mood disorders
overview of mood disoders
disturbances that cause subjective discomfort, hinder a persons ability to function, or both
why do we have emotions?
evolutionary psychiatry
emotions improve our reproductive fitness: “emotional benefit our genes far more than they do us”
overview of depression and mania
unipolar disorders vs bipolar disorders
depressed←——→ mania
spectrum
unipolar: too much depression or too much mania
bipolar: swings back and forth on the contiuum
normal mood variation: not static, varies across times
three elements: depth (how high or low your mood varies), variability, and reactivity
unipolar disorders
major depressive disorder: depth is extremely low and variability is very low
major depressive episode
affective symptoms
extreme depression
cognitive symptoms
rumination
negativism
death or dying
behavioral systems
anhedonia
psychomotor retardation
physiological systems
low energy
sleep disturbances
appetite and weight changes
somatic symptoms
have to have symptoms for 2 weeks
prevalence of depressive disorders
MOST common: 19 precent of population at some point
onset: mid 20s
more women than men (21% vs 12%)
controversial developments in mood disorders
persistent complex bereavement disorder→ understudy (overcomplicated greif)
disruptive mood dysregulation disorder→out of proportion temper outbursts
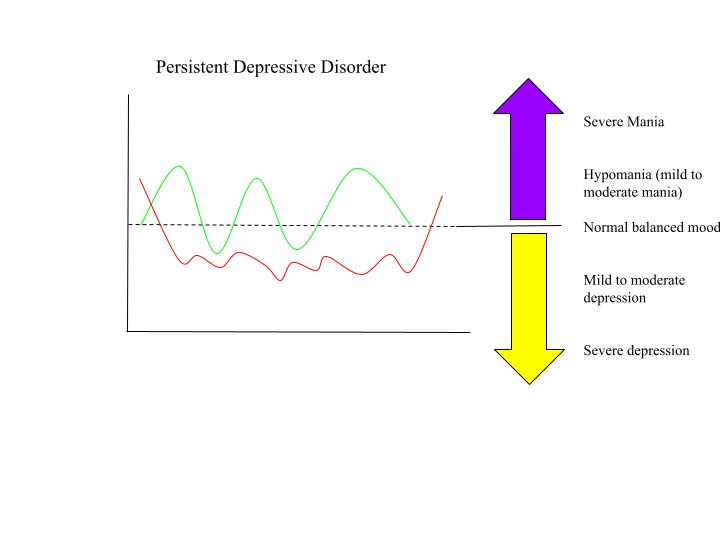
persistent depressive disorder (dysthymic disorder)
have symptoms for 2 years
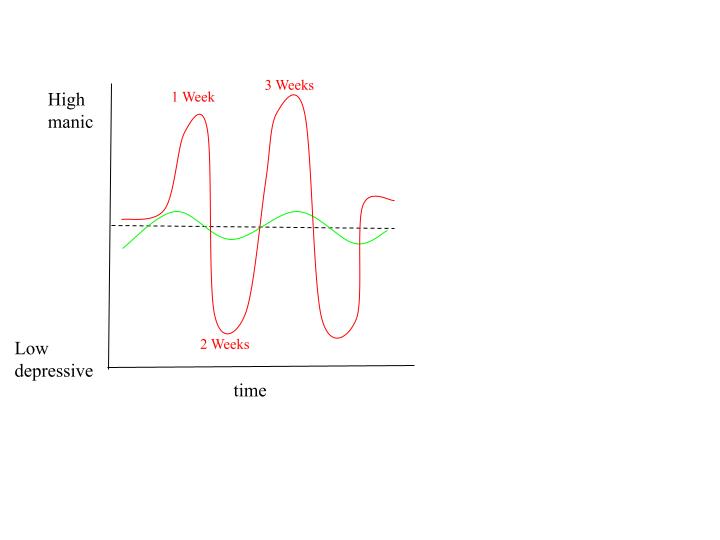
Bipolar disorders:
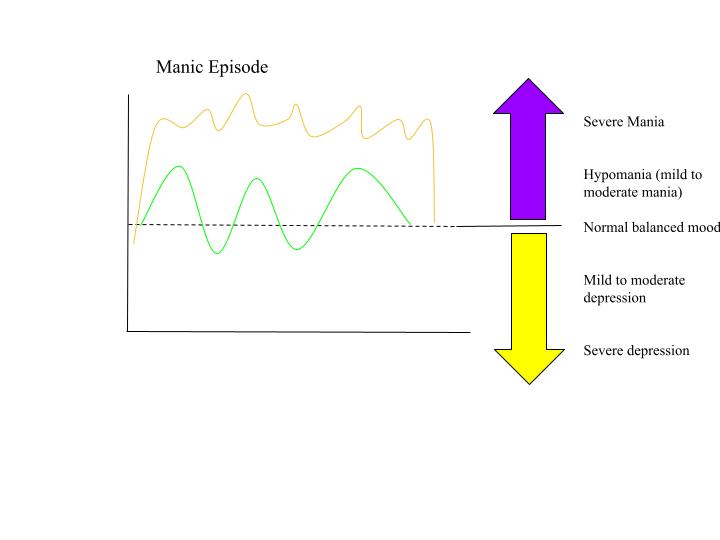
manic episode: 1 week
exaggerated elation, joy, euphoria
1 week or less→ less: if institutionalized, brought to jail(dont have to wait to say its a manic episode)
cognitive symptoms
increased self-esteem or grandiosity
flight of ideas
distractibility
physical dysfunction:
decrease need for sleep
hyperverbal
increase goal oriented activities/activities with high chance of bad outcome
hypermanic episode (4 days)
bipolar disorder I
alternating major depressive and manic episodes
single manic episode
recurrent
symptoms free for 2 months
bipolar disorder II
alternating major depressive and hypomanic episodes
cyclothymic disorder
alternating mild manic and depressive episodes
similar to bipolar II but less severe
two years of mood swings, no more than 2 months without symptoms
RARE 0.4%
15% to 50% progress to bipolar I or II
etiology of mood disorders:
similarities between mood and anxiety disorders: distress
both share a “general affective sense of distress”
studies have found a high degree of comorbidity between anxiety and mood disorders
GAD and MDD share common genetic diathesis
mood as a thermostat
moos has a purpose (evolutionary)
anxiety = smoke alarms, mood = thermostat
we have natural set-points
problems occur when the ability to regulate mood fails
biological perspective:
genetics and family studies
5-HTTLPR is a region on the gene which codes for serotonin transportation
in humans → it codes as short or long
short allele (variation) associated with neurocitism
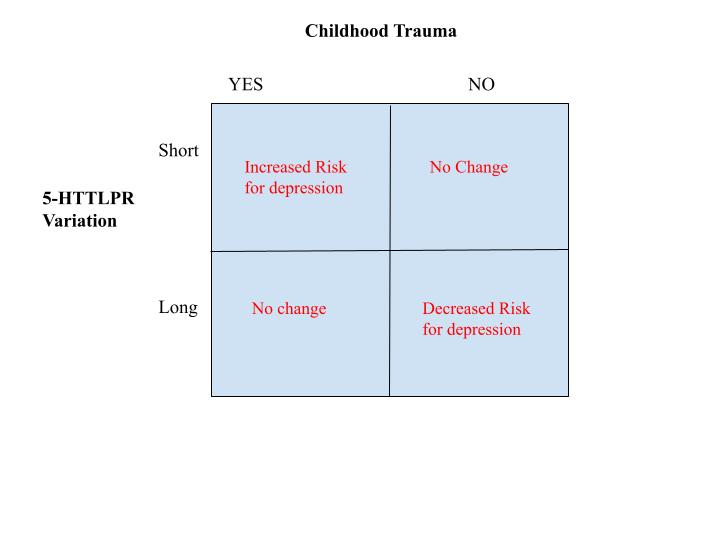
gene x environment interaction
short allele + childhood trauma = increased risk for depression
medication that works for parents Major Depressive Disorder(MDD) usually works for the child with MMD
biochemical
deficits in serotonin, norepinephrine, and dopamine
tricyclic antidepressants → circa 1950
NOTE - casual relationship still speculative
REM sleep disturbances
too much too little increase risk
increased REM associated with depression
Psychological models
psychodynamic theory of depression:
oral stage: needs were either not met or over satisfied. spend their lives searching for love and approval
real or imagined loss
anger turned inwards
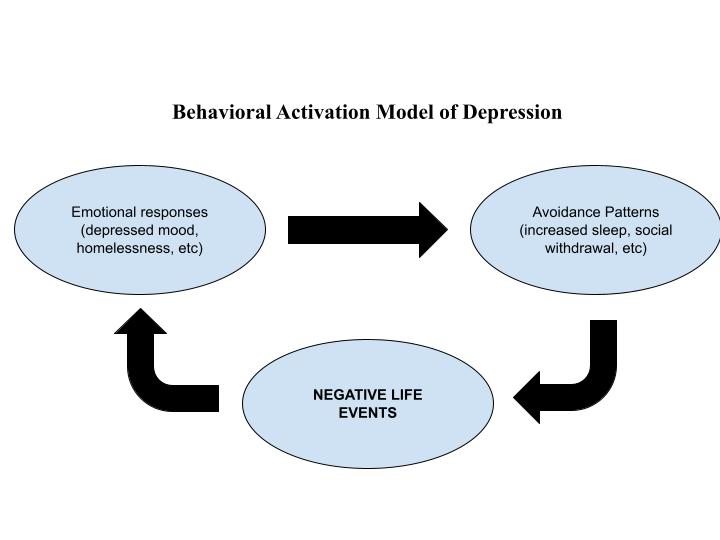
behavioral theory of depression:
reduction in the amount of reinforcement is the cause and leads to less activity (lewinsohn)
cognitive theory of depression
founder aaron beck
“depressives suffer from a kind of basic thinking that distorts reality”
thinking and depression by aaron beck 1963 (founder of cognitive theory of depression)
descriptive research
thematic content of cognitions
occurred in response to things and in “free associations”
characteristics of depressive cognitions (NOTE: not just the content of the thought but thinking patterns in general)
automatic
plausibility to patient → patients believed thoughts in head
preservation → thinking about the thoughts again and again
unable to not think about something else
depression is in the thoughts not in the genetics
etiology of mood disorders(aaron beck):
early childhood experiences can lead to the formation of dysfunctional beliefs
which in turn lead to negative self views and automatic thoughts
which in turn lead to depression
triad of mood disorders (Aaron Beck) → cognitive model
learned helplessness and depression → cognitive schemas: Seligman(person)
depression results from loss of control
attribution style
people who feel helpless make speculations (causal attributions) about why they are helpess
internal/external, stable/unstable, global/specific
example: walking and trip on the side walk
internal: i am a klutz
stable: i am always gonna keep failing
global: no matter where i go i will fall
external: the sidewalk had a crack in it
unstable: not gonna fall next time
specific: it is only this piece of concrete that i will fall
seligman dog experiment
some dogs were placed in a chamber where they received electric shocks from which they could not escape (the non-escape condition)
the dogs in the escape group could escape the shocks by pressing a panel with their nose.
in the second phase, the animals were placed in a shuttle box divided by a barrier in the middle so that the dogs could jump in order to escape the shocks. only the dogs that had learned to escape in the previous phase tried to jump. the other dogs did not attempt to
when the the dogs in the “non-escape” condition were given the opportunity to escape the shocks by jumping across a partition, most failed even to try; they seemed just to give up and passively accept any chocks the experiments chose to administer
in comparison, dogs who were previously allowed to escape the shocks tended to jump the partition and escape the pain.

treatment of mood disorders:
approximately 85% of people who receive treatment for depression improve
4 types of treatment: work well in combination
medication
psychotherapy
electroconvulsive therap
transcranial magnetic stimulation (TMS)
medication: major depressive disorder
selective serotonin reuptake inhibitors(SSRI)→ prevent reabsorption of serotonin into neighboring cells
time: does not take effect right away →2-4 weeks before medication reaches full effect
depends on person and type of medication prescribed
side effects
close to 50% of people who take medication stop because of side effects
blood pressure, glucose level, sexual side effects (ED, and decrease sex drive)
50% of sample respond to first antidepressant; 70% to the second and 90% to the third
treatment non-responders = chronic depression or misdiagnosis
chronic depression → cannot be treated by medication
medication: bipolar disorder
lithium (naturally occurring metallic element)
very small therapeutic window → must give exact right amount of medication for it to work without side effects
anticonvulsant: anti-seizure medication
atypical antipsychotics: only be used when person is in a manic episode
electroconvulsive therapy(ECT)
psychotherapy
cognitive therapy:
identify errors in thinking
correct negative cognitive schemas
behavioral activiation:
increased positive events
exercise
electroconvulsive therapy (ECT)
what is it?
brief electrical current
temporary seizures
the longer the seizures, the more effective the treatment
6-10 treatments
typically done in an operating room→ put patient under general anesthesia
high efficiency → severe depression
few side effects
effectiveness is 70% to 90% but studies vary
once it is effective, patient has decreased need for medication
need to consider cost-benefit analysis
advantage: effective
disadvantage:
not effective forever, some people might have to get it redone every 6-12 months (not all)
side effects: memory loss (for 24-48 hours), headaches
transcranial magnetic stimulation (TMS)
around for 10 years, novel antidepressant treatment
mechanism of action (how it works) is not clearly understood
variation in diagnostic criteria
lack of solid biomarkers in depression
“the effect size TMS antidepressant efficacy is at least comparable to those of antidepressant medications”
outpatients office, put electromagnetic coil into certain parts of brain and fire magnetic field