Kidneys
Why do we need kidneys?
· Salt and water homeostasis
· Excretion (kidneys are the most important excretory organ)
o Removing things from the bloodstream (a perfect blood scrubber must be able to remove anything from the blood)
§ Toxins, new molecules, inert substances (unreactive)
o The only way to be certain of excreting anything is to excrete everything and then reclaim the things that you need
Excretion
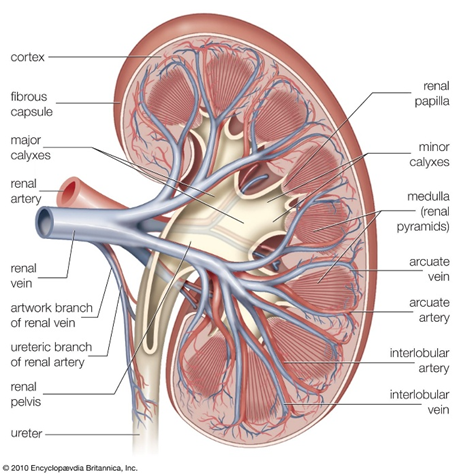
· Renal anatomy and blood supply
· Filtration
· Reabsorption and secretion
The kidney receives 25% of cardiac output (1200ml/min)
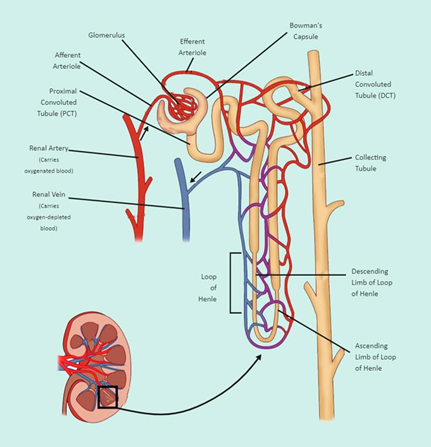
Nephron
- The functional unit of the kidney (1.5 million per kidney)
· Renal reserve is at least 50% and you can have renal sufficiency until you've lost about 85% of your nephrons
The blood supply is really important to a nephron as it is a blood scrubber.
Collecting duct
· Collect the urine from many different nephrons
· Eventually become the ureter
The interlobular arteries divide into about 50 glomerular capillaries inside the Bowman's capsule
Kidney: artery -> arterioles -> capillaries -> more arterioles
The glomerular capillaries drain into efferent arterioles, not venules (Portal system)
- emptying into very tight vessels on the outside of the glomerular capillaries
The difference between nephrons is in the length of the loop of Henle and the vasa recta.
· Most nephrons have a short one which just reaches the cortex medulla junction
· About 15% have very long loops - which are much more important in producing hypertonic urine (juxtamedullary)
Starlings forces
- What drives fluid through, in and out of capillaries
Not in the kidney:
Pc = Capillary hydrostatic pressure
Πc = Capillary osmotic pressure
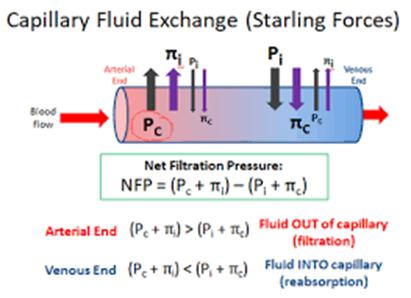
Net = Pc - Πc
Arterial end: Pc is high and higher than Πc so there's a net force for efflux. Fluid/oxygen/etc is pushed out into the organ
Venous end: Pc drops and is lower than Πc so there's a net force for influx. Interstitial fluid/CO2 is pushed back into the capillaries to take away
In kidney: (glomerular)
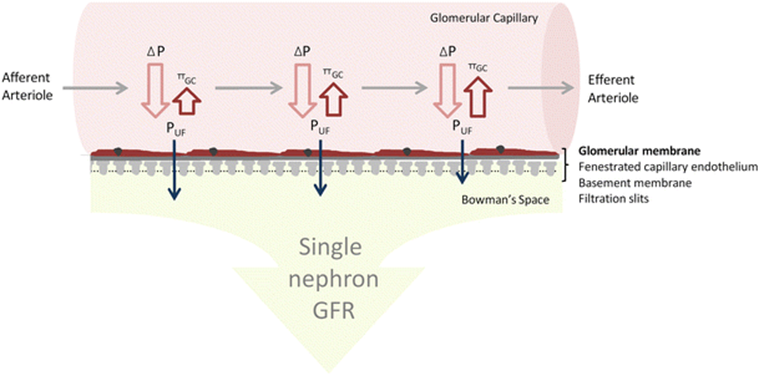
The reason for no change is because it drains into the efferent arterioles.
- Very high pressure vessels so there is little or no drop across the capillary bed
As you're taking some fluid out of the capillaries, the osmotic pressure goes up but you still have a balance for net efflux.
In a glomerular capillary, the Starling's forces are positive for efflux all the way along in order to keep fluid moving out of them.
Filtration barrier
· Capillaries (with windows) – Fenestrated capillaries
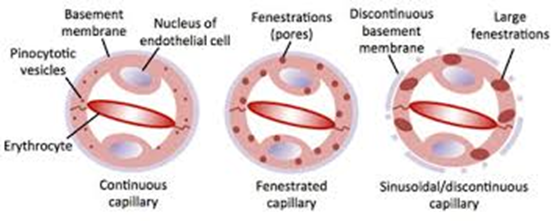
Permeable to substances <100nm
· Base membrane
· Podocytes
Podocytes are kidney cells that sit on top of the capillaries and form part of the barrier
All three barriers work together to form a functional barrier
· They are not a barrier to water (no resistance)
· Also allow small molecules (Na+) <7000Da, <4nm through (glucose, amino acids, sugars, ions, etc)
· Large molecules >70000Da, >8nm do not get through and are retained in the blood (blood proteins, blood cells)
o Albumen is a blood protein at 60,000Da and it's completely excluded from urine as the basement membrane has a negative charge which repels albumen’s negative charge
UTI
You lose the negative charges on your basement membrane so albumen appears in the urine. This can be used to diagnose a UTI assuming the kidney is healthy.
All the ions, water, sugar, amino acids, etc, are pushed out of the capillaries, across the filtration barrier, driven by Starling forces and then get trapped inside Bowman's capsule. It then exits via the proximal tubule to form primary urine. Primary urine has all the things we desperately need to live.
Reabsorption
The proximal tubule employs active transport techniques to recover the molecules you want to get back (amino acids, glucose, etc)
E.G. Glucose circulating in your blood would get filtered into the urine and the proximal tubule takes it back by active transport
Active transport
Unidirectional movement of sodium
The sodium pump pumps sodium Na+ out of the epithelial cells, creating an inwardly directing sodium gradient. This provides the energy gradient to energise sodium-glucose cotransport.
Glucose then goes out of the cell through a facilitated transport mechanism. It brings down the glucose gradient into the bloodstream.
There are two SGLTs, which are the sodium-glucose transporters:
· SGLT 1 is a high affinity sodium-glucose transporter which you see in Section 3 of the proximal tube (also found in the small intestine)
· SGLT 2, which is a lower affinity transporter that you see in sections one and two of the proximal tubule
The proximal tubule is divided into 3 sections:
· S1 is closer to the glomerular capillaries
· S3 is closer to the vasa recta
Primary urine will be packed full of urine (up to five millimolar) so you don't need a high affinity transporter to recover that. SGLT 2 transporter pick up loads of glucose and any little bits left are picked up by SGLT1. By the end of the proximal tubules, there is no glucose left.
Unidirectional movement of sodium and movement of glucose to build the osmotic gradient across the proximal tubular cells. This will move water.
When you move and recover the glucose, you're also able to recover the salt as well. This creates an osmotic gradient and recovers the water.
No matter how much glucose we filter out, we can recover it through active transport.
The proximal tubule deliberately takes actively secretive substances from the bloodstream and concentrates them in the proximal tubular cells so that they end up in the urine at really high concentrations.
Filtration moves about 20% of any substance on a single pass through the kidneys - the blood goes to the kidney and 20% of the blood ends up in the urine.
This would take about one hour to remove 90% of any substance by filtration alone as it would take several passes through the kidney. If you actively secrete a substance, you can get rid of 90% on a single pass, which is much faster.
If there's something that is known to be toxic, then the active secretory process means that as soon as it appears in the bloodstream, it is filtered and secreted so it is gone in one go.
There are two basic secretory processes: one for organic cations and one for organic anions.
The one for organic cations is driven by the membrane potential.
Organic anion secretary process
Organic on my own is anything that has carbon in it and one charge that is small and transportable e.g. DDT, antibiotic, uric acid, etc
The energy-dependent step for this is an anion exchange process on the basolateral membrane.
Dicarboxylic acids, such as alpha ketoglutarate, are exchanged out of the cell and organic anions come in. Therefore, there is an outward-facing gradient for dicarboxylic acids so that they are providing the energy for anions to come in.
The dicarboxylic acid gradient is taken up across the basolateral membrane by a sodium-dependent process.
· Dicarboxylic acids circulate around the basolateral membrane.
Organic anion exchange is loosely coupled to the sodium gradient (an active transport process).
· Identified by John Pritchard and Dave Miller who worked for NIH
o It was done in the mid 1980s and came up with a model for organic anion secretion
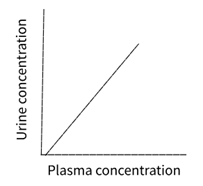
· Filtered, not secreted, not reabsorbed
· No limit to filter
· E.g. Insulin – inert, small polysaccharide
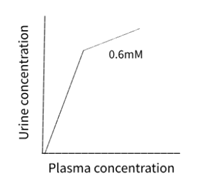
· Filtered and secreted
· Urine concentration goes up more rapidly as it is being secreted
· E.g. Para amino hippuric acid – organic anion not so toxic
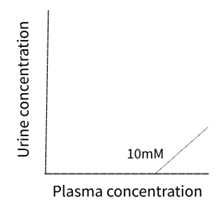
· Filtered and reabsorbed
· The concentration in urine doesn't increase because it is being reabsorbed
· E.g. Glucose
· Lines for PAH and glucose stop halfway as this doesn't carry on forever. As you increase the concentration of substrates, PAH level of secretion levels off (at 0.6mM) and glucose starts to appear in the urine (at 10mM)
· The lines in all three graphs become parallel as at high concentration, all these substances are being treated the same way (filtered, not secreted, not reabsorbed)
· This is because absorption and secretion or active transport mediated processes, and you can saturate them
· It will move as much as it can, but any excess will simply not be transported
o For PAH, the transfer maxima is 0.6mM (anything above that will not be secreted)
o For glucose, as it is much more important, transfer maxima starts at 10mM (anything above that will start to appear in the urine, not reabsorbed anymore)
Glucose in the urine
· Glucose is reabsorbed until the active transport process for glucose is saturated at its transfer maximum
· Glucose first appears in the urine at a plasma concentration of 10mM (renal threshold)
· Saturation occurs at a plasma glucose concentration of about 14mM. No additional glucose can be reabsorbed
· Glucose appears in the urine
· Diagnostic sign of diabetes mellitus (very high blood sugar)
o WHO Defines diabetes as a fasting plasma glucose (FPG) of more than 7mM (below renal threshold)
o It is much easier now to measure blood sugar than wait until the blood sugar exceeds the renal threshold to diagnose
o If you have sugar in your urine or your blood sugar is more than 7mM per litre, then you're diabetic
The normal range of FPG is 4-5. 5mM
Between 5.5-7mM is pre diabetic and almost all the people who are pre diabetic have type 2 diabetes, and one of the major causes is lifestyle/obesity.
Pre diabetes is possible to reverse by losing weight or changing diet
Consequences/Comorbidities
· Guillotine amputation - limb can go gangrenous as the blood supply isn't sufficient
· Renal problems - affect the kidney
· Vision impairment
Test
· Glucose tolerance test
· Haemoglobin A1C test (HbA1c)
Filtration and reabsorption
· The kidney filters a lot of sodium ions (26 moles a day)
· It recovers 99.4% of it
· It philtres 18 moles a day of Cl-
· It recovers 99.2 percent of it
· 4.9 mol of HCO3- a day
· It recovers 100% of it
· 0.6 mole of potassium ions a day
· It recovers 99.3% of it
· 0.8 mole of glucose a day
· It recovers 100% of it
The kidney does salt and water homeostasis, but is evolved to excrete things
Water absorption
· 180 litres of water go through your kidney each day
· It recovers 99.4% of it
· Four to five times your total fluid volume
o Blood is going through the kidney and filtering it five times a day
Salt and water homeostasis
· Two easily regulated determinants of body osmolarity or body fluid volume
o The amount you drink, regulated by your brain, which you take in through your gut (1.5l/day)
The amount of fluid you lose in your urine, which is the provenance of the kidney (1.5l/day)
Osmolarity is the number of osmotically active particles in solution.
Example: average male weighing 70 kilograms
· Body fluid compartment of 40 litres
· Normal osmolarity of 300 mOsmol per litre
· Urine produced is 1.5 litres per day
· A mOsmol is 1/1000th of an Osmol
· Ions dissociate in solution therefore: 150mM NaCl = 300mOsmol/L
o If body fluid compartment is less than 40 litres
o His osmolarity is high (same amounts of salt, less water)
o Fluid = water, not salts
An increase in osmolarity is detected by osmo receptors in the hypothalamus. It then reacts in two ways:
· Releases anti diuretic hormone (ADH) from the pituitary which causes the kidney to preserve fluid which reduces your urinary flow rate to a theoretical minimum of 0.5l/day.
It will also cause you to feel thirsty and therefore, increase fluid intake to rapidly bring the fluid back to 40 litres
o If body fluid is more than 40 litres
o Osmolarity is low (same amount of salt, more water)
A decrease in osmolarity is also detected by the hypothalamus
· It stops/reduces the amount of ADH it produces, which causes the kidney to lose more fluid and increase your urinary flow rate to a theoretical maximum of 23 litres a day.
Your fluid volume goes down to normal and then there's a recovery.
= NEGATIVE FEEDBACK LOOP
Negative feedback loop
You can change the osmolarity on the behaviour of the kidney.
It changes to compensate so you return back to where you were before
At rest
· Urinary flow is 1.5 litres a day
This implies that there's a lot of ADH produced under normal circumstances.
Hormone levels set at an intermediate point so that regulation can occur in both directions
Low in NA+/NaCL
· Low in sodium means your osmolarity is low
· Less salt, same amount of water
o Low as molarity is detected by the hypothalamus, which will increase the amount of ADH and therefore, increase the fluid loss through urine so your volume goes down (<40l)
o Now there is low salts, low fluid, but normal osmolarity, which is more important in terms of homeostasis
The kidney compensates for low salt levels by reducing fluid volume so osmolarity is preserved (short term, ranged)
· There must be an appropriate corrective mechanism
Water reabsorption
· Every part of the nephron does some form of water reabsorption.
Proximal tubule: 180 litres a day gets filtered and 127 litres a day gets reabsorbed (70.5%)
Loop of Henle: 10 litres a day gets reabsorbed (5.5%)
Distal tubule: 20 litres a day gets reabsorbed (11%)
Collecting duct: 23 litres a day hits the top of the collecting duct
· If nothing else happened, 23 litres a day would be lost in urine
In the presence of ADH, the collecting duct is water permeable.
In the absence of ADH, the collecting duct is not warped to be permeable so water would go straight on as urine.
Anti diuretic hormone = Anti water loss hormone
· AKA arginine vasopressin
ADH binds to AVPR2 receptors that stimulate the insertion of AQP2 channels into the apical membrane of collecting duct cells.
This reabsorbs 22.5 litres a day (12.5%)
This leaves urine producing only half a litre a day
Therefore, there must be an osmotic gradient between the collecting duct and the medulla.
· The medulla must be of a higher concentration than the collecting duct to draw the water out
Standard blood concentration: 300mOsm/L
In the loop of Henle
Fluid circulates in the loop from the cortex to the medulla.
It then goes into the collecting duct.
If you added ADH, nothing would change as there's no driving force.
The sodium pump is crucially important:
· It is on the ascending limb of the loop of Henle and is pumping sodium ions out of the loop into the interstitial space. This increases the concentration in this space
· The ascending and descending limbs have equilibrium between each other. Therefore, this increases the amount of sodium that's going into the descending limb of the loop
· This increases the concentration going up into the ascending limb, which then meets another sodium pump
Acid/Base Balance
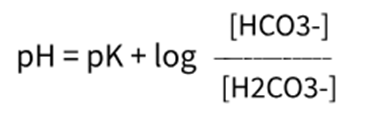
Henderson-Hasselbach Equation
The whole of our blood runs on a bicarbonate buffer system.
Circulating bicarbonate concentration is in equilibrium with carbonic acid and if you know the constant for that relationship, you can work out the pH
· A bicarbonate buffer system is the dominant buffer system
Carbonic acid concentration is largely determined by the partial pressure of CO2 (which is regulated by the lungs)
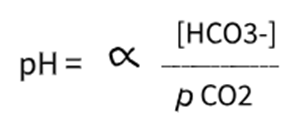
HCO3- is regulated by the kidney.
If you need to change the pH:
· Change the rate of breathing to change the partial pressure of CO2
· Change the amount of bicarbonate the kidney is excreting
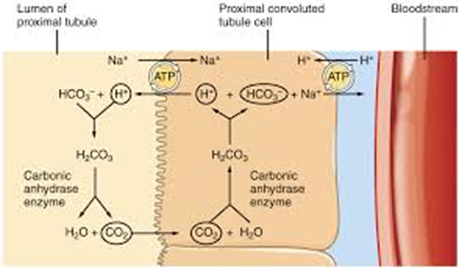
· The sodium pump pumps sodium out of the cells, creating an inwardly directed sodium gradient
· In the urine, bicarbonate and protons will be in equilibrium with carbonic acid. This will be in equilibrium with CO2 and H2O
· To make carbonic acid from CO2 and H2O is really slow, but there's an enzyme, carbonic anhydrase, which is secreted by the proximal tubular cells, that enhances the rate that CO2 is made from carbonic acid
· The CO2 is membrane permeable so diffuses into cells
· It then combines with H2O to turn back into carbonic acid, which then dissociates into H+ and HCO3-.
· The bicarbonate is then taken across the basolateral membrane
· The protons cycle back across the apical membrane and exchange for sodium
· This is then what drives H+ + HCO3- -> H2CO3
The effective transfer maximum of this process is 25mM per litre, which is the normal concentration of bicarbonate in the blood
· If your bicarbonate concentration goes up, your kidney doesn't absorb it
Too low
· CO2 is coming from the blood and diffusing into the cells
· It forms bicarbonate, which leaves the cell, and protons, which are being cycled across the apical membrane
· Ammonia in the urine binds to the proton to form ammonium
NH3 + H+ -> NH4+ (NHS Comes from metabolism of proteins)
· Ammonium is then excreted out in the urine
You can regulate the amount of bicarbonate you excrete by regulating the amount of ammonia you make
The kidney can manufacture bicarbonate to regulate body pH. This occurs in the stomach too
Renal Endocrine Functions
The kidney is an endocrine organ at the juxtamedullary apparatus (where the glomerular capillaries come against the distal tubules)
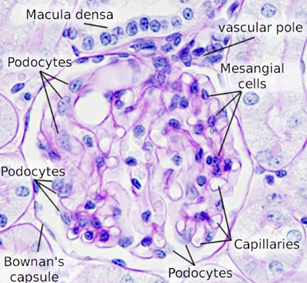
Juxtaglomerular Apparatus
· Mesangial cells: glomerular (inside Bowman’s capsule) and extraglomerular (AKA goormaghtigh cells)
· These are involved in tubuloglomerular feedback to keep the glomerular filtration rate constant
· Macula dense (thick spot on distal tubule which detects changes in sodium concentration)
· Afferent arteriole granular cells (found around afferent arterioles)
Lou sodium in the distal tubule is detected by the macular denser, which then signals to the granular cells using prostaglandins E2/I2, nitric oxide, adenosine/ATP
The granular cells are also regulated by catecholamines (epinephrine), which caused the granular cells to activate (also by stretch)
When they activate, they release renin (hormone/enzyme)
Renin
· The substrate for renin is a circulating plasma protein, angiotensinogen
· It turns angiotensinogen into a smaller, angiotensin 1
o Angiotensin one circulates through the blood and lungs and makes a converting enzyme
o This converts angiotensin 1 into angiotensin 2
· ACE inhibitors (angiotensin converting enzymes) would use blood pressure as angiotensin 2 causes massive vasoconstriction
· As angiotensin two goes through the adrenal cortex, it stimulates the production of aldosterone (steroid hormone)
· Aldosterone stopped sodium secretion
This is called the renin/angiotensin/aldosterone system.
The kidney compensates for low salt levels by reducing fluid volume.
For correcting salt loss: aldosterone stimulates mineralocorticoid receptors in principle cells causing upregulation of sodium ion pump synthesis and activity.
· Excreting more sodium ions out the collecting duct into the bloodstream
Other renal hormones
· Erythropoietin EPO - renal tubular cells - blood oxygenation
o Target is the bone marrow
o Stimulates erythrocyte maturation
Deficient = large amateur red blood cells that don't work effectively
Too much = potential issues with lots more blood cells
· Vitamin D3
o Creates cholecalciferol (from diet/cholesterol and UV)
o In the liver it's hydroxylated to 25-hydroxycholecalciferol
o In the kidney, it creates 1,25-dihyrdroxycholeciferol In the proximal tubule, which is the active form of vitamin D
o Encourages CA2+ uptake for bones (rickets) and teeth
o Vitamin D3 is produced by immune cells:
§ Innate immune response
· stimulates production of the antimicrobial protein cathelicidins
§ Adaptive immune response
· promotes immune tolerance, regulates T cell phenotypes, stimulates B cell proliferation
§ Disease
· enhances the cell mediated response against TB, may protect susceptible individuals against Ms, SLE and type 1 diabetes
Why do we need the kidney?
· Primary excretory organ
· Scrubs 1200ml/min, 1728l/day of blood
· Recovers >99% of all useful solutes
· Regulates salt and water loss
· Regulate body pH (with lungs)
· Acts as an endocrine organ