10 The Pharyngeal Apparatus
1. Pharyngeal Apparatus Formation (4th week embryo)
Pharyngeal arches are bulges in the head/neck region.
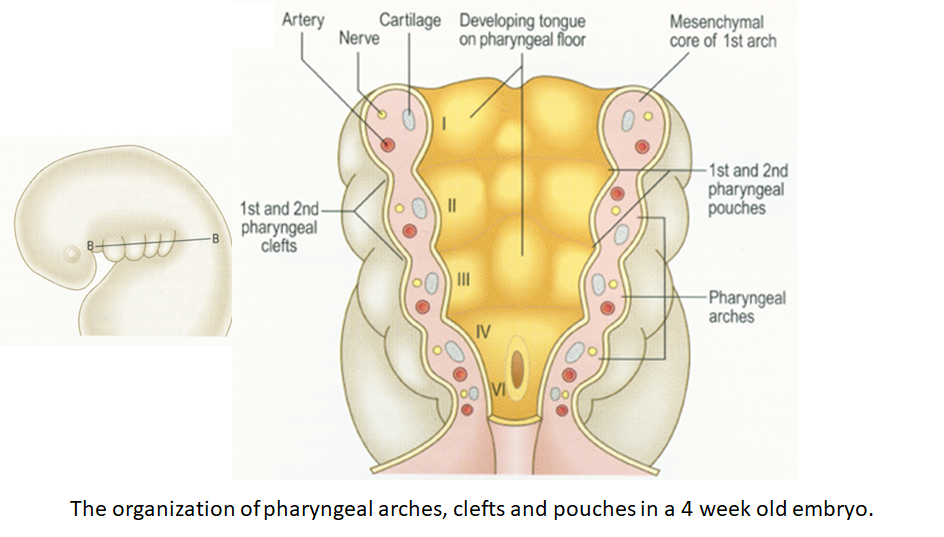
Each arch contains:
Mesoderm core (cartilage, artery, nerve)
Ectoderm (outer layer)
Endoderm (inner lining)
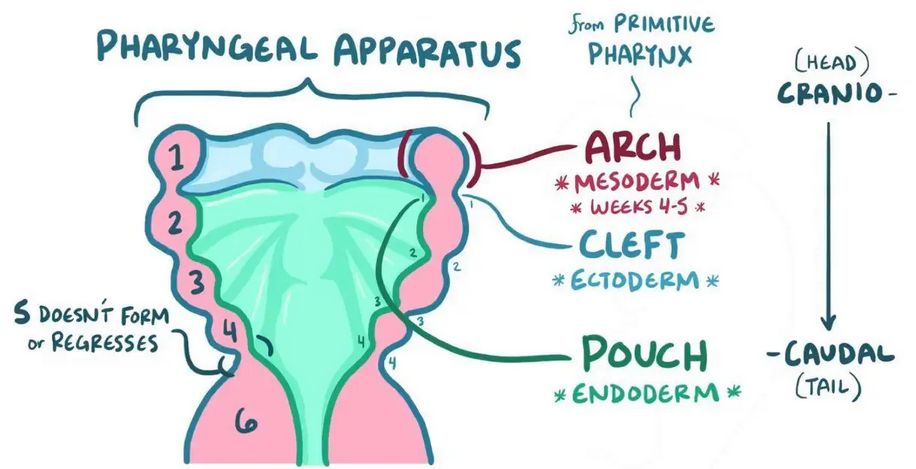
Mnemonic: CAP – Covers from C (clefts/ectoderm), A (arches/mesoderm), to P (pouches/endoderm)
There are arches 1–6 (but arch 5 disappears early).
2. Arch Innervation and Derivatives
Each arch is innervated by a cranial nerve. The arch-derived muscles stay innervated by the same nerve.
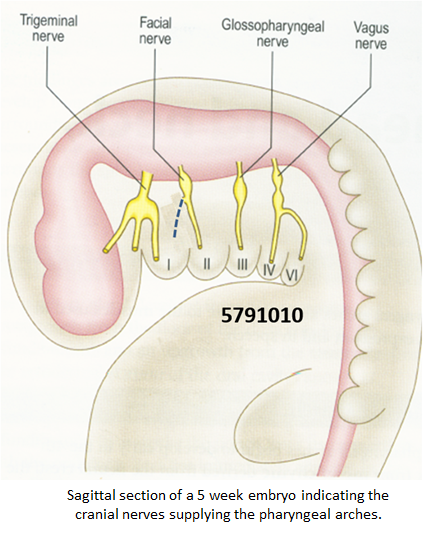
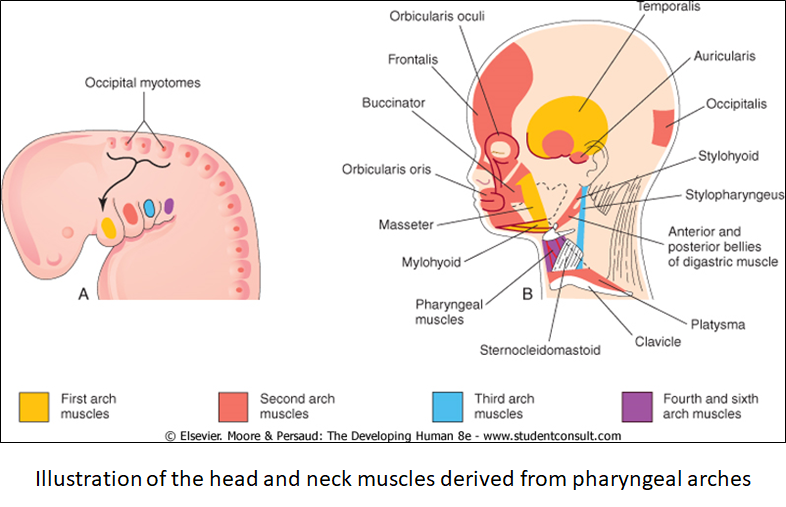
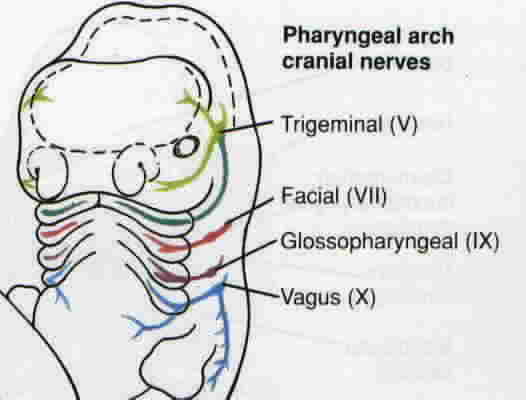
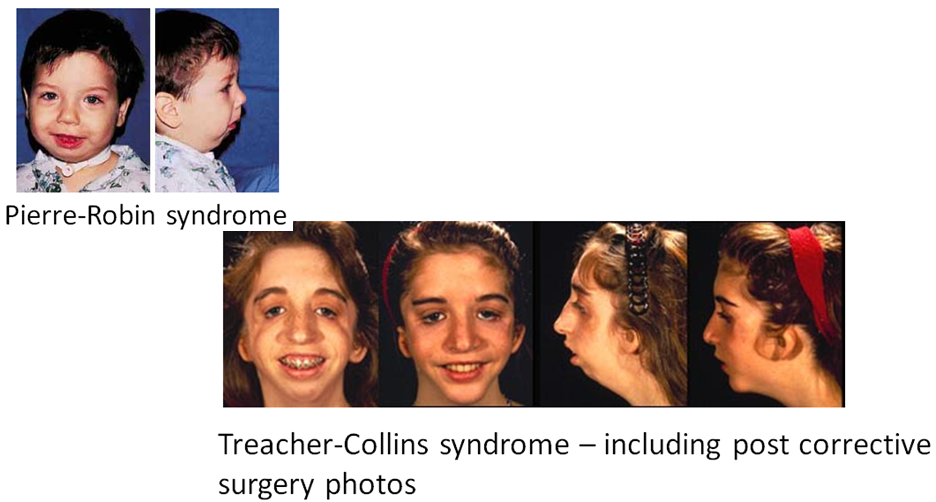
1st Arch (CN V - Trigeminal)
Muscles: mastication
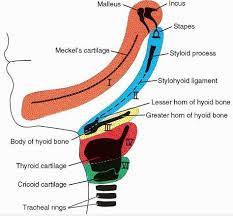
Cartilage: malleus, incus
Linked to Treacher-Collins and Pierre-Robin syndromes
2nd Arch (CN VII - Facial)
Muscles: facial expression
Cartilage: stapes, styloid process, part of hyoid
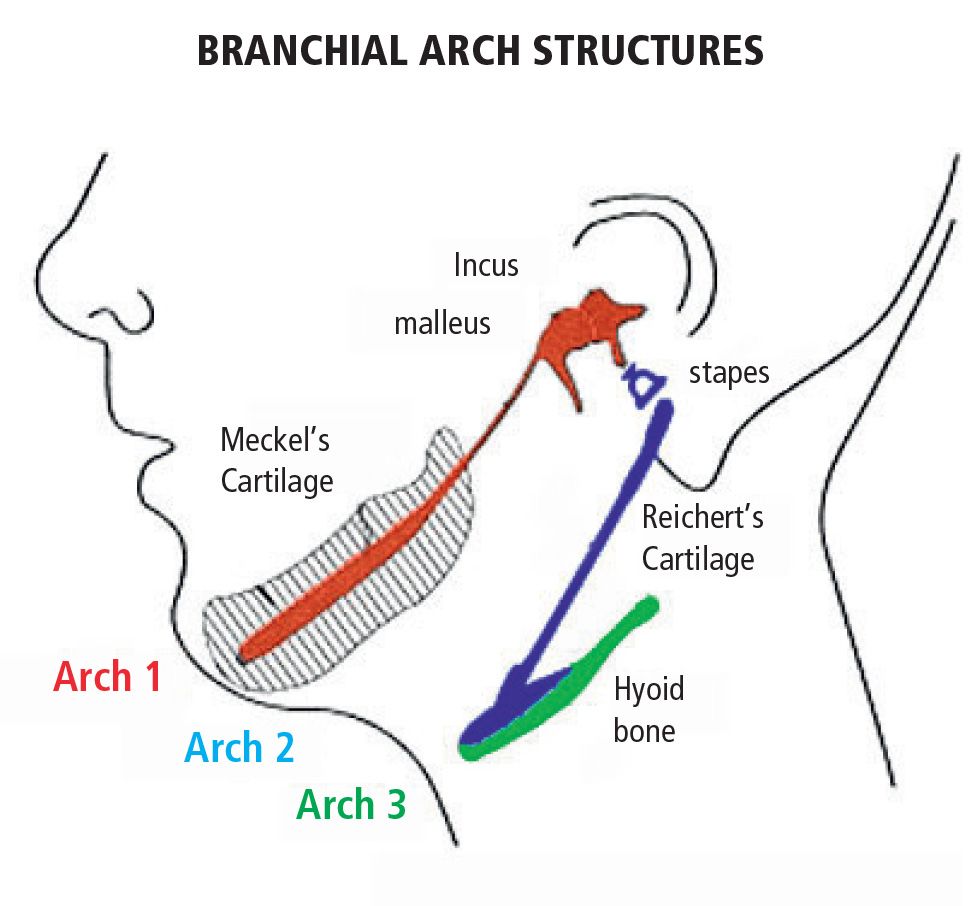
3rd Arch (CN IX - Glossopharyngeal)
Muscle: stylopharyngeus
Cartilage: part of hyoid
4th Arch (CN X - Vagus, superior laryngeal branch)
Muscles: pharynx, cricothyroid
Cartilage: thyroid, cricoid
5th Arch – disappears
6th Arch (CN X - recurrent laryngeal branch)
Muscles: larynx, esophagus (upper)
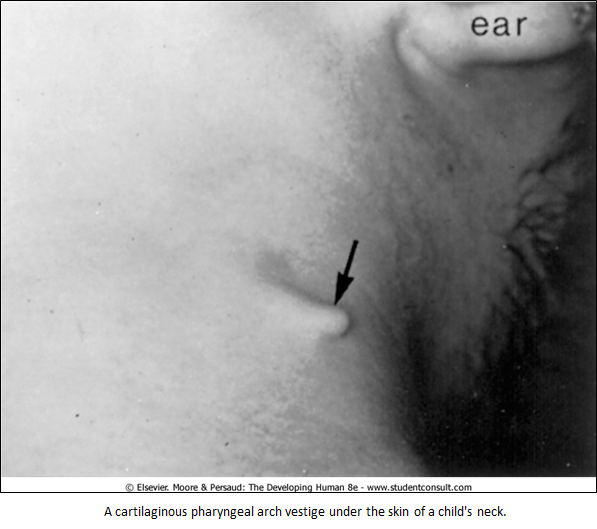
Vestigial cartilage remnants occasionally seen
Nerve mnemonic: 5791010
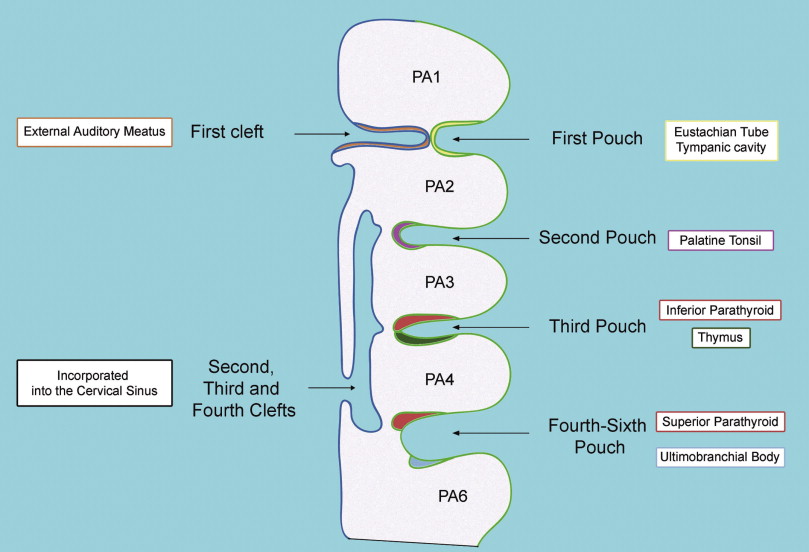
3. Derivatives of Clefts and Pouches
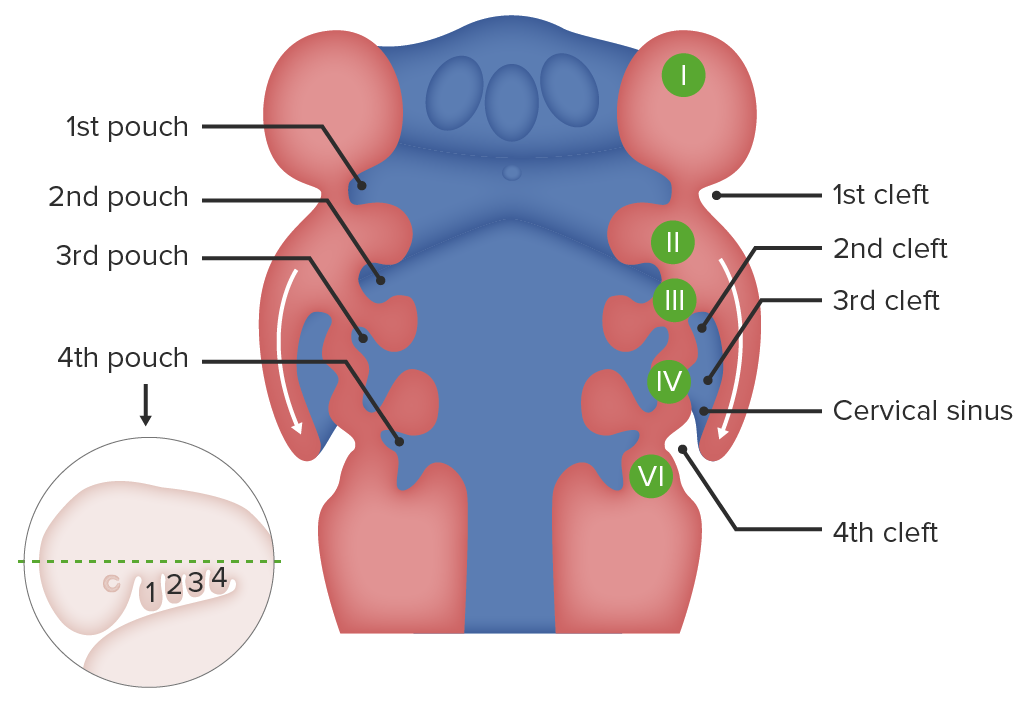
Pharyngeal Clefts (outside)
1st cleft forms external auditory meatus
Others usually disappear due to growth of 2nd arch covering them.
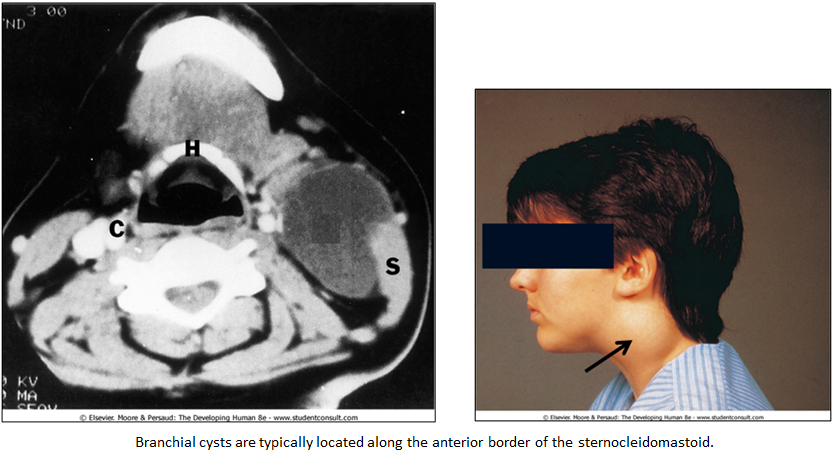
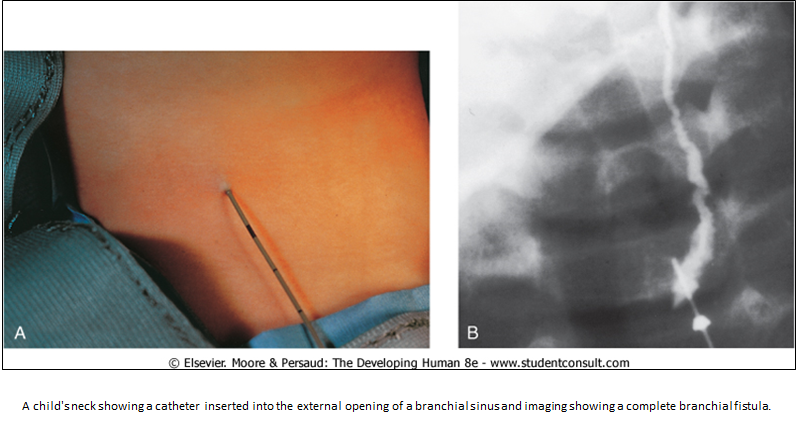
If persistent and does not degenerate → branchial cyst, cervical sinus, or fistula (see photos below)
Branchial cyst: 2nd pharyngeal arch failed to cover 3rd and 4th, leaving a remnant that forms a fluid-filled cyst along the anterior sternocleidomastoid.
Cervical sinus: Persistent space from incomplete fusion of pharyngeal arches; should regress during development.
Branchial fistula: Abnormal tract from persistent cervical sinus, opening to skin or pharynx.
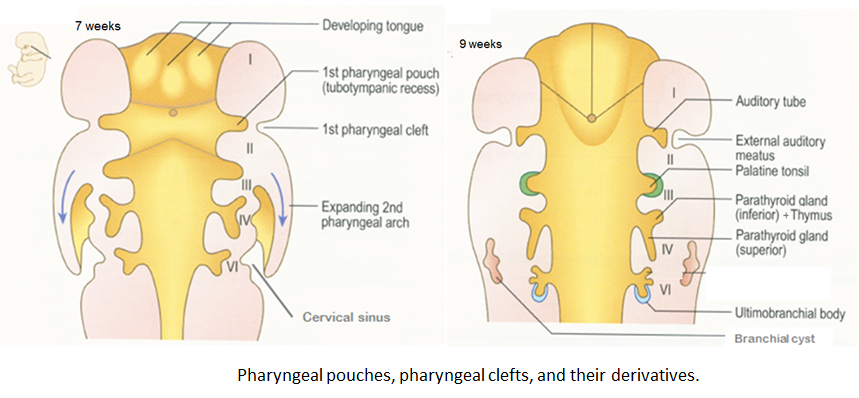
Pharyngeal Pouches (inside)
Mnemonic: 1A, 2P, 3TIP, 4ParaSP
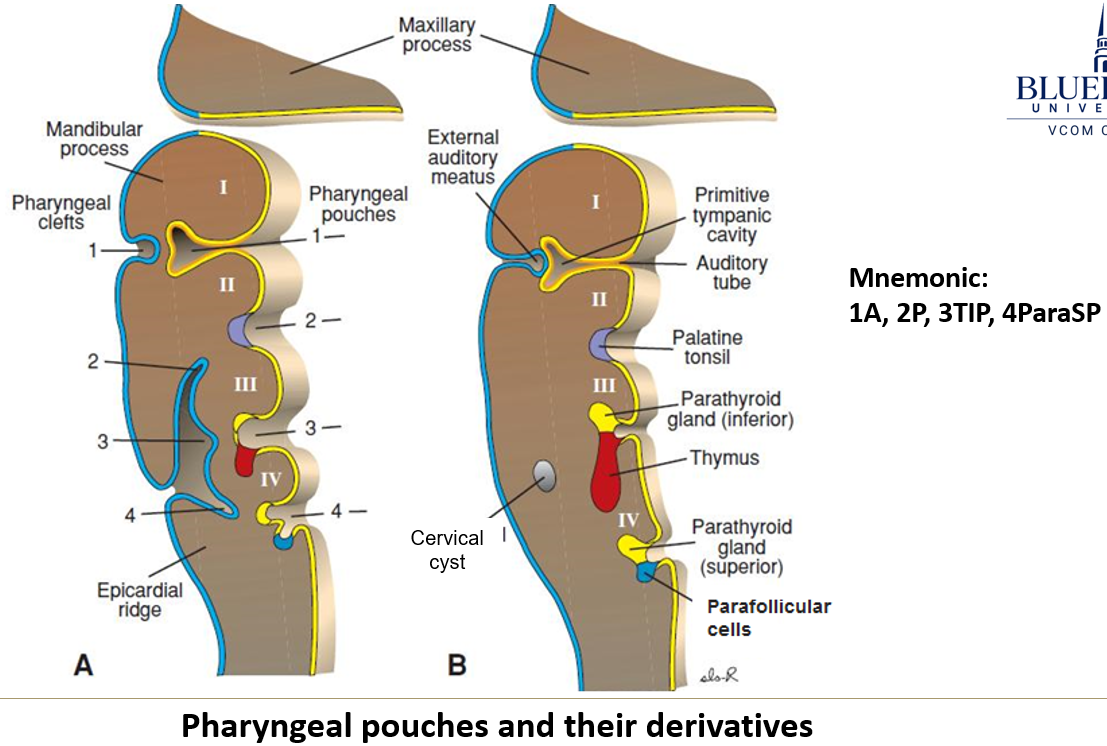
1st pouch = auditory tube, middle ear
2nd = palatine & pharyngeal tonsils
3rd = thymus + inferior parathyroids (migrate down)
4th = superior parathyroids + parafollicular (C) cells of thyroid
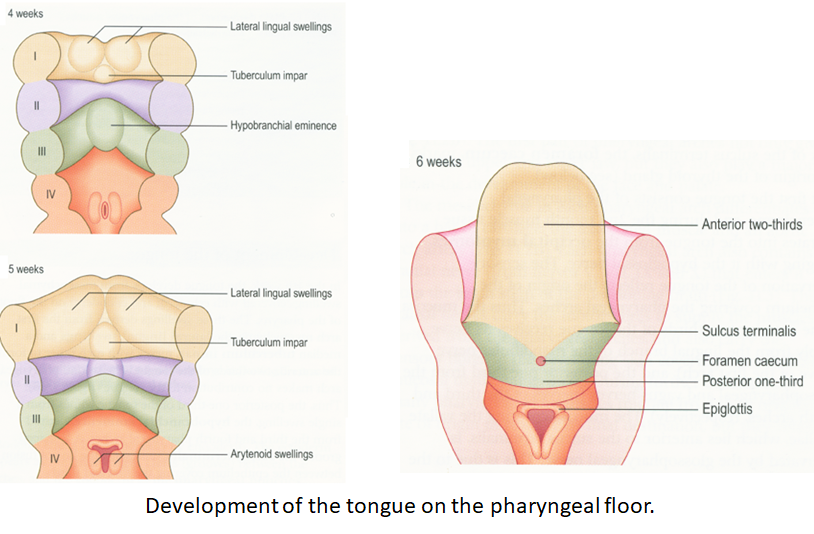
4. Tongue Development
Comes from 3 swellings that merge (Lateral lingual)
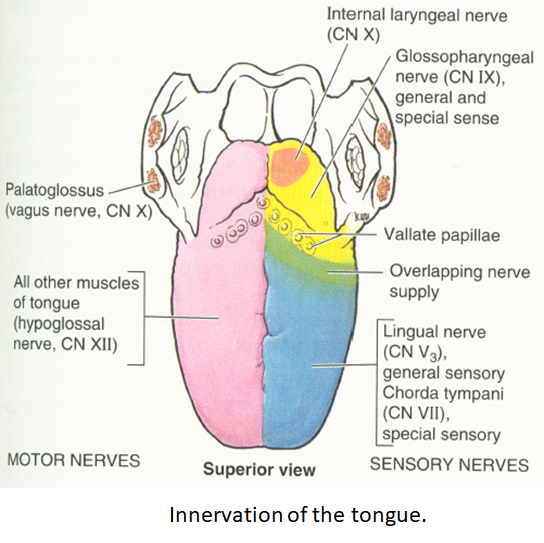
Anterior 2/3 (oral part) — Lateral Lingual Swellings
From 1st arch
Sensation: CN V
Taste: CN VII
Posterior 1/3 (pharyngeal part) — Hypobranchial eminience
From 3rd arch
Sensation + taste: CN IX
Muscle: CN XII (Hypoglossal), except 1 exception
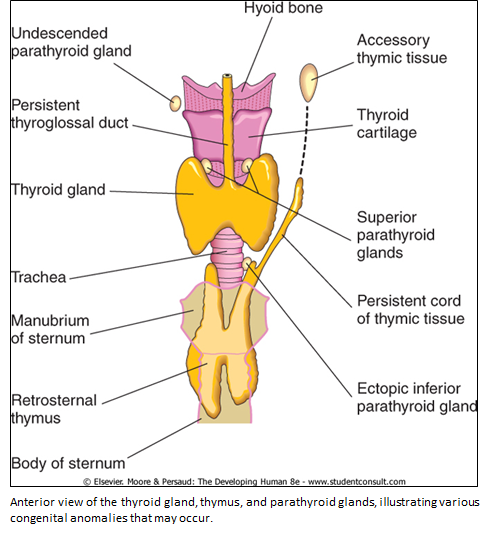
5. Thyroid Development
Begins at foramen cecum on tongue.
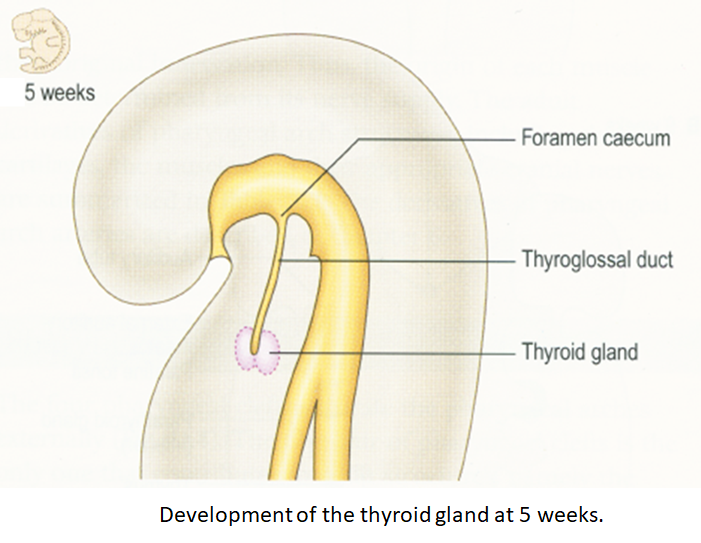
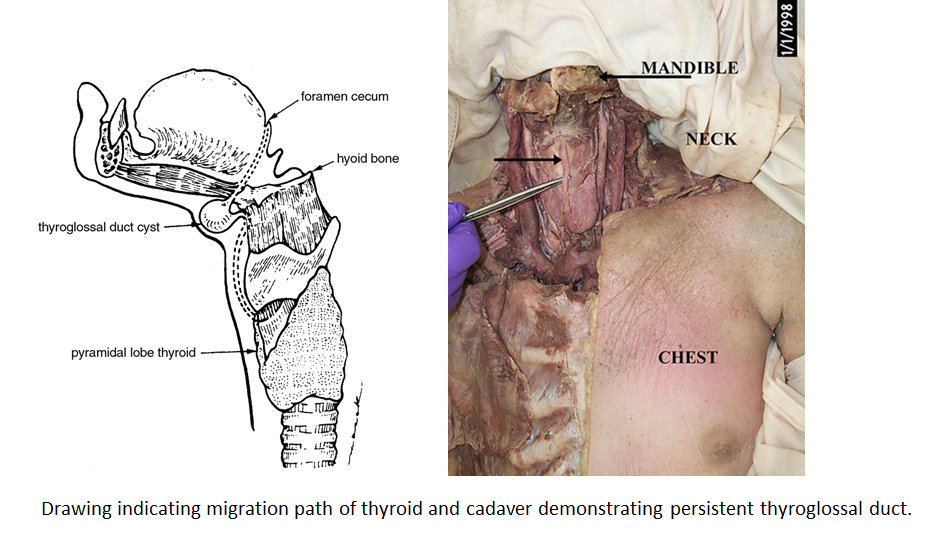
Then, migrates downward through thyroglossal duct, eventually settling in the neck.
Picks up cells from 4th pouch on the way.
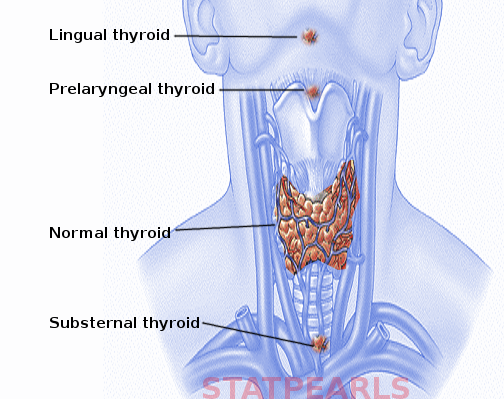
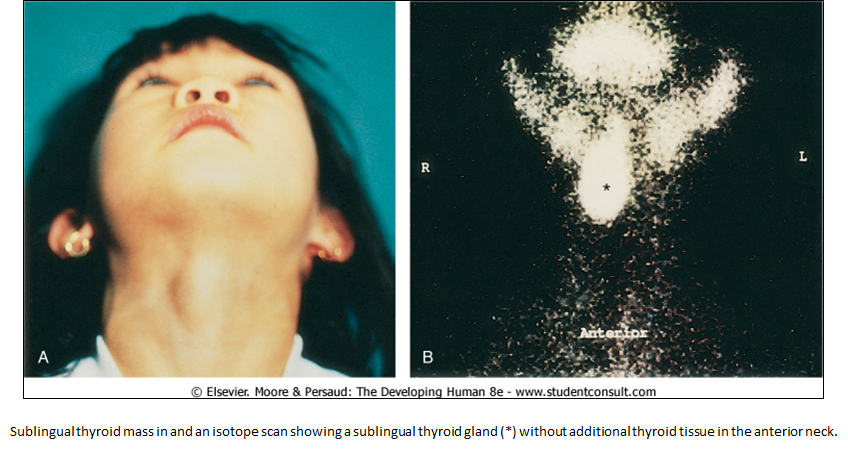
Issues with Thyroid development:
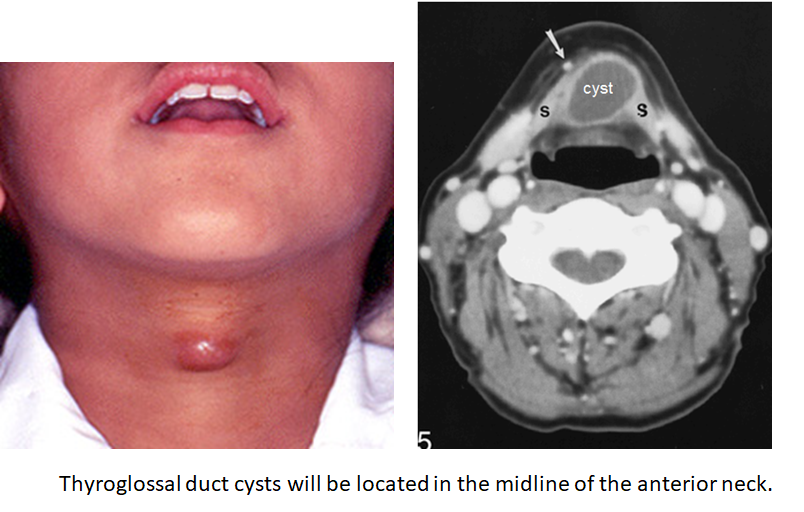
Thyroglossal duct cysts: If the thyroglossal duct doesn’t disappear, it can form a cyst in the tongue or front of the neck. If infected, it might drain through the skin called a thyroglossal duct sinus.
Ectopic thyroid: If the thyroid doesn’t migrate properly, it might end up in the wrong place or leave behind extra thyroid tissue (accessory thyroid) along the path it took.