Psychopharmacologic Agents
The prevalence of psychiatric disorders such as depression and anxiety has significantly increased in the US.
Statistics: 9.6 million adults in the US are documented as suffering from severe mental illness.
Guidelines: Most psych medications should be continued through the perioperative period.
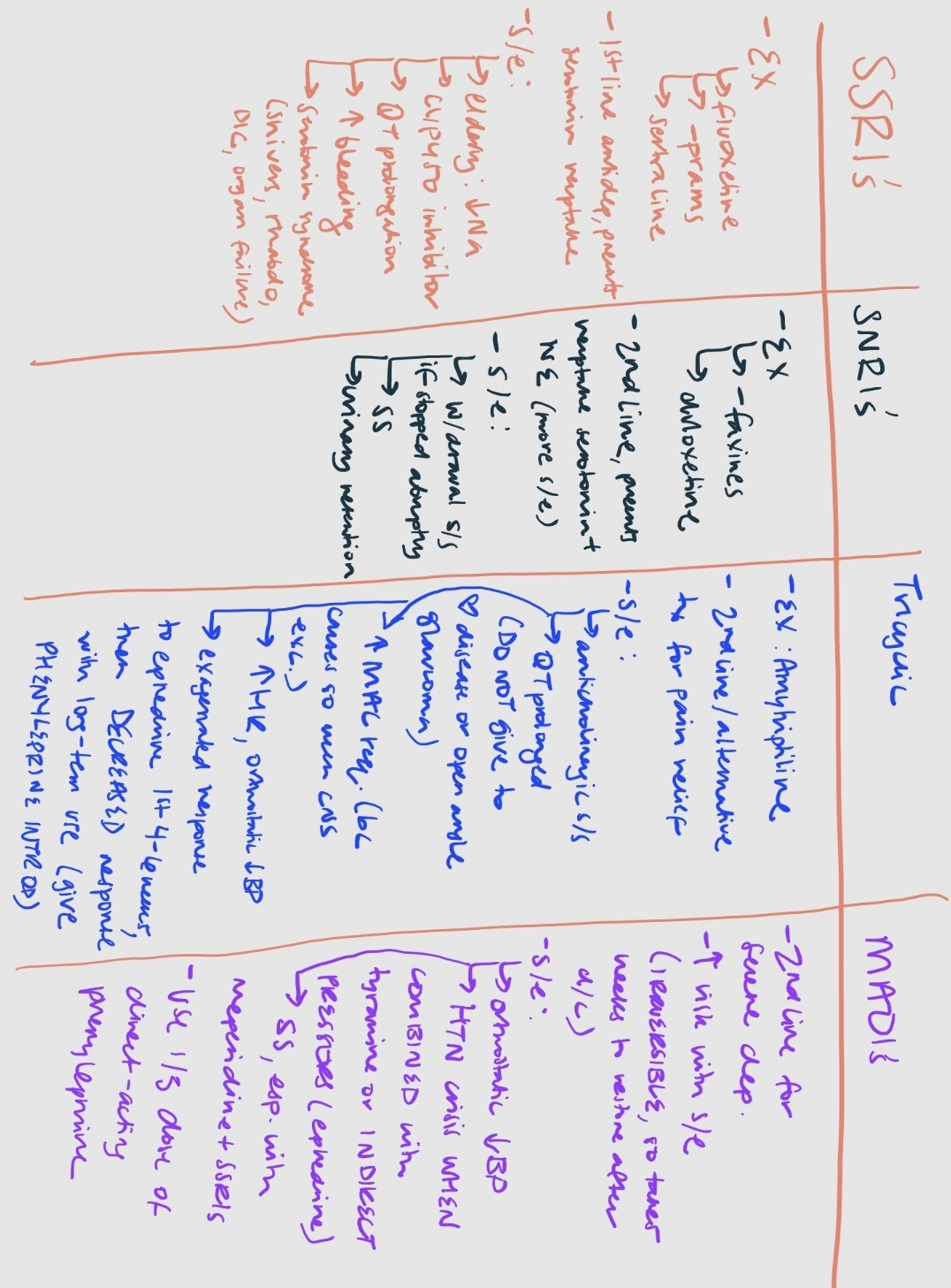
Selective Serotonin Reuptake Inhibitors (SSRIs)
EX Drugs: Fluoxetine, Paroxetine, Sertraline, Fluvoxamine, Citalopram, Escitalopram
Mechanism of Action (MOA): Bind and inhibit the serotonin transporter protein (SERT), blocking the reuptake of serotonin from the synaptic cleft back into the presynaptic neuron, which inhibits serotonergic transmission.
These are first line tx in depression and should be continued through periop period
Side Effects:
Insomnia, nausea, diarrhea, headache, dizziness, sexual dysfunction.
Elderly patients may experience hyponatremia.
Antiplatelet effects may increase bleeding risks.
CYP450 inhibitors
QT Interval Prolongation: Citalopram and Escitalopram
Serotonin Syndrome:
A condition marked by toxic levels of synaptic and extracellular serotonin causing autonomic excitability, neuromuscular excitability, and mental status changes.
Symptoms: Life-threatening hyperpyrexia, rigidity, risk of rhabdomyolysis, multi-organ failure, and disseminated intravascular coagulation.
Common Causes: Often caused by drug combinations or interactions.
Serotonin Norepinephrine Reuptake Inhibitors (SNRIs)
EX Drugs: Venlafaxine, Desvenlafaxine, Duloxetine, Levomilnacipran
Mechanism: Inhibit both norepinephrine transporter (NET) and SERT.
Usage: Commonly employed as first or second-line treatments for anxiety, depression, and chronic pain.
Side Effects:
Increased sweating, tachycardia, urinary retention, and dose-dependent hypertension. “SHIVERS”
Withdrawal symptoms with abrupt cessation.
Tricyclic Antidepressants (TCAs)
EX Drugs: Amitriptyline, Doxepin, Clomipramine, Nortriptyline, Imipramine, Desipramine
Usage: Second line or alternative treatments for depression and as analgesic adjuncts (pain relief typically observed in 7 (-14 days)
Common Side Effects: Anticholinergic effects (dry mouth, urinary retention, constipation, blurred vision, confusion).
Risks:
May cause cardiac conduction delays, potentially leading to dysrhythmias.
Prolonged QT interval necessitates ECG screening, especially in patients with heart disease.
Avoid Amitriptyline in pts with hx heart disease (arrhythmias, HF, conduction disorders) an open angle glaucoma
Causes increased HR and orthostatic hypotension?
Increases MAC requirements of volatile anesthetics due to increased catecholamines.
Exaggerated responses to ephedrine for the first 4-6 weeks of TCA administration. After initial increase in catecholamines, receptor down regulation and depleted catecholamine stores result in lesser response
Direct acting PHENYLEPHRINE is the preferred vasopressor if needed.
Monoamine Oxidase Inhibitors (MAOIs)
EX Drugs: Phenelzine, Moclobemide, Isocarboxazid, Selegiline, Tranylcypromine
Second-line treatment for severe depression, not used as often due to side effects (hypotension, insomnia) and potential lethal overdosing
Mechanism: Inhibit either MAO-A or MAO-B (same as Epi);
MAO-A ENZYMES: metabolize serotonin, NE, and Epi
MAO-B ENZYMES: metabolize phenylethylamine
**MAOIs form an irreversible complex with MAO enzyme which causes an increase in neurotransmitter release (Norepinephrine, epinephrine, serotonin, dopamine)
Risks:
By itself, causes orthostatic hypotension
Hypertensive crisis may occur WITH tyramine containing foods or indirect acting vasopressors (ephedrine)
Use directing acting vasopressors (Phenylephrine); 1/3 total dose
serotonin syndrome due to drug interactions with OTC dextromethorphan, Ecstasy, SSRIs, Meperidine, atypical antipsychotics
Anesthesia considerations:
No longer recommended to discontinue MAOIs but the anesthesia plan should be altered.
Avoid the use of Meperidine
Regional anesthesia is acceptable, but Ephedrine should not be used if patient experiences hypotension
Direct acting vasopressors should be used (Phenylephrine)
Lithium
Drug of choice for maintenance of bipolar disorder–
Often given with anticonvulsants or other antipsychotic medications
Narrow therapeutic window
Side effects: tremors, thirst, confusion, weight gain, polyuria, & edema
Avoid NSAIDs, ACE inhibitors, Diuretics (which can ↑ lithium levels)
not tylenol!!!!
Prolongs the duration of neuromuscular blocking agents, reducing MAC requirements (as causes more sedation)
**still continue periop
Antipsychotics/Neuroleptics
Medications used to treat schizophrenia and other serious mental illnesses
Dopamine receptor antagonists (first generation) EX: Haloperidol, Loxapine, Pimozide, Chlorpromazine, Thioridazine, Perphenazine, Fluphenazine
antiemetic properties (Haloperidol)
risk of prolonged QT interval, tardive dyskinesia, sexual dysfunction, neuroleptic malignant syndrome
Serotonin-Dopamine receptor antagonists (second generation- atypical antipsychotics) EX: Abilify, Zyprexa, Seroquel, Risperdal
More commonly used
Should be continued throughout the perioperative period.