Reading 1: Medical Model of Disability
Core Concept: The Medical Model
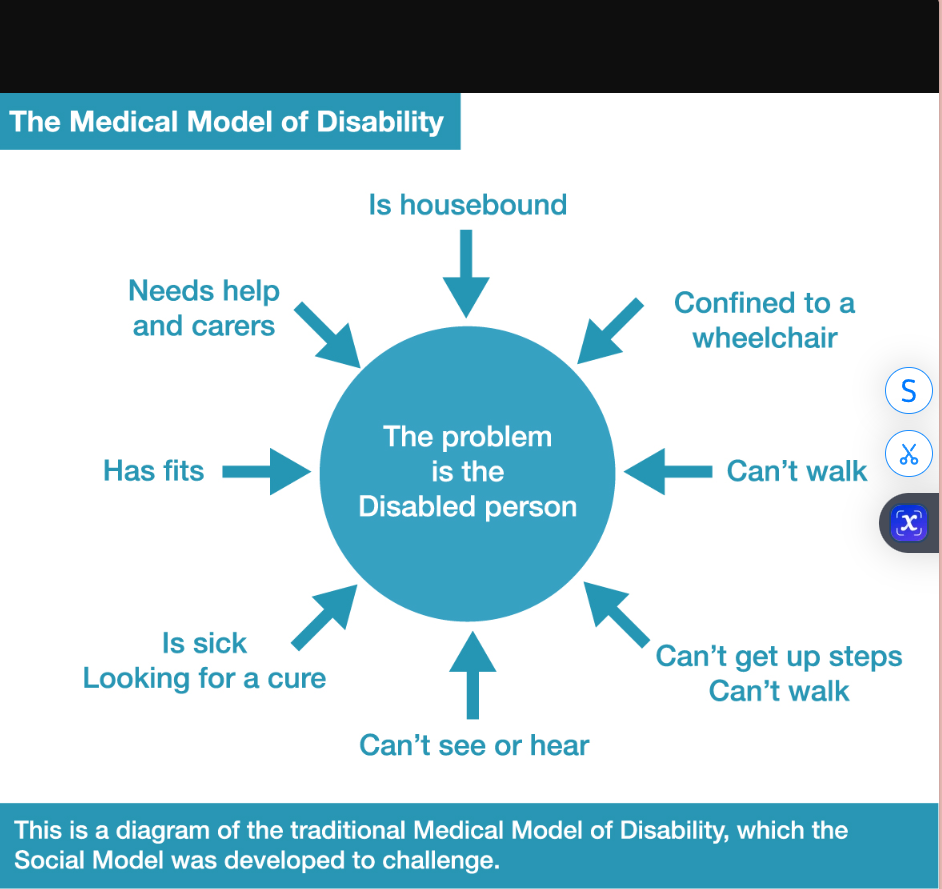
Definition: Views disability as an individual impairment or deficit located within the person.
Primary Goal: To "fix," cure, or treat the impairment to help the individual conform to societal norms of ability.
Focus: On what is "wrong" with the individual.
Key Characteristics
Professional Expertise: Doctors, clinicians, and specialists are seen as the authorities on disability.
Treatment-Oriented: Solutions are primarily medical or therapeutic interventions.
Context of Use: Predominant in healthcare, mental health, and traditional special education systems.
Critical Implications & Criticisms
Negative Outcomes:
Stigmatization: The individual is labeled as the problem.
Disempowerment: Disabled people are passive recipients of care rather than active agents.
Overlooks Environment: Ignores how societal barriers (attitudinal, physical, and systemic) create disability.
Resulting Feelings: Can foster shame, dependency, and low self-worth within the disability community.
Position Relative to Other Models
Contrasts with:
Social Model: Views disability as created by societal barriers.
Biopsychosocial Model: Integrates medical, psychological, and social factors.
Strength-Based Approaches: Focus on abilities and potential.
Hidden Disabilities & the Stigma-Disability Cycle
Hidden Disabilities: Non-visible conditions (e.g., learning disabilities, ADHD, mental health conditions, chronic pain).
Triple Burden:
Stigma of diagnosis – internalized shame, stereotyping
Environmental barriers – settings, systems, expectations not adapted to needs
Constant measurement – daily performance monitoring, deficit-focused assessment
Result: Can lead to or exacerbate mental health challenges (anxiety, depression, low self-worth).
Practitioner Training & Model Awareness
Dominant Training: Most professionals first learn medical/deficit models.
Reference Point: Definitions and diagnoses are often used as primary frameworks.
Best Practice
Use diagnostic knowledge but do not run therapy/intervention solely by the deficit model
Shift from “What’s wrong?” to “What’s needed?” and “What’s strong?”
Complexity & Co-morbidity in Hidden Disabilities
Rarely isolated: Many hidden disabilities co-occur (e.g., dyslexia + ADHD, autism + anxiety).
Overlapping challenges — create complex, layered experiences.
Overlapping strengths — are also common but often unrecognized or hidden.
Implication — A singular, deficit-focused approach fails to capture the whole person.
Core Tension: Accessibility vs. Cure
Medical Model Goal: Cure, fix, or normalize the individual.
Social/Inclusive Model Goal: Provide accessibility – remove barriers, offer accommodations, design for diversity.
Paradigm Shift Required:
From: “How do we treat this disability?”
To: “How do we make the environment, curriculum, and society accessible to this person’s needs and strengths?
Key Terms:
Medical/Deficit Model
Impairment vs. Disability
Professional Expertise
Cure/Treatment Paradigm
Stigmatization