EEG EXAM NORMAL VS ABNORMAL
Normal Awake EEG Pattern
In a relaxed, awake adult with eyes closed, the expected EEG features include:
Posterior dominant rhythm (alpha, ~10 Hz) over occipital regions
Symmetry between left and right hemispheres
Low-voltage fast activity over frontal regions
Alpha reactivity: posterior alpha attenuates with eye opening or increased attention
Absence of posterior alpha in an awake adult should prompt further consideration.
Symmetry as a Key Principle
EEG interpretation relies heavily on symmetry.
Always compare:
Left vs right hemispheres
Anterior vs posterior regions
Marked asymmetry between equivalent regions often suggests focal cerebral dysfunction.
Symmetry is expected in normal EEG recordings.
Slowing and Brain Dysfunction
Slowing refers to increased theta or delta activity.
Focal slowing
Suggests local cortical dysfunction near a structural lesion (e.g. tumour, stroke)Generalised slowing
Suggests diffuse brain dysfunction (e.g. metabolic disturbance, infection, sedation)
Age is critical:
Slower activity is more normal in children than in adults
Epileptiform Activity
Epileptiform abnormalities are defined by waveform shape, not simply size.
Typical features:
Sharp contours
Pointed peaks
Brief duration
Patterns of concern include:
Recurrent spikes
Spike-and-wave complexes
Rhythmic epileptiform discharges
Single isolated sharp transients are less concerning than repetitive patterns.
EEG Summary
EEG interpretation depends on:
Understanding that signals are differences between electrodes
Knowing the reference and montage
Checking scale before interpretation
Estimating frequency accurately
Assessing symmetry and slowing patterns
Recognising characteristic epileptiform shapes
ABNORMAL EEG
Abnormal EEG: Core Concepts
What is considered abnormal on EEG?
An EEG is considered abnormal when activity:
Looks irregular, bizarre, or non-rhythmic
Contains spikes, sharp waves, or spike–wave complexes
Appears in runs rather than smooth background rhythms
Is asymmetrical between the two hemispheres
Is localised to one region or unexpectedly widespread
Loss of symmetry is one of the most reliable signs of abnormality.
Normal EEG (reference pattern)
In an awake, relaxed individual:
EEG is symmetrical left vs right
Low-voltage fast activity dominates anteriorly
Posterior dominant rhythm (~10 Hz alpha) is visible over occipital regions
Alpha rhythm is blocked by eye opening
There is a front–to–back gradient in amplitude
Midline Pacemaker Theory
Rhythmic EEG activity is not generated by the cortex alone.
Deep midline structures, especially the thalamus and reticular nucleus, act as pacemakers
These structures synchronise activity across large areas of cortex via thalamocortical loops
This rhythm-generating system is separate from thalamic relay nuclei, which transmit specific sensory information
Because EEG is sensitive to synchronised, widespread activity, rhythms generated by these deep structures are easily detected on the scalp.
large-scale EEG rhythms are strongly shaped by thalamo-cortical synchronisation.
Explaining Abnormal EEG Patterns
Deep or midline dysfunction
Damage or dysfunction affecting:
Thalamus
Reticular formation
Brainstem
→ Produces generalised EEG abnormalities, often widespread slowing
Seen in:
Metabolic encephalopathy
Drug effects (e.g. sedatives)
Reduced consciousness
Coma
Focal vs Generalised EEG Abnormalities
Brain problem | Typical EEG pattern |
|---|---|
Focal cortical lesion | Focal EEG abnormality |
Diffuse pathology | Generalised EEG changes |
Thalamic / reticular involvement | Widespread rhythmic changes |
This distinction is central to EEG interpretation.
General Principles of Abnormal EEG
Focal lesions usually cause focal EEG abnormalities
Diffuse pathology (infection, metabolic disease, encephalopathy) causes generalised slowing
Lesions affecting deep structures can cause widespread EEG changes, even if small
Tumours and Lesions
Brain tumours are electrically silent
EEG abnormalities arise from irritated surrounding cortex, especially at tumour edges
Small or slow-growing lesions may produce little or no EEG change
Rapidly growing lesions are more likely to produce marked EEG abnormalities
EEG reflects how much the surrounding brain is disturbed, not the size of the lesion.
Speed of Lesion Development
Rapid lesions → strong EEG abnormalities
Slow lesions → brain adapts → fewer EEG changes
The rate of change matters more than the size of the lesion.
Consciousness and EEG
The degree of EEG abnormality correlates strongly with level of consciousness:
Mild impairment → mild EEG changes
Severe impairment / coma → severe, generalised EEG abnormalities
Diagnostic Caveat
EEG is not diagnostically specific.
Many different brain insults produce similar EEG patterns
EEG shows functional disturbance, not disease type
Structural imaging (e.g. MRI) is required to identify the cause
EEG and MRI are complementary tools, not substitutes.
EEG AND EPILIPSY
EEG is one of the most important tools for investigating epilepsy because seizures arise from abnormal electrical activity in the brain. EEG can show interictal abnormalities, such as spikes and sharp waves, which reflect areas of hyper-excitable cortex that are prone to generating seizures, even when no seizure is occurring. EEG can also record ictal activity during a seizure, helping to confirm that events are epileptic rather than non-epileptic and providing information about seizure onset and spread.
EEG is useful for suggesting seizure localisation, particularly in focal epilepsy, as recurrent abnormalities over the same region indicate a likely seizure focus. EEG also helps classify seizure types, for example distinguishing focal seizures from generalised seizures based on whether abnormalities are localised or widespread across the scalp.
EEG provides information about functional cortical excitability rather than brain structure. It shows where abnormal electrical activity is occurring but does not identify the underlying cause. For this reason, EEG is used to detect epileptic activity and guide localisation, while structural imaging such as MRI is required to identify the cause. EEG and MRI are therefore complementary tools in epilepsy assessment.
What does “hyper-excitable cortex” mean?
It means:
A part of the brain is too easy to activate and fires when it shouldn’t.
Normally, brain cells are picky.
They fire only when they get the right signal.
In a hyper-excitable cortex:
Neurones fire too easily
Too many cells fire together
The brain loses its normal balance between excitation and inhibition
Why is this a problem?
Because the brain depends on balance.
Excitation = “go”
Inhibition = “stop”
Hyper-excitability happens when:
Excitation is too strong
Inhibition is too weak
Or both
When that balance tips, you get:
Spikes on EEG
Seizures
Abnormal brain rhythms
What does it look like on EEG?
Hyper-excitable cortex produces:
Spikes
Sharp waves
Spike-and-wave complexes
Important:
A spike ≠ a seizure
It means the cortex is capable of producing seizures
Think of it like dry grass:
Dry grass doesn’t mean a fire is burning
But it means a fire could start easily
What causes cortex to become hyper-excitable?
Common causes:
Epilepsy
Cortical malformations
Tumours (irritating surrounding cortex)
Scarring after injury or stroke
Infection or inflammation
The lesion itself is often silent — it’s the irritated surrounding cortex that becomes hyper-excitable.
Why does this matter clinically?
Because:
Hyper-excitable cortex explains why seizures recur
It helps classify epilepsy
It guides treatment (medication vs surgery)
In EEG interpretation:
Spikes = hyper-excitability
Fast evolving rhythms = seizure
Slow waves = dysfunction or irritation
One-line exam definition (very safe)
Hyper-excitable cortex refers to brain tissue that fires excessively and synchronously due to reduced inhibitory control, predisposing to epileptiform activity.
Focal seizure — what it means
What’s happening in the brain
A focal seizure:
Starts in one specific spot
Comes from one side of the brain
Begins in a particular network (e.g. motor, sensory, language)
That spot is hyper-excitable and misfires.
What it looks like clinically
Depends on where it starts:
Motor area → twitching of one hand, face, or leg
Sensory area → tingling, strange smells, visual flashes
Language area → speech arrest
Memory/emotion area → déjà vu, fear
The person may:
Be aware (focal aware seizure)
Or confused/unresponsive (focal impaired awareness)
What it looks like on EEG
Abnormal activity starts in one region
Often asymmetric
May spread over time
If it spreads to the whole brain → secondary generalisation
What focal seizures usually mean
They suggest:
A local brain problem
Examples: tumour, scar, dysplasia, prior injury
That’s why focal seizures often trigger:
MRI
Surgical evaluation
Sometimes SEEG or ECoG
Widespread (generalised) seizure — what it means
What’s happening in the brain
A generalised seizure:
Involves both hemispheres from the start
No single starting point
Comes from brain-wide networks (often thalamo-cortical)
It’s a system-level problem, not a local one.
What it looks like clinically
Typical features:
Sudden loss of awareness
Bilateral movements
No warning
Very fast recovery (especially in absence seizures)
Examples:
Absence seizures
Generalised tonic–clonic seizures
Myoclonic seizures
What it looks like on EEG
Symmetrical activity on both sides
No focal onset
Classic example: 3 Hz spike–wave in absence epilepsy
What generalised seizures usually mean
They suggest:
Genetic or developmental epilepsy
Network-level dysfunction
Not a single removable lesion
Surgery is usually not helpful.
Why this distinction matters (clinically & for exams)
Because it affects:
Diagnosis
Treatment choice
Prognosis
Whether surgery is considered
Raised pressure / hydrocephalus (deep system compression)
When pressure rises, deep midline systems get squished and the whole cortex gets “slowed down”:
hydrocephalus
diffuse cerebral oedema
big bleeds / swelling causing global pressure effects
This matches what your lecturer said: deep systems get disrupted → generalised slowing.
How to read abnormal EEG: what these cases teach you
The core idea repeatedly emphasised in the lecture is that EEG shows how the brain is functioning, not what a lesion is called. Interpretation relies on recognising patterns and inferring the likely type and location of pathology from a small number of key features: whether activity is symmetrical or asymmetrical, the frequency of the signal (cycles per second), whether changes are focal or generalised, and whether the activity is rhythmic, irregular, or spiky.
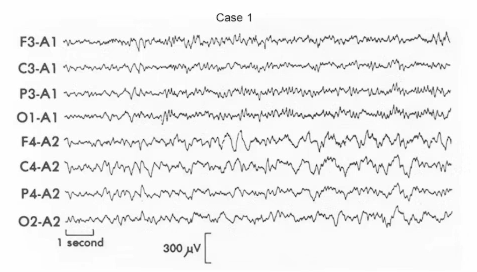
Case 1: Slow wave focus due to glioma (TUMOR)
This EEG shows high-amplitude delta activity (around 1–3 Hz) confined to a single frontal region. The abnormality is focal, clearly asymmetrical, and occurs while the patient is awake, which makes it pathological. Focal slowing in an awake adult strongly suggests a local structural disturbance of cortex. Tumours themselves are electrically silent; the EEG abnormality arises from irritated cortex at the edges of the lesion. A key rule is that focal delta in an awake adult should be assumed to reflect a structural lesion until proven otherwise.
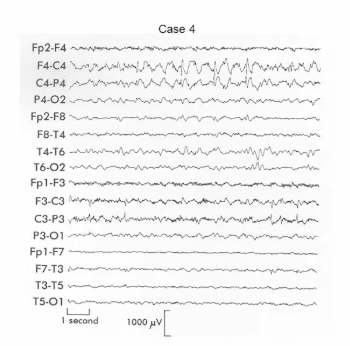
Case 2: Generalised delta due to hydrocephalus
Here the EEG shows delta activity that is symmetrical and maximal frontally on both sides, affecting large areas rather than a single region. This pattern represents generalised slowing and points to deep or diffuse pathology rather than a focal cortical lesion. Hydrocephalus fits this pattern because raised intracranial pressure compresses deep midline structures such as the thalamus and reticular system, disrupting the brain’s pacemaker mechanisms and producing bilateral slowing. Symmetrical frontal delta therefore suggests deep midline involvement rather than a tumour.
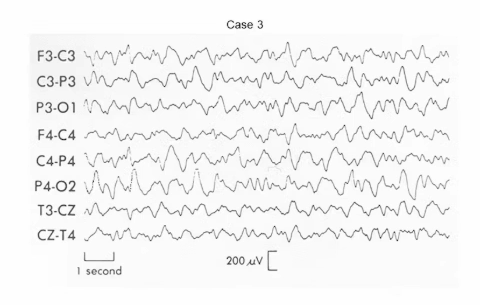
Case 3: Irregular slow waves due to encephalitis
This EEG shows slow activity that is irregular, disorganised, and lacks a clear rhythm. The abnormality is diffuse, involving both anterior and posterior regions, with no focal generator. This pattern reflects widespread cortical dysfunction and loss of synchrony. Encephalitis causes inflammation across cortex, subcortex, and white matter, producing chaotic brain activity rather than organised rhythms. Diffuse, irregular slowing is therefore typical of encephalopathy or encephalitis.
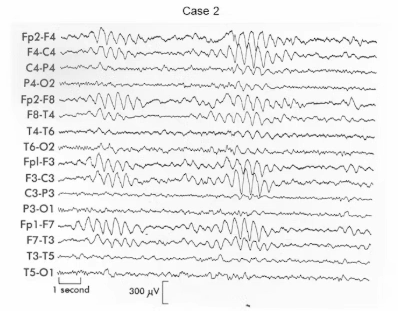
Case 4: Bilateral interictal spikes
In this case, sharp, fast transients are seen arising independently from both hemispheres. These are interictal spikes, meaning they occur between seizures rather than during one. Spikes indicate hyper-excitable, epileptogenic cortex but do not mean a seizure is happening at that moment. The presence of two independent spike foci has important clinical implications, as epilepsy with multiple foci is often harder to treat and may produce different seizure types. A key principle is that spikes reflect epileptic tendency, not seizures themselves.
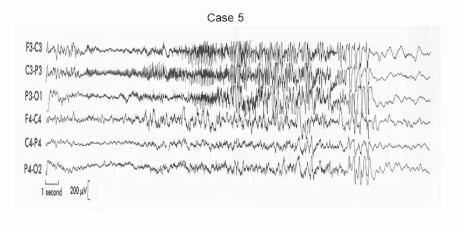
Case 5: Focal seizure beginning on the left
This EEG shows sudden high-frequency activity starting in a single region (left central), evolving over time, spreading, and then slowing, followed by post-ictal slowing. This is an ictal EEG pattern, meaning a seizure is occurring during the recording. The focal onset indicates a focal seizure, with possible secondary generalisation. A left central onset is consistent with motor features involving the face or limbs, and post-ictal slowing reflects the recovery phase. Focal fast activity that evolves in time is characteristic of a focal seizure.
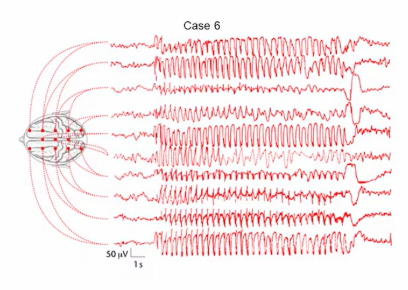
Case 6: Generalised absence seizure
This EEG demonstrates abrupt onset of symmetrical, generalised 3 Hz spike–wave activity, followed by a sudden return to normal. There is no focal onset, no evolution, and no post-ictal confusion. This pattern is classic for absence epilepsy, which presents clinically as brief lapses of awareness. A generalised 3 Hz spike–wave pattern is a hallmark of absence seizures.
Big-picture rules the lecturer wanted you to learn
Symmetry is critical: symmetrical abnormalities usually indicate deep or generalised pathology, while asymmetry points to focal cortical disease. Frequency matters: counting cycles per second helps identify abnormal rhythms, with delta in awake adults indicating pathology and 3 Hz spike–wave indicating absence epilepsy. The distinction between focal and generalised patterns guides interpretation, with focal slowing suggesting tumours or strokes, generalised slowing suggesting metabolic or infectious causes, irregular diffuse slowing suggesting encephalitis, and spikes indicating epileptogenic cortex. Above all, EEG shows brain function, not diagnosis: the same EEG pattern can have many causes, so EEG must always be interpreted alongside clinical findings and imaging.
1. How can the brain be affected even when there is no seizure?
A seizure is the loud, obvious problem.
But an excited cortex causes quiet, constant disruption in the background.
Think of brain activity like traffic on roads.
Normal brain → cars move smoothly, lights work properly
Excited cortex → traffic lights flicker randomly
Even if there’s no huge crash (seizure), traffic still doesn’t flow well.
2. Why normal thinking gets interrupted
An excited cortex:
Fires when it shouldn’t
Interrupts other signals
Competes with normal processing
So when the brain tries to:
Pay attention
Store information
Retrieve words
The abnormal activity gets in the way.
This means:
Thoughts don’t fully form
Signals are delayed or distorted
Processing becomes inefficient
Not broken — noisy.
3. Effects on attention, memory, and speech
Attention
Attention needs stable networks.
If one area keeps misfiring:
The brain keeps “checking” it
Focus drifts
Mental effort increases
This can look like:
Inattention
Slowness
Fatigue
“Zoning out” (even without seizures)
Memory
Memory depends on timing and coordination.
Excited cortex:
Disrupts encoding (laying memories down)
Interrupts consolidation (stabilising memories)
Interferes with retrieval
So children may:
Learn information
But not retain it well
Or recall it inconsistently
This is common in epilepsy even without frequent seizures.
Speech and language
Language relies on very precise timing.
If abnormal firing happens near language networks:
Word retrieval becomes harder
Fluency drops
Comprehension may slow
In children:
Language development can stall
Skills may plateau rather than regress
This is why “benign” epilepsies are not always benign.
4. Why this is especially serious in children
Children’s brains are still building networks.
An excited cortex:
Disrupts normal wiring
Interrupts learning windows
Forces the brain to “work around” noise
So instead of developing efficiently:
Networks develop more slowly
Or reorganise in less optimal ways
This can lead to:
Long-term learning difficulties
Executive function problems
Language vulnerabilities
Even if seizures later stop.
5. Why excited activity spreads
Now to the spreading part — this is key.
Neurons are connected.
They talk to each other constantly.
When one area becomes over-excited:
Nearby neurons are repeatedly stimulated
Inhibitory control gets overwhelmed
Excitation spreads outward
Think of:
One person clapping → others join in
One spark → grass catches fire
6. How excited cortex “pulls in” normal tissue
Normal brain tissue is not diseased, but it is connected.
Repeated abnormal firing:
Lowers the firing threshold nearby
Makes normal neurons easier to recruit
Turns helpers into participants
Over time:
The abnormal network grows
More cortex becomes involved
Seizures spread more easily
7. How focal seizures become generalised
A focal seizure:
Starts in one area
If excitement spreads:
It reaches both hemispheres
Large networks synchronise
The seizure becomes generalised
This explains why:
Some patients start with focal symptoms
Then lose awareness
Then have whole-body involvement
It’s not sudden — it’s network recruitment.