Anatomy
==Block 8 - Lecture 15 & 16 (Thoracic viscera 1 & 2) - Khanna==
Thoracic viscera 1
- List three major compartments of the thoracic cavity
- Right and left pleural cavities, mediastinum (cardiac window)
- Describe the topography of the lungs
- Superior: apices extend 2.5 cm above the clavicle to vertebrae prominens
- Inferior: depends upon the line of the axis
- Mid-clavicular: Rib 6
- Mid-axillary: Rib 8
- Paravertebral: Rib 10
- Right lung has three lobes, left lung has two lobes
- Describe the boundaries and divisions of the mediastinum
- Boundaries
- Anterior: sternum
- Posterior: T1-T-12
- Superior: jugular notch → T1
- Inferior: diaphragm → T12
- Divisions: separated by line connecting jugular notch → T4/T5
- Superior
- Inferior: anterior, middle, posterior subdivisions
- List the major viscera located in each of the divisions of the mediastinum
- Superior mediastinum: trachea, esophagus, & thymus (anterior)
- Middle mediastinum: pericardium, heart, initial segments of great vessels
- Posterior mediastinum: esophagus continued & primary bronchi
- Describe the surface topography for the auscultation of cardiac valves
- Right 2nd intercostal space - aortic valve
- Left 2nd intercostal space - pulmonary valve
- Left 4th intercostal space - right AV valve
- Left 5th intercostal space - left AV valve
- Describe the general function of the thymus gland and its mediastinal location
- Superior/anterior mediastinum = educates T lymphocytes to recognize self antigens & then involutes (peak mass of 35 g @ puberty)
- Describe the movements of the heart during inspiration and expiration
- Fibrous pericardium is attached to the diaphragm, heart moves up and down with each breath
Thoracic viscera 2
- Compare & contrast the anatomy of the four cardiac chambers
- RA: pectinate muscle (derived from primitive atrium), sinus venarum (smooth; derived from sinus venosus), fossa ovalis, openings for coronary sinus/SVC/IVC, crista terminalis
- RV: trabeculae carneae (muscular ridges), papillary muscles, chordae tendinae
- LA: mostly smooth, 4 x pulmonary veins, valve of foramen ovale, some pectinate muscle
- LV: trabeculae carneae, papillary muscles, chordae tendinae
- List the great vessels and the cardiac chambers that receive or issue from them
- SVC & IVC → RA
- 4 pulmonary veins → LA
- 2 pulmonary arteries (send blood from RV → lungs via pulmonary trunk)
- LV → aorta
- Describe the sulci, surfaces, base and apex
- 3 sulci: one separating A/V & 2 separating the ventricles
- Atrioventricular/coronary sulcus: separates atria and ventricles → RCA
- Anterior IV → LCA
- Posterior IV → circumflex & RCA
- Surfaces: anterior/sternocostal (RA, RV, part of LV & L auricle); right pulmonary (RA); left pulmonary (LV & part of LA); diaphragmatic (RV & LV)
- Base: receives pulmonary veins, SVC & IVC
- Apex: formed by LV, 7-9 cm left of midline, 5th intercostal space
- 3 sulci: one separating A/V & 2 separating the ventricles
- Describe the cardiac valves with regard to location and numbers of cusps
- Right AV valve = tricuspid valve; 3 cusps (anterior, posterior, septal)
- Left AV valve = bicuspid/mitral valve; 2 cusps (anterior, posterior)
- Pulmonic valve (more anterior): 3 cusps (anterior, right, left)
- Aortic valve: 3 cusps (left, right, posterior); posterior is non coronary w/ right and left giving off branches of coronary arteries
%%Block 9. Thoracic viscera 3 & 4 - Khanna%%
Thoracic viscera 3
- Describe the coronary circulation with regard to dominance and arterial distribution and venous drainage
- Right cusp of aortic artery → RCA
- Left cups of aortic artery → LCA
- Dominance patterns: depends which artery is supplying the posterior IV sulcus
- Right dominant pattern
- 70-80% of people; RCA → posterior IV sulcus (as posterior descending artery)
- Left dominant pattern
- 8-10% of people: Left circumflex → posterior IV sulcus
- Balanced pattern
- 1% of patients: 2 posterior IV arteries (RCA & LCx)
- Venous drainage:
- Great cardiac vein (anterior IV) → coronary sinus
- Middle cardiac vein (posterior IV) → coronary sinus
- Anterior cardiac veins → drain directly into right atrium
- drains primarily right ventricle
- Venae cordis minimae → run deep w/ muscle tissue
- Describe the cardiac conduction system and the clinical relevance of Koch’s triangle
- Koch’s triangle borders
- Todaro’s tendon, ostium of coronary sinus, base of septal cusp
- Location of the AV node
- SA → AV → Bundle of His → RBB and LBB → Purkinje
- Koch’s triangle borders
- Describe the pleural membranes and associated recesses
- Parietal pleura
- Regions of parietal pleura
- Costovertebral or costal pleura: along the ribcage & vertebral column
- Diaphragmatic pleura
- Cervical pleura: covers apical lung
- Mediastinal pleura
- Recesses: points of reflection -- potential spaces
- Costodiaphragmatic recess = potential space which can accumulate fluid, where costal and diaphragmatic pleura meet
- Costomediastinal recess = parietal pleura meets mediastinum
- Vertebromediastinal recess = lungs to vertebral
- Visceral pleura - up against the organ
- Potential space between parietal and visceral pleura = pleural cavity
- Parietal pleura
- Describe the trachea, its wall, and bronchial branching pattern
- Starts at C6
- Bifurcates T4, T5
- Right main bronchus: more vertical, wider
- 10-11 cm in length
- 16-20 cartilaginous incomplete rings
- Layers (internal to external)
- Mucosa - epithelium
- Tunica mucosa or submucosa - glands
- Cartilaginous/fibromuscular - trachealis muscle
- Adventitia - connective tissue coat
- Bronchi → bronchioles
- 2 primary (right and left)
- Right has 3 lobes → 3 secondary/lobar bronchi
- 10 tertiary/segmental
- Left has 2 lobes → 2 secondary/lobar bronchi
- 8 tertiary/segmental
Thoracic 4
- Compare and contrast the features of the right and left lungs
- Describe the applied anatomy in performing a thoracentesis
- Describe the esophageal segments, constrictions, and layers forming its wall
- Describe the locations of esophageal diverticula and the relevance of Killian’s triangle
- Describe the arteries of the thorax, the parent vessels that issue them, and their distribution
^^Block 10. Thoracic viscera 5 & 6 - Khanna^^
Thoracic 5
- List he parts of the aorta found in the thorax
- Describe the normal and variant branching pattern of the aortic arch
- Describe the veins of the thorax, the vessels they empty into, and their drainage
Thoracic 6
- Describe the distributions of the phrenic nerve and the sympathetic and parasympathetic divisions of the autonomic nervous system
- Compare and contrast the general functions of the ANS
- Describe the clinically applied anatomy of vocal cord paralysis and achalasia
- Describe the clinically applied anatomy of asthma, Pancoast tumor, and cardiac referred pain
@@Block 11. Abdomen 1 & 2 - Lutfi@@
Abdominal wall 1
- Locate the surface landmarks, regions, reference planes and positions of organs (appendix and liver) for the abdomen
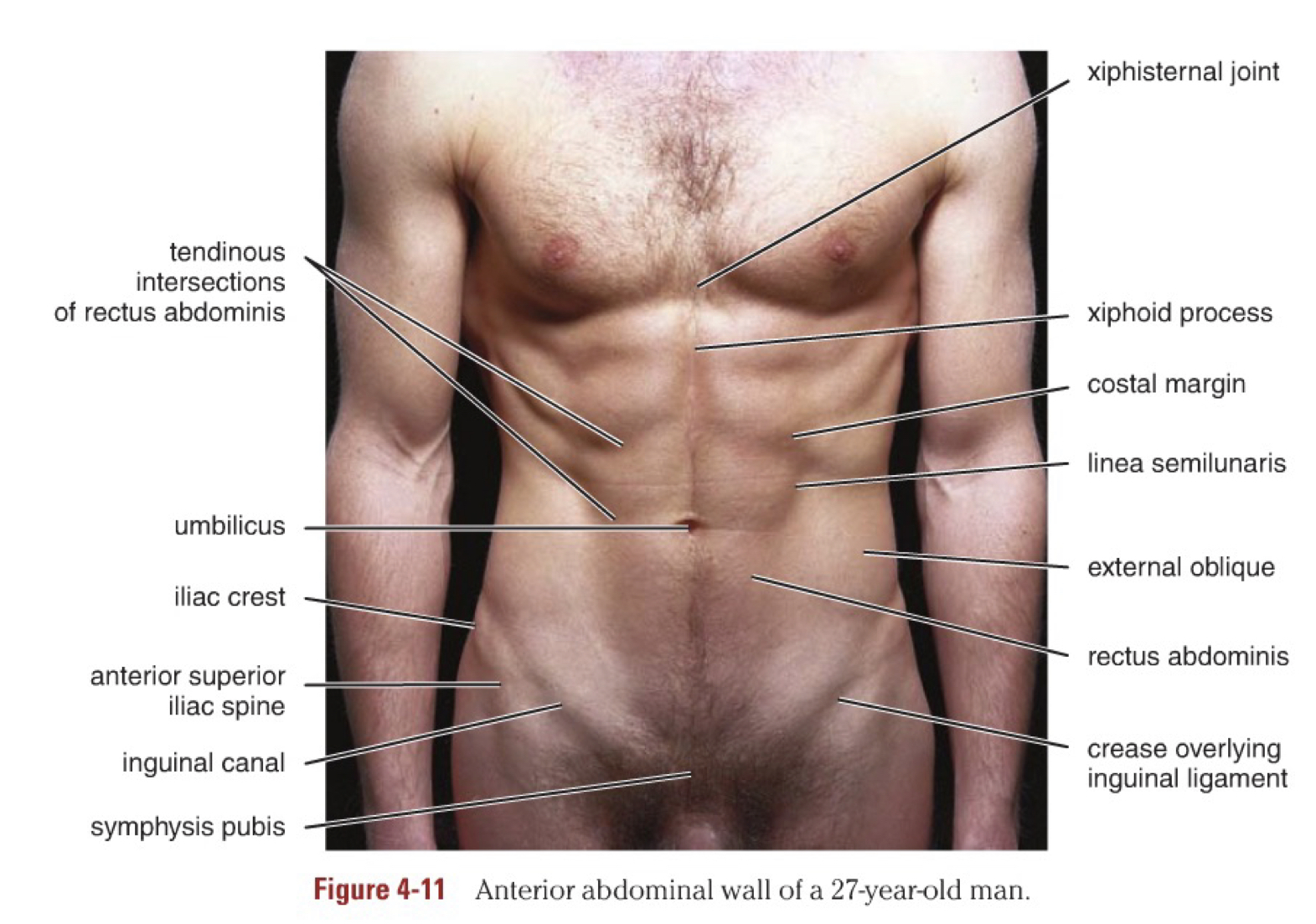 Surface anatomy:
Surface anatomy:
- Umbilicus: L3 - L4 intervertebral disc
- Linea alba: xiphoid process → pubis (separates into right and left abdomen)
- Linea semilunaris: curved line (convex laterally) approx. 5-8 cm from median plane; 9th costal cartilage → pubis; represents lateral border of rectus abdominis muscle
- Tendinous intersections: transverse lines over the rectus abdominis muscle
- Inguinal groove: division between the anterior abdominal wall and anterior thigh region
- Pubic symphysis: firm resistance felt at the inferior end of the linea alba at the anterior aspect of the median plane
- Pubic crest and tubercle: bony landmark located 2.5 cm laterally of pubic symphysis (inguinal ligament attaches here)
- Iliac crest: extends posteriorly from ASIS, the iliac tubercle can be palpated 6 cm posterior to the ASIS
- Epigastric fossa: slight depression in epigastrium just inferior to xiphoid, best seen supine
- SUPERIOR ABDOMEN
- Xiphoid process
- Costal cartilages of 7-10th ribs
- INFERIOR ABDOMEN
- Inguinal ligament
- Pubic crest and pubic symphysis
- PLANES AND REGIONS
- Horizontal planes
- Transpyloric plane = thru L1
- Subcostal plane = joins the inferior margins of the 10th costal cartilage passing thru L2-L3
- Transtubercular plane (TTP) or inter-tubercular plane = thru iliac tubercles, usually passes thru body at L5
- Transumbilical plane (TUP) = thru umbilicus; indicates the level of the intervertebral disc between L3 - L4
- Vertical planes
- Mid-clavicular lines: from mid clavicle → mid-inguinal point in the sagittal plane
- Median plane
- Position of appendix: 1/3 the distance from the ASIS → McBurney’s point
- Right inguinal region
- Position of the liver: right hypochondriac region
- Typically can’t feel it in a healthy person because it is protected by the ribs
- Define the sensory distribution of the abdomen
- List the layers of the abdominal wall from superficial to deep
- Locate the origin and insertion of the abdominal wall muscles (external oblique, rectus abdominus, internal oblique, transversus abdominus) and define their innervation and describe their actions
Abdominal wall 2
- List the components of the rectus sheath
- Distinguish the differences between the rectus sheath above and below the umbilicus
- Locate the arcuate line in the posterior view of the abdominal wall and define its significance
- Label the blood supply (epigastric vessels) of the abdominal wall and its branches
- Identify the spinal nerve branches that innervate the abdomen
- Describe the movements of the abdomen (lateral, flexion, extension, and rotation)
- Describe the boundaries of the surface anatomy of the inguinal canal
- Identify the origin, insertion, nerve and blood supply, and action of the abdominal wall muscles
- Identify the layer of the abdominal wall. Be able to list these layers in order from superficial to deep
B12. Inguinal region + inguinal hernias & Abdominal organs - Lutfi
Inguinal region and hernias
- Define the boundaries of the inguinal canal (anterior wall, posterior wall, roof and floor)
- Surface anatomy of inguinal region: ASIS → pubic tubercle
- Inguinal canal = 4-5 cm, oblique passage, runs inferomedially just superior and parallel to medial half of the inguinal ligament
- Boundaries of inguinal canal
- Anterior: aponeurosis of EOM and lateral 1/3 IOM
- Posterior: fascia transversalis, reinforced by conjoint tendon
- Roof: arching fibers of IOM and transversus abdominis (intercrural fibers)
- Floor: lacunar ligament
- Differentiate the contents of the inguinal canal male vs. female
- Male: spermatic cord + its contents
- Female: round ligament of uterus
- Both sexes: Ilioinguinal nerve (L1) ** content of inguinal canal, but not of spermatic cord!
- Describe the layers of the spermatic cord from superficial to deep
- Spermatic cord passed thru IOM, TA and IOM pass over it, and TA and IOM converge behind the superior inguinal ring → conjoint tendon
- Coverings of spermatic cord (sup to deep)
- Internal spermatic fascia from (TF) transversalis fascia
- Cremasteric fascia and muscle from IOMA and muscle fibers
- External spermatic fascia from EOMA
- Define an inguinal hernia and explain its possible causes & sites of weakness
- Inguinal canal has an opening at either end
- Deep inguinal ring: slit in TF
- Superficial inguinal ring: triangular opening in EOMA
- Hernia = abdominal protrusion of tissue thru an opening from the cavity in which it belongs
- Inguinal hernia: males > females
- Indirect (congenital) 75% of cases
- Direct (acquired)
- Inguinal canal has an opening at either end
- Differentiate between an indirect and direct hernia
- Indirect inguinal hernia: LATERAL to inferior epigastric artery → deep inguinal ring → canal → superficial inguinal ring
- hernial sac w/i spermatic cord
- can be palpated lateral to pubic tubercle
- Direct inguinal hernia: protrude ANTERIORLY through posterior wall of inguinal canal and leave abdominal canal MEDIAL to the inferior epigastric artery
- pass thru Hesselbach’s triangle (aka inguinal triangle)
- located posteriorly to superficial inguinal ring
- hernial sac parallels spermatic cod
- Indirect inguinal hernia: LATERAL to inferior epigastric artery → deep inguinal ring → canal → superficial inguinal ring
- Identify the efferent and afferent arms of the cremasteric reflex
- Afferent: ilioinguinal nerve L1 → supplies anterosuperior skin of the thigh
- Efferent: genital branch of the genitofemoral nerve L1/L2 thru superficial inguinal ring
- genital branch supplies the cremaster muscle
- Absent reflex → corticospinal tract injury
- List the contents of the spermatic cord
- Begins at deep inguinal ring and ends in the testis
- Contents (3 arteries, 2 nerves, 1 venous plexus, VD, lymph, remnant)
- Vas deferens
- Testicular artery (abdominal aorta)
- Testicular veins
- Lymphatic vessels → lumbar lymph nodes
- Sympathetic nerves (run w/ testicular artery)
- Remnant of processus vaginalis
- Cremasteric artery → cremasteric muscle
- Genital branch of genitofemoral nerve (L1-L2)
- Arteries to vas deferens (from superior or inferior vesical artery)
- Identify the boundaries of Hesselbach’s triangle
- Inferior: inguinal ligament
- Medial: rectus abdominis muscle
- Lateral: inferior epigastric artery
- Describe the venous drainage of the testicles
- Testicular veins begin in testes as extensive venous plexus (Pampiniform)
- Pampiniform plexus
- Right testicular vein leaves plexus as single vein → IVC at L1 (directly)
- Left testicular vein leaves plexus as single vein → left renal vein at L1
- Define varicocele and its pathogenesis
- abnormality in the testicular venous drainage system, valve problem
- dilated/tortuous pampiniform plexus or cremasteric plexus → infertility
- Testicular veins begin in testes as extensive venous plexus (Pampiniform)
Abdominal organs
- Describe the embryology of the GI tract
- split into foregut, midgut, and hind gut
- Define foregut, midgut, and hind gut
- Foregut: cranial portion which ends at second part of duodenum where the common bile duct enters
- esophagus, stomach, duodenum, liver, pancreas, biliary passages, gallbladder
- PSD: vagus
- SD: pre greater splanchnic → post celiac ganglion
- Blood supply: celiac trunk
- Referred pain → epigastrium
- Midgut: second part of the duodenum and ends at left colic flexure
- 2/3/4 duodenum, jejunum, ilium, cecum, appendix, ascending colon, proximal 2/3 transverse colon
- PSD: vagus
- SD: pre lesser splanchnic → post superior mesenteric ganglion
- Blood supply: SMA
- Referred pain → umbilical
- Hind gut: starts at left colic flexure → ends at upper anal canal
- distal 1/3 transverse colon, descending colon, sigmoid, rectum, upper anal canal (above pectinate line)
- PSD: pelvic splanchnic
- SD: pre lumbar splanchnic → post inferior mesenteric ganglion
- Blood supply: IMA
- Referred pain → hypogastrium
- Foregut: cranial portion which ends at second part of duodenum where the common bile duct enters
- Define the blood supply & nerve supply: esophagus, stomach, duodenum, small intestine
- Esophagus: short abdominal segment which measures 1-2 cm, enters at cardiac region of stomach posterior to level of 7th costal cartilage
- Arteries: left gastric and left inferior phrenic artery
- Venous: azygos and left gastric vein (portal system)
- Nerves: vagus, sympathetic trunks, greater splanchnic, plexuses around left gastric and inferior phrenic arteries (periarterial plexuses)
- Stomach
- Arteries: celiac trunk, common hepatic artery → right gastric artery and gastroduodenal artery, splenic artery → left gastroomental and short gastric artery
- Veins: right and left gastric veins, right and left gastroomental veins, short gastric veins
- Nerves: PSD vagus & a/p vagal branches; SD celiac plexus and T6-T9 efferent, greater splanchnic (T5-T9)
- Duodenum
- Arteries: celiac trunk via common hepatic artery through superior pancreaticoduodenal artery (gastroduodenal artery) and SMA via the interior pancreaticoduodenal artery
- Veins: portal system of veins and SMV
- Nerves: Foregut section → vagus (PSD) and greater splanchnic (SD); midgut section → vagus (PSD) and lesser splanchnic (SD)
- Small intestine: proximal 2/5 = jejunum and distal 3/5 = ileum
- Arteries: SMA (abdominal aorta L1 via jejunal and ileal branches
- Veins: portal vein (SMV joins with splenic vein)
- Nerves: Vagus (PD) and lesser splanchnic (SD)
- Esophagus: short abdominal segment which measures 1-2 cm, enters at cardiac region of stomach posterior to level of 7th costal cartilage
- List branches of the celiac trunk, superior and inferior mesenteric arteries
Celiac trunk
- Left gastric artery
- 3 branches: ventral → anterior surface of stomach, dorsal → lesser curvature, cardioesophageal → cardia and esophagus
- Common hepatic artery
- Gastroduodenal artery
- Retroduodenal artery
- Right gastroepiploic artery
- Superior pancreaticoduodenal artery
- Right gastric artery → lesser omentum and pylorus
- Proper hepatic artery
- Right hepatic artery → cystic artery
- Left hepatic artery → capsule of liver
- Middle hepatic artery → quadrate lobe of liver
- Gastroduodenal artery
- Splenic artery
- Pancreatic artery, dorsal pancreatic artery, great pancreatic artery, caudal pancreatic artery
- Left gastroepiploic artery → greater curvature
- Short gastric arteries → fundus of stomach
- Splenic artery → spleen
Superior mesenteric artery (RIIM)
- Right colic
- Ileocolic
- Ileal and jejunal branches
- Middle colic
Inferior mesenteric artery (LESS)
Left colic artery
Sigmoid artery
Superior rectal artery
- List the two veins that join to form the hepatic portal vein
- SMV + splenic vein
- Describe the parts of the stomach and its relationships
- Body: pyloric antrum and pyloric canal which is continuous with pylorus
1. 2.
7. Describe the parts of the duodenum and its relationships
- \
- Superior part
- anterior to first part = liver and gallbladder
- posterior to first part = bile duct and portal vein
2. Descending part
- lies anterior to renal vessels
3. Horizontal
- Lies anterior to the IVC, aorta, right ureter, right gonadal artery
4. Ascending
- Suspensory ligament of Treitz (musculus suspensorius duodeni): extends from upper aspect of the
8. Define the surface anatomy of the small intestine along with its structures (3 subdivisions) and function
- Duodenum: C- shaped organ which receives openings of pancreatic bile ducts, measures approx. 25 cm, extends from pylorus on the right side → wraps around head/neck of pancreas → terminates left side of duodenojujunal junction; four parts (superior, descending, horizontal, ascending*)
- *suspensory ligament of treitz
- Jejunum: part of the midgut, proximal 2/5 of small intestine
- Ileum: part of midgut, distal 3/5 of small intestine, enters ascending colon at ileocecal junction
- J&I → suspended from posterior abdominal wall via mesentery
9. Describe the origin and ending of the small intestine and its location in relation to the other body organs/landmarks
- Duodenum: starts on @ pylorus (CC 9, L1, 1.25 cm R of midline);
- 1: liver and gallbladder anterior to 1st part of duodenum; bile duct and portal vein are posterior to it
- 2nd part lies anterior to renal vessels
- 3rd part lies anterior to IVC, aorta, right ureter, right gonadal artery
- 4th part: suspensory ligament attaches here and to the diaphragm + tissue around celiac trunk
- Jejunum
- suspended from posterior abdominal wall by mesentery
- Ileum
- enter ascending colon at level of ileocecal junction
10. Describe the wall structure of the small intestine
- Jejunum: few large loops, tall/large/closely packed plicae, deep red in color 2/2 greater vasculature long vasa recta
- Ileum: lots of short loops, pale pink in color, short vasa recta, sparse plicae, lots of lymphoid tissue
11. Explain the characteristics of the three different regions of the small intestine
- Duodenum: 4 parts → superior, descending, horizontal, ascending
- Jejunum: proximal 2/5 of small intestine
- Ileum: distal 3/5
12. Describe superior mesenteric artery syndrome
- Narrowing of the SMA angle w/ aorta → compresses third part of duodenum
- Normal range: 38-65 degrees