Alterations in cardiovascular
anatomy/physiology
Point of maximum impulse (PMI)= apex of heart → 5th ICS in left midclavicular line
3 layers: endo (also lines valves) → myo → epi (serous)
→ then pericardium =
visceral
parential = is attached to great vessels, diaphragm, sternum, vertebrae = heart attached to thorax
pericardial space w/ serous fluid
vessels
layers of vessels → tunica
adventitia: outside → connective tissue, nerve, vessel
media: [sub]/endothelium, elastica lamina
intima: smooth muscle, endothelial squamous
function of vessels:
arteries: high BP from heart
→ arterioles → capillaries (gas exchange, nutrient/waste transfer) → venules
veins: reservoir of blood and low BP to heart
heart blood supply:
coronary arteries (CA): Left anterior descending, (L)
circumflex, (L/R) coronary artery, Right marginal artery
during diastole → blood to CA
function
electrophysiology: SA → AV - (slight delay to contract ventricles) → bundle of his → Purkinjean fibers
hemodynamics: systole, diastole
CO: amount of blood eject from ventricle/ min (L/min)
vasocontraction, artery compliance, afterload, blood entering to heart
normal = 5-6L/min
CO= SV x HR
preload: can be measure w/ pulmonary capillary wedge (PCW)
afterload: ~ to BP
contractability: influences SV → use inotropic of SNS stim
heart sounds:
S1: close MV and TV → open AV and PV (systole)
S2: close AV and PV → open MV and TV (diastole)
S3: normal in children, HF for >40
venticular gallop
loud DUB after S2: lubdubDUB
S4: atrial gallop
LUBlubdub
low ventricular compliance by HTN, aortic stenosis, CAD, cardiomyopathy
murmur: turbulence WHOOSH
systolic between S1 and S2
diastolic between S2 and S1
pericardial friction rub: left sternal border
inflammation, infection, infiltration
GRATING
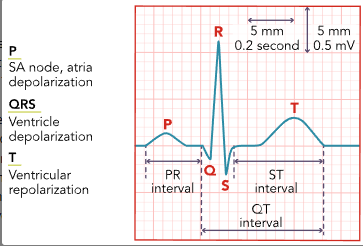
Cardiac rhythms
depolarization (contract) → repolarization (relax)
ECG identify areas w/ low perfusion
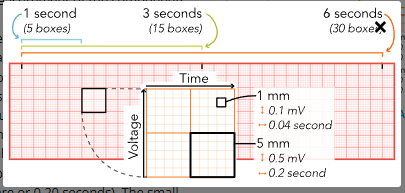
ECG Analysis
Calculate HR
R to R intervals = count large square then divide by 300 (for ventricular rhythm)
P to P intervals = atrial rhythm
count all QRS in 6sec strip x 10= bpm
Determine if heart rhythm is regular.
R to R: P to P = if same is reg if not then irreg
Assess for P waves.
more than one before QRS, no P wave, or diff P waves
disturbance between SA and AV
Measure PR interval.
beginning of P wave → beginning of QRS
0.12-0.2
count small boxes then x 0.04sec
Measure duration of QRS complex.
until beginning of ST segment
0.06-0.1
premature ventricular contractions (PVC)
unifocal =same shape in same site
or multifocal = diff shape from diff site
bigeminy( every other), trigeminy, quadrigeminy)
more frequently more lethal
Assess ST segment.
1 small box change (1mm) in elevation or depression in the isoelectric line → E/I or low cardiac perfusion
Observe for changes in T wave.
peak = E/I (hyper K)’
inversion = ischemia or PE
Measure length of QT interval.
means length of time of ventricular repolarization
no more than 0.45
lethal dysrhythmias → QT prolonged
Interpret the rhythm.
sinus bradycardia
NSR but lower than 60
causes:
people w/ exercise, or Afib or Brugada syndrome
by MI, sleep apnea, ICP
low metabolic need : eating disorder, hypothyroidism
Vagus stim
Lyme disease, typhoid fever, malaria, or Rocky Mountain spotted fever
meds:
Parasympathomimetics (acetylcholine)
Beta blockers (metoprolol)
Digitalis glycosides (digoxin)
Calcium channel blockers (diltiazem)
Antiarrhythmics (amiodarone)
Chemotherapy agents (thalidomide)
Lithium
s/s: no s/s → dizzy, syncopal ep, AMS, SOB, diaphoresis, exercise-fatigue
lab/dx:
E/I: Ca/ Mg, troponin, TH, check U/A or blood for illicit drug
nurse intervention:
hold BB, fall precaution, toxin or infectious exposure
s/s = monitor ECG, adm fluids,
tx:
IV atropine q 3-5mins but not over 3mg
temporary, transcutaneous pacemakers
sinus tachy
Excessive SNS → prologued → low CO
100<x<150
causes:
fluid loss/ excess
pain, fever, shock, anxiety, stress
MI, hyperTH
atropine, catecholamines, theophylline, illicit (cocaine, amphetamine), caffeine, nicotine
s/s:
palpitation, dizzy, ortho hypoTN
can report high temp, SOB, angina
lab/dx:
CBC: infection, anemia
BMP, heart enzymes, drug screen
ABG, ECG, D-dimer, chest radio
24-hr ECG for abnormal activity
tx:
teach vagal stim
IV adenosine: determine if NSR or supraventicular
nausea, feeling of doom, sweating, numbness
BB
catheter ablation: destroys abnormal excited cardiac cells
performed using sedation
inserted in femoral → heart
postop = monitor bleeding, thrombosis, hematoma
keep extremity straight at all time
Premature Ventricular contraction (PVC)
early electrical impulses from irritated ventricular cells
QRS is wider and occur early in cardiac cycle
causes:
HTN
MI, Cardiomyopathy, Ventricular tachycardia
COPD, Pulmonary hypertension
Sleep apnea
Electrolyte imbalances: low K/Mg
Thyroid disorders
Caffeine sensitivity, :Nicotine, alcohol, or illicit drug use
s/s:
inc palpitations lying down at night and sleep disturbances
palpitations
lightheadness
chest pain or SOB
lab/dx:
BMP, TH
ECG: NRS but w/ premature, widen (>0.12) QRS
hiden P wave,
24hr monitor = 24-48hr, with diary to note s/s
don’t shower
determine heart sounds
tx:
metoprolol and carvedilol
flecainide, propafenone, amiodarone = antiarrhythmics (close monitor for kidney and liver)
catheter ablation after 30days
tx:
>50 = annual cardiac health screen
Premature Atrial Contractions (PACs)
benign w/ irritated atrial
causes: unknown
MI, HTN, DM, CHF
digoxin, BB, chemo, antidepressant
s/s: no s/s, only anxiety from dx
may report flutter or SOB w/ exercise
lab/dx:
ECG: normal NSR but some P wave unidentifiable and PR interval shorten (<0.12)
BMP
tx:
lifestyle modification → contact HCP if SOB or angina
if frequent PAC → BB
1st degree heart block
SA→ AV delay = PR >0.2sec

cause:
age, hx of cardiac, E/I
endocarditis, rheumatic fever, and COVID-19
RA, lupus, sarcoidosis
higher vagal resting tone
meds:
Sodium channel blockers (Lidocaine)
Beta blockers (Metoprolol)
Calcium channel blockers (Diltiazem)
Potassium channel blockers (Amiodarone)
Cardiac glycosides (Digoxin)
Magnesium
s/s: no s/s → until ADL interruption (dizzy or SOB)
lab/dx:
BMP, toxicology
ECG
tx:
low sodium, cholesterol, triglycerides
lifestyle modification
check for abnormal heart sounds
→ s/s → atropine, isoproterenol
Afib
rapid, chaotic, firing that does not allow atria to properly contract = inc blood clots
causes:
DM, OSA, hyperTH, smoking, sedentary, cardiac surgery
HTN, COPD, stroke
s/s:
dizzy, palpitation,
stroke → w/ med → inc bleeding
no s/s unless affect perfusion
irregular apical pulse, low BP, palpitation, high HR
weight gain and in urination
lab/dx:
hyperTH, CBC, glucose, creatinine,
oral coagulant → INR
ECG: no P waves
HR: normal or <100 (rapid ventricular response RVR)
Echo: determine size of chambers → transesophageal echocardiogram (TEE)
tx:
anticoagulant:
no catch up w/ doses
bleeding precautions → soft-bristle brush, safety razors, no contact sports
warfarin (VKA) → q2-4w PT/INR
keep normal vit K consumption
direct oral anticoagulants (DOACs) =apixaban (Eliquis), dabigatran (Pradaxa), and rivaroxaban (Xarelto)
no testing required
only reversal when bleeding emergencies
dabigatran (Pradaxa) is idarucizumab (Praxbind).
Andexanet alfa= apixaban (Eliquis) and rivaroxaban (Xarelto).
refrain from high intense activities, stimulants, herbs
Decreases the Effect (Increases Risk for Blood Clotting)
Coenzyme Q-10
Ginseng
Licorice
St. John's wort
Increases the Effect (Increases Risk for Bleeding)
Danshen
Evening primrose
Ginkgo biloba
Saw palmetto
assess:
pulse deficit (apical pulse - radial pulse)
synchronized electrical cardioversion: timed electrical shock on R wave to disrupt irregular cycle = when pt unstable and not able to maintain BP
50-200 joules
conscious sedation → maintain open airway and continuous cardiac monitoring
anticoag 4 weeks after
antidysrhythmic: BB, CCB, amiodarone, digoxin
require monitoring of QT prologue, low HR
amiodarone for most complicated
ADR: pulmonary fibrosis, or liver = PFT, and LFT
→ electrophysiology (EP) study (map out electricsal system) cardio ablasion
foods w/ vit K:
HIGH amount of vitamin K
Brussel sprouts
Greens (beets, collard, mustard, turnips)
Kale
Spinach
MODERATE amount of vitamin K
Asparagus
Broccoli
Cabbage
Carrots
Cauliflower
Celery
Green beans
Lettuce (butterhead, iceberg, romaine)
Mixed vegetables
Okra
Peas
Pickles
LOW amount of vitamin K
Avocados
Bananas
Corn
Fruit
Garbanzo beans
Green or red peppers
Potatoes
Tomatoes
Medications that later VKAs:
Increase INR
Acetaminophen
Allopurinol
Antibiotics
Cephalosporins
Doxycycline
Fluoroquinolones (ciprofloxacin, levofloxacin, moxifloxacin)
Macrolides (azithromycin, erythromycin)
Metronidazole
Penicillin (amoxicillin, amoxicillin-clavulanate)
Antifungals (fluconazole, miconazole)
Chemotherapy (capecitabine, 5-FU)
Testosterone
Decrease INR
Antibiotics (dicloxacillin, nafcillin, rifampin)
Antiseizures (carbamazepine, phenobarbital, phenytoin)
Immunosuppressants (Azathioprine
Protease inhibitor (ritonavir)
Sucralfate
Supplement (St. John’s wort)
Vitamin K
Atrial flutter
(supraventricular) beating in NR atrial rates = 240-400bpm but ventricular HR = normal
cause: after Afib
recent MI, or cardiac surgery
BB, CCB, amiodarone, digoxin
DM, hyperTH, OSA< obesity, alcohol, smoking
cardiomyopathy, pericarditis
s/s:
low BP, dizzy, palpitation, SOB, syncopal ep
lab/dx: check for BMP, LFT, TH, kidney
ECG: P waves → flutter waves
echo
tx = Afib tx
supraventricular tachycardia SVT
Paroxysmal supraventricular tachy (PSVT) = AV nodal reentrant tachy (AVNRT) = occur w/o precipitating factors and ends w/o warning
causes:
inc stress, smoking, alcohol, caffeine, stim
hx of HF, Wolff-parkinson-White syndrome, pregnancy, COPD
s/s:
unable to perform normal exercise routine
dizzy, syncopal ep
low BP, SOB
abrupt heart palpitation
lab/dx:
check for DM, hyperTH, renal disease, CBC, E/I
ECG: regular rhythm, HR 110-220, narrow QRS<0.12
PSVT = same except HR ~ 160bpm
tx:
valsalva maneuver
→ adenosine → diltiazem, esmolol, or metoprolol
defibrillator and resuscitation should be at bedside
CAD:
due to atherogenesis, and inflammation of tunica intima
chronic stable angina:
pain when exercise → nitroglycerin
→acute coronary syndrome (ACS)
STEMI: abrupt disruption of blood flow by artery blockage due to artery erosion, or dissection of CA = thormbus
NSTEMI (w/ elevated cardiac markers), unstable angina
cause: artery spasm, stable plaque, cardiac embolism, arteritiis
→ low BP, high HR, aortic stenosis, PE
complete stop of blood flow
cause: HTN, sedentary, DM, smoking
age, sex, race, family hx
poor sleep, HLD, stress
comorbidities: joint pain, BMI of 30, gout, OA, cancer
s/s: chest pain → HF/ arrhytmias
mental health = depression, anxiety, stress, PTSD
no s/s → pain can radiate form left arm, neck, jaw
unstable = ACS = !!!
diaphoresis, dizzy, n/v, SOB, weakness
female = no chest pain = extreme fatigue, abdominal pain, nausea, chest pressure
DM = right side of the chest, epigastric region, or the back of the neck, or no pain
check for peripheral edema, lung and heart auscultation
lab/dx:
cholesterol: high LDL and low HDL, high triglycerides
homocysteine (amino acid) → broken down by vit B12/6, folic acid
high = high risk of CAD = cause damage to lining of vessels
inflammation: CRP
MI= Troponin I/T detect cardiac injury within 4hrs of MI s/s
CK-MB= detect 4hrs and peak in 24hr, goes down ~ 48-72hr so can be used to detect reinfarction
myoglobin= one hr after injury but for skeletal and heart
ECG: ST elevation/ depression, T wave inversion
cardiac catheterization: (angiogram)
use contract for digital photographs
ADR: bleeding, blood clot, or vessel damage
infection, heart arrhythmias, ischemia, chest pain, MIs, sudden blockage of the coronary artery or damage to the coronary arteries, decreased kidney function due to the contrast, stroke, and death.
Stress tests:
exercise: treadmill= reach 85% of predicted HR while measuring VS and ECG, if angina → CAD dx
echo: send soundwaves to capture heart images to see if there is decrease blood flow to heart → then get target heartrate and another echo
use dobutamine for those who are unable to walk on treadmill
nuclear stress test :
radioactive for 15-45mins the camera w/ treadmill and take pics
X-rays
tx:
educate on lifestyle change (DASH), how to use nitrate, use medical alert bracelet
sleep 7-9hr
obtain blood pressure in both arms, get apical pulse, check capillary refill, JVD, use bell for S3/S4
continous monitoring
if elevated troponin = 150-300mg of ASA, heparin, no ticagrelor if thombolysis,
pain control and O2 sat
unstable/ NSTEMI → perfusion study (SPECT/ PET)
all ACS cases = BB, statins, ACE inhibitor STAT
CABG (bypass)
enter by left internal mammary artery, the saphenous vein in a lower extremity, the radial artery, or the gastroepiploic artery.
later require ICU
complications stroke, infection, failure of graft, kidney failure
, Afib development
angioplasty: w/o stent (percutaneous coronary angioplasty (PCI)
inflatable balloon and plaque pushed into wall
stent has a wire mesh
removed with pressure from puncture site
med:
ACE inhibitors: -pril
BB: metoprolol, atenolol, esmolol
CCB: nifedipine, verapamil, diltiazem
nitrates
statins
non statins:
ezetimibe, alirocumab, gemfibrozil, fenofibrate
thermolytic agents: tPA
antiplatelet: ASA
anticoagulant: heparin, enoxaparin
DASH diet:
Eating fruits, vegetables, and whole grains
Including fish, poultry, beans, and nuts in diet
Using fat-free or low-fat dairy products
Using vegetable oils
Limiting foods high in saturated fat
Limiting fatty meats
Limiting sugary foods and beverages
Limiting sodium intake
M": Morphine
O: O2
N: Nitroglyceride
A: antiplatelet
valvular dysfunction
valve regurgitation or stenosis (calcification)→ HF, sudden cardiac arrest, death
causes:
congenital heart valve disease (biscupid)
RA , endocarditis (ex strep throat)
HTN, MI, atherosclerosis of the aorta, HF
lupus, Marfan syndrome, radiation (→ Ca deposits), aging
high sodium, sweet, smoking, HLD, DM, CAD,
dilation of left ventricle, or radiation tx, defibrillators or pacemakers
aortic stenosis = HTN (also regurgitation), HLD, Afib, DM
mitral regurgitation = Afib, PVC, HTN
tricupid regurgitation = COPD, pulmonary HTN
s/s:
fluid overload: edema, SOB
syncope, fatigues
chest pain, murmur, palpitation
abdominal pain due to enlarged liver
lab/dx:
Echo= left side → sonographer moves trasducer w/ sound waves → heart pictures = measures pressure fro each valve
if stenose = more pressure on front side
can also measure size of valve and EF (50-70% normal)
TTE (transthoracic), TEE (also mitral valve disease and chordae problems)
CXR
ECG: indicte previous cardiac damage
cardiac MRI
cardiac catheter
stress test
tx:
check for illicit drug and IV sharing,
assess pulses, edema, ascultate
mamnagemetn of s/s: BB, digoxin, CCB
diuretics for fluid overload, vasodilators
surgeries:
valve repair: no replace but decrease s/s
balloon valvuloplasty: expands opening of stenosed valves
valve replacemet: from animal, donor, or mechanical (for yonger than 65y or PTH activer extra)
biological for CKF, not able to take warfarin, pregnant, for inc for bleeding
take 10-15y
ICU for 3-7 days
HF
heart not able to meets of the body ← when ventricles not filling properly,
causes:
CAD, MI, DM
uncontrolled arrhythmias, HTN, myocarditis, congenital heart disease
thyrotoxicosis, anemia, thiamine deficiency, pregnancy
anthracycline (cardiotoxic agent)
comorbodities: obesity, A-fib, CKD, DM, HTN
s/s:
SOB, fatigue, difficulty sleeping, LE edema
may need O2
L/R side: JVD and SOB, and both L/R manifestations
L: low BP w/ high HR, orthopnea, paroxysmal nocturnal dyspnea, LE edema, weight gain, inc abdominal girth, pulmonary congestion (rales/ productive cough w/ pink sputum), PMI displaced to one side
R: S3, murmur, palpitation, ascites, peripheral edema, enlarged spleen/liver
lab/dx:
Framingham Diagnostic Criteria:
major:
Acute pulmonary edema, Pulmonary rales
Cardiomegaly
Hepatojugular reflux
JVD, Central venous pressure greater than 16 cm of water
Paroxysmal nocturnal dyspnea or orthopnea
Third heart sound (S3 Gallop)
Weight loss of 4.5 kg or more in five days in response to treatment
Radiographic cardiomegaly
minor:
Ankle edema
Dyspnea on exertion, Nocturnal cough, Pleural effusion
Hepatomegaly
Tachycardia (heart rate greater than 120/min)
A decrease in vital capacity by one third the maximal value recorded
NYHA classification for HF:
I: no s/s
II: slight limits in ADL, rest has no s/s
III: moderate s/s, only comfortable at rest
IV: severe limitations, s/s at rest
(chest pain, SOB, heart palpitations, fainting)
check for renal, liver, anemia or iron deficiency,
BNP
cardiac catheterization, PCI
echo: check
systolic HF: not enough for to push out to system
diastolic HF: not enough space for blood to fill
CXR, ECG, stress test (determine cause of HF)
tx:
weight gain of more than 2-3lb/ day or 5lb/week = worsening HF, daily weight
sodium restrictions 2-3g/day and fluid restrictions 2L/day
if resp distress: high Fowler, cough and deep q2h, lung sounds reassess q4h
lifestyle modifications:
meds:
Sodium-glucose-co-transporter 2 (SGLT-2) ~~
ACE inhibitor: -pril
ARBs: -sartan
angiotensin-receptor neprilysin inhibitors (ARNIs): sacubitril/valsartan
BB
aldosterone antagonists: spironolactone, eplerenone
hydralazine and isosorbide dinitrate (biDil)
Diuretics: furosemide, chlorothiazide, amiloride
statins, anticoag, digoxin
surgery:
cardiac catheterization, percutaneous cardiac intervention if by acute MIO
enlarged ventricles → ventricular desynchrony (relax at diff times) → cardiac resynchronization therapy( CRT) w/ biventricular pacemaker
less than 35% EF = implantable cardioverter defibrillators (ICD)= under skin w/ 2 wires one in RA other in RV
discharge instructions:
check for infection,
dry for 4-5 days, no tub baths or swim, no rubing,
no lifting more than 10-15lb, no twist,pull or push for 2-3w, no lift arm of affected side higher than shoulder,
need follow up appt
cardiomyopathy
4 types:
dilated (DCM): weakened ventricles
hypertrophic (HCM): thickened hypertrophy
restrictive (RCM): stiffness of ventricles
arrhythmogenic cardiomyopathy (ACM): wall muscle is replaced w/ fibrous, fatty tissue → dysrhythmias
causes:
DCM: viral infections, autoimmune, myocarditis, sarcoidosis, malnutrition, endocrine, inflammatory, alchohol
HCM: genetic predisposition, occur in athelets
RCM: unknow but ~ hx of amyloidosis, sarcoidosis
ACM: genetic
s/s:
medications can disrupt libido, mood , urinary continence
DCM: chest discomfort, peripheral edema, increse levels of fatigue, exertional SOB
HCM: no s/s → fatigue, syncopal ep, palpitations, exhaustion, SOB, risk of sudden cardiac death (those w/o s/s)
RCM ~ DCM/HCM
ACM: ~DCM/HCM + ascites, JVD, lethal dysrhythmias,
lab/dx:
CXR
CBC, CMO (liver, thyroid, renal)
BMP, troponin I/T
ECG: irregular rhythm, wide QRS (bundle branch block), P/T wave change, lethal dysrhythmias
Echo
tx:
may have ICD for abnormal rhythmias supervision
aviod strenous exercise, lifestyle modification, fluid and sodium restriction, daily weight
meds: diuretics, vasodilators,
DCM: ACE, ARB, BB, mineralocorticoid antagonist
HCM: BB, CCB
RCM: needs high HR so caution w/ CCB and BB
surgery:
heart transplant
LV assist device (LVAD): battery operated mechanical pump
ICU 4-5 days
HCM: septal myectomy (remove peaces of septum for diastolic filling)), alcohol septal ablation w/ cardiac catheterization
ICD: 6-12y)
Pericarditis:
pericardial sac inflammated (50 mL of fluid in sac)
→ untreated = rigid and constricted
causes:
idopahic ~ GI or FLU like illness
cardiac procedures, bacterial infections, cancer (lung, breast, lymphoma), autoimmune (hypoTH)
s/s:
Dysphagia, low grade fever, recent weight loss, pericardial friction rub, hiccups
ST elevation, PR depress
Lab/dx:
WBC, CRP, ESR, temp more of 100.4F, blood cultures
troponin I/T
Echo: check for fluid accumulation
CXR/ cardiac MRI: for pericardial effusion
tx:
chest pain or discomfort that worsens when inhaling or laying supine and improves when sitting upright
avois strenous exercise
hold breath, if rub = cardiac
meds: antiinflammatory
NSAID, colchicine ( targets pericardium), glucocorsteriods
pericardial effusion
effusion compressed all chambers = (50-100) - (100-500)- (>500mL)
→ cardiac tamponade!! = >200mL
causes: cancer, infection, metabolic illness, cardiac trauma (~ pericarditis)
s/s: high temp, chest pain, dry cough, SOB when exertion or laying supine
lab/dx: renal, thyroid, CK-MB, troponin
ECG: sinus tachy, low QRS voltage, electrical alternans canges beat-to-beat amplitude (vertical) of QRS
echo
CXR
tx:
pericardiocentesis if !!! ← NPO
local anesthetic
assess for bleeding risk
low blood pressure, muffled heart sounds, rapid pulses, and shortness of breath
PVD
veins, and arteries
Veins: damaged, occluded, or altered
chronic venous disease (CVD): in wall of vein, blood pools in legs → reflux = chronic vein insufficiency (CVI) and VTE → vein distention and varicose veins ( collagen and smooth muscle have low elasticin
→ increased venous pressure → ulcer formation and DVT
DVt (Virchow triad) = injury of wall, abnormalities in clotting, vein stasis
causes:
abdnormal structure → venous reflux, valcular incompetency
genetics, progesterone
family hx, obesity, smoking, pregnancy, hx of WTE, standing for long periods, oral contraceptives, recent surgery/ hospitalization, hypercoagulability
primary CVD = progressive/ secondary CVD = previous DVT, congenital CVD
s/s:
→ PE
varicose veins, brown pigmentation w/ leg edema, pruritus, open sores, restless legs, feeling of heaviness in LE
hemorrhage, phlebitis, and DVT can develop
lab/dx:
plethysmography = blood volume in LE
Duplex ultrasound: images of vascular system, direction of blood, and severity of reflux
tx:
elevate legs higher than heart for 30 mins 3-4/day, ankle pumps
stop smoking, exercise and walk for 30 mins, no standing for long or cross legs when sitting
compression sucks
assess pulse, temp, color, wounds, edema, stasis dermatitis, lipodematosclerosis
surgery:
vein-stripping, ultrasound-guided sclerotherapy (vein assessed w/ catheter and UT), radiofrequency and laser ablation
meds:
flavonoids (anti-inflammatory) → diosmin
pentoxifylline→ hemorheologic agen
ASA
Saponins
PAD
causes:
ATHEROSCLEROSIS
injury LE, inflammation, radiation, embolisms or thrombosis, vasospasm
BMI 30, DM, Hypercholesterolemia, high homocysteine, smoking, hx of CV
s/s:
discomfort, weakness, cramping, anxiety
→ nerve damage →functional disability, infection, ulcerations
intermittent claudication
shiny appearance, pale, elevated or cyanotic, bruits in iliac and femoral
if in dependent position → red color
lab/dx:
ankle-brachial index (ABI)
> 1.4 = vessel stiff
<0.9 vessel narrowing = PAD
measures ankle SBP ratio and compares w/ brachia SBP
uses doppler and gel, use blood cuff above ankle and doppler placed in dorsalis pedis → repeated in tibial = use highest reading → repeated in other leg
then get branchial
Duplex UTsonography: gets a 2d image, locates lesions, hemodynamic
CTA, MRA, peripheral angiogram
tx:
check 6Ps = pallor, pain, polikilothermia, pulse, paralysis, parathesis
cessation of smoking, controlling hypertension, maintaining a healthy weight, and reducing cholesterol
2 goals:
lower CV
improve ability to move
exercise therapy (30-45min 3-4xday for min of 12w)
med:
cilostazol - antiplatelet
pentoxifylline
surgery: balloon angioplasty, stent, bypass graft
lead placement
RA lead—on the right shoulder or arm
LA lead—on the left shoulder or arm
RL lead—on the right leg
LL lead—on the left leg
V1 lead—at the 4th intercostal space, right sternal border
V2 lead—at the 4th intercostal space, left sternal border
V3 lead—midway between V2 and V4
V4 lead—at the 5th intercostal space, left mid-clavicular line
V5 lead—at the 5th intercostal space between V4 and V6
V6 lead—at the 5th intercostal space, just left of the spine
tx:
check foot daily