflammation: The Body's Coordinated Response
Inflammation is a non-specific, localized, and complex biological response of tissues to harmful stimuli such as pathogens, damaged cells, or irritants. It is a protective mechanism aimed at eliminating the initial cause of injury, removing necrotic cells/tissues, and initiating repair and recovery. However, it can be harmful if uncontrolled.
Inflammation vs. Infection: Inflammation is the immunovascular response, while infection describes the interaction between an invading pathogen and this response. Inflammation can occur without infection (e.g., atherosclerosis, hypersensitivity).
Cardinal Signs of Inflammation (Celsus & Galen):
Rubor (Redness): Due to increased blood flow.
Tumor (Swelling): Due to accumulation of exudate fluid.
Calor (Heat): Due to increased blood flow.
Dolor (Pain): Due to release of chemical mediators (e.g., histamine, bradykinin) that sensitize nerve endings.
Functio laesa (Loss of function): Due to combined effects of pain, swelling, tissue damage. (Also known by the acronym PRISH: Pain, Redness, Immobility (loss of function), Swelling, Heat).
Process of Acute Inflammation:
Initiation:
Resident cells (mast cells, macrophages, dendritic cells) recognize PAMPs and DAMPs via PRRs.
Release of initial inflammatory mediators like histamine and bradykinins.
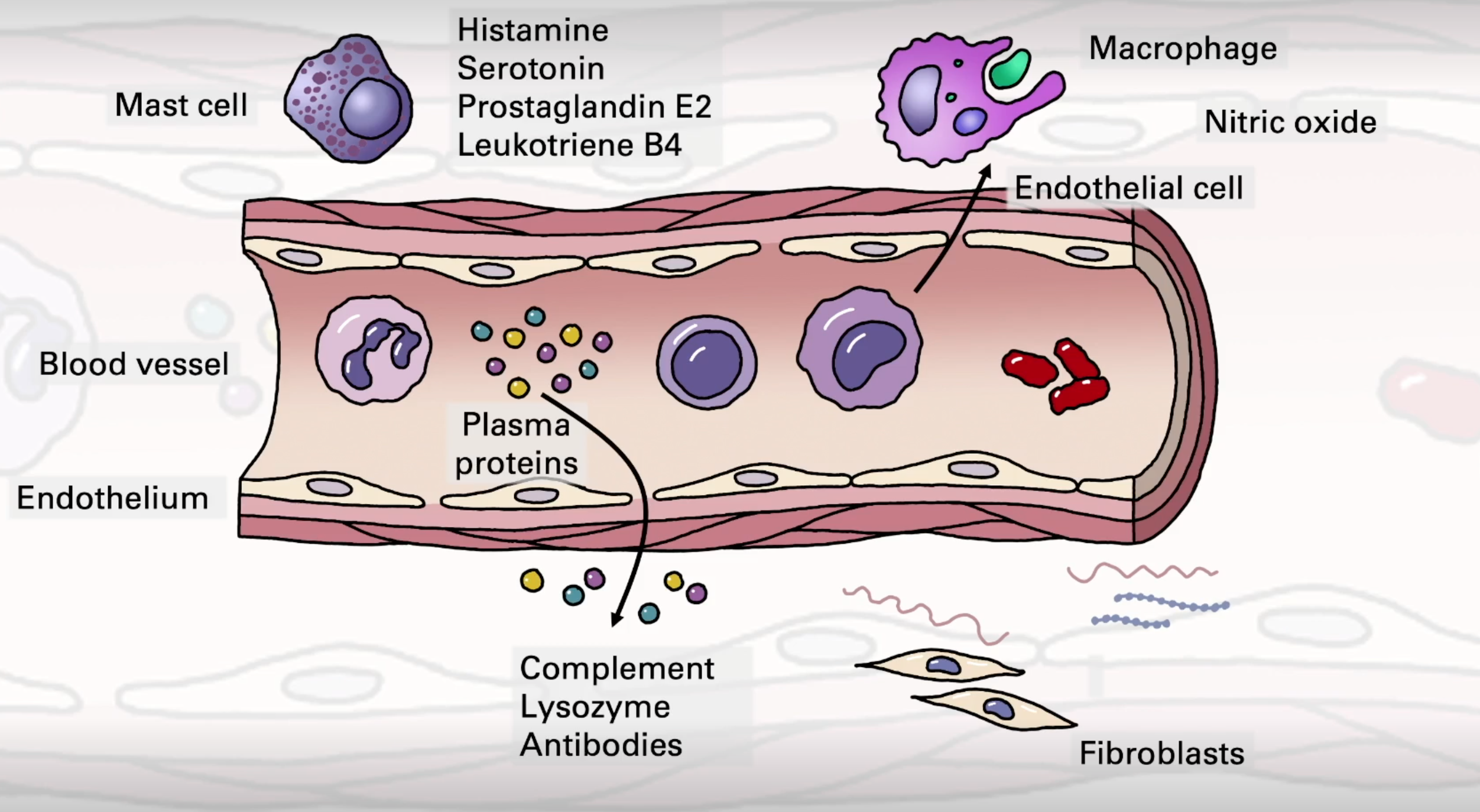
Vascular Components/Changes:
Vasodilation: Increased blood vessel diameter leads to increased blood flow (causing redness/rubor and heat/calor). Mediated by histamine, serotonin, prostaglandin E2, nitric oxide.
Increased Vascular Permeability: Endothelial cells contract, widening intercellular gaps, leading to exudation of protein-rich fluid (plasma proteins like complement, lysozyme, antibodies, clotting factors, kinins) from blood vessels into the tissues (causing swelling/tumor). Mediated by histamine, C5a, Leukotriene B4 (LTB4).
Blood Stasis: Loss of fluid from vessels leads to increased concentration of red blood cells (RBCs) and slower blood flow. Stasis forces leukocytes towards the vessel walls (margination). In normal flow, neutrophils are in the axial stream; stasis allows for pavementing of neutrophils and adhesion of platelets.
Cellular Components/Leukocyte Recruitment (Extravasation Cascade):
Stimulus (e.g., bacteria) and mediators (cytokines like TNF, IL-1 from macrophages/mast cells; histamine) activate endothelial cells.
Margination: Leukocytes (especially neutrophils) move from the central axial flow to the periphery of blood vessels due to blood stasis.
Rolling: Leukocytes loosely adhere to activated endothelial cells via selectins (P-selectin, E-selectin on endothelium) binding to sialyl-Lewis X on neutrophils. Mediators like histamine, C5a, LTB4, PGE2, and bacterial products promote this.
Adhesion (Firm Adhesion): Stronger adhesion mediated by integrins (e.g., LFA-1, Mac-1, VLA-1 on leukocytes) binding to adhesion molecules like ICAM-1 and VCAM-1 on activated endothelium.
Diapedesis (Transmigration): Leukocytes squeeze between endothelial cells to enter the tissue, mediated by molecules like PECAM-1/CD31.
Chemotaxis: Leukocytes migrate within the tissue towards the site of injury/infection along a chemotactic gradient of chemoattractants (e.g., C5a, LTB4, bacterial products, chemokines like IL-8).
Phagocytosis and Clearance: Recruited phagocytes (neutrophils arrive first, followed by monocytes/macrophages) engulf and destroy pathogens and remove dead cells and debris.
Repair and Resolution:
Once the threat is eradicated, the inflammatory response is actively terminated to protect surrounding tissue and restore homeostasis.
Mechanisms include: short half-life of inflammatory mediators, apoptosis of inflammatory cells (especially neutrophils), and a switch to anti-inflammatory cytokine/chemokine production.
Repair processes involving fibroblasts and extracellular matrix deposition begin.
Leukocyte Adhesion Deficiency (LAD):
Rare genetic disorders (e.g., LAD1 due to ITGB2 gene mutation encoding integrin β2 subunit) cause defects in neutrophil adhesion and transmigration.
Leads to recurrent severe bacterial infections because leukocytes cannot effectively reach infection sites; leukocyte arrest is impaired, and no diapedesis occurs. Delayed umbilical cord sloughing is a characteristic sign.
Acute Phase Response (Systemic Effects of Inflammation):
Fever: Body temperature >37.8°C, induced by pyrogenic cytokines like IL-1, TNF-α, IL-6.
Increased blood pressure / heart rate.
Chills, Anorexia (loss of appetite).
Acute Phase Protein Production by Liver: Stimulated by IL-6, leading to elevated C-Reactive Protein (CRP) and increased Erythrocyte Sedimentation Rate (ESR) – common clinical markers of inflammation.
Leukocytosis (Increased White Blood Cell Count):
Neutrophilia (↑ neutrophils) – typical of bacterial infections.
Lymphocytosis (↑ lymphocytes) – typical of viral infections.
Eosinophilia (↑ eosinophils) – typical of parasitic infections or allergy.
Acute vs. Chronic Inflammation:
Feature | Acute Inflammation | Chronic Inflammation |
|---|---|---|
Onset | Rapid (minutes/hours) | Slow (weeks/months) |
Duration | Short (days/weeks) | Long (months/years) |
Key Cells | Predominantly Neutrophils | Predominantly Monocytes/Macrophages, Lymphocytes |
Outcome | Resolution, protein exudate, apoptosis | Necrosis, Fibrosis (scarring), Angiogenesis |
Chronic Inflammation Causes: Persistent injury (e.g., ulcer, TB infection), prolonged toxic agent exposure (e.g., silica), autoimmune diseases (e.g., Rheumatoid Arthritis/RA, Systemic Lupus Erythematosus/SLE).
Chronic inflammation is implicated in a wide range of diseases, including cancer, arthritis, neurological diseases (e.g., Alzheimer's), diabetes, cardiovascular disease, and pulmonary disease.
V. The Lymphatic System: Interface for Immune Responses
(Briefly recapping relevant anatomy from "09 Anatomy of the immune system - lymphatics - Slides.pptx")
Primary Lymphoid Organs: Bone marrow and Thymus – sites of lymphocyte development and maturation.
Thymus: Contains cortex and medulla; site for thymocyte development involving interactions with cortical and medullary epithelial cells, dendritic cells, and macrophages.
Secondary Lymphoid Organs & Tissues: Lymph nodes, Spleen, Mucosa-Associated Lymphoid Tissues (MALTs - e.g., Peyer's patches in the gut, tonsils, adenoids, NALT, BALT) – sites where innate and adaptive immune responses are initiated.
Lymph Nodes: Filter lymph; organized into cortex (B-cell follicles, germinal centers), paracortex (T-cells, dendritic cells), and medulla (macrophages, plasma cells). Afferent lymphatics bring lymph and antigen-presenting cells in; efferent lymphatics allow cells and lymph to exit.
Spleen: Filters blood; white pulp contains PALS (T-cells), follicles (B-cells), and marginal zone. Red pulp involved in RBC clearance.
MALT (e.g., Peyer's Patch): Contains M-cells for antigen sampling from lumen, B-cell follicles/germinal centers, and T-cell zones. Similar structures (NALT, BALT) exist in airways.
Lymphatic Vessels: Network for lymph circulation, returning fluid and cells to the blood. Lymphatic capillaries have overlapping endothelial cells forming one-way valves.
Role in Linking Innate and Adaptive Immunity: Dendritic cells, after capturing antigens in peripheral tissues (an innate process), travel via lymphatic vessels to regional lymph nodes. Here, they present processed antigens to T-lymphocytes, initiating specific adaptive immune responses. This highlights the crucial interplay between the innate recognition and response system and the highly specialized adaptive immune system.
Further Reading
The immune system consists of innate and adaptive components that work synergistically to protect against pathogens (Marshall et al., 2018). Innate immunity provides rapid, non-specific responses using pattern recognition receptors to detect conserved microbial structures (Janeway & Medzhitov, 2002). This initiates inflammation, phagocytosis, and cytokine production (Kiboneka, 2021). Adaptive immunity, mediated by T and B lymphocytes, offers antigen-specific responses and immunological memory (Yates & Lyczak, 2004). The interplay between innate and adaptive immunity is crucial, with innate immune cells acting as antigen-presenting cells to activate adaptive responses (Clark & Kupper, 2005). Toll-like receptors play a key role in pathogen recognition and initiating immune responses (Janeway & Medzhitov, 2002). Metabolic reprogramming during immune responses leads to increased reactive oxygen species production, affecting immune cell function (Sun et al., 2020). Understanding these interactions is essential for developing targeted therapies for immunological and inflammatory diseases (Dempsey et al., 2003; Medzhitov & Janeway, 1998).