Week 8: working with emotional triggers
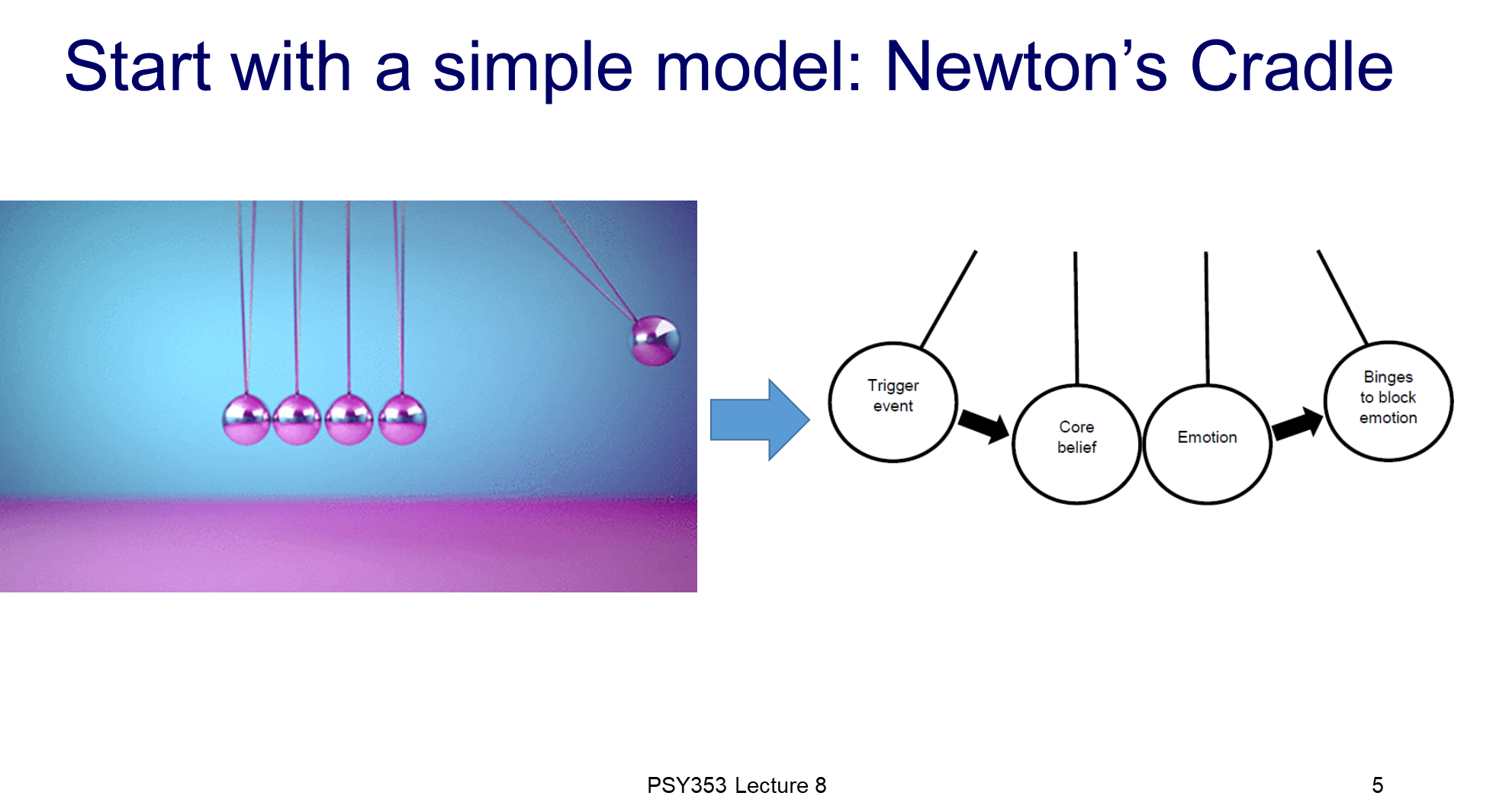
we can use the physics model as a comparison.
this model is an illusion, it gives the perception that the middle balls do not play a role in the movement of the end two balls, however, scientifically they do
it is the same with triggering binges
additionally, the balls on either side once they hit the middle ball results in the other ball going up, it’s a two way street
just how a trigger event and a binge to block emotions are a two way street
Any of these models could apply to anyone, but earlier on it typically is the second model
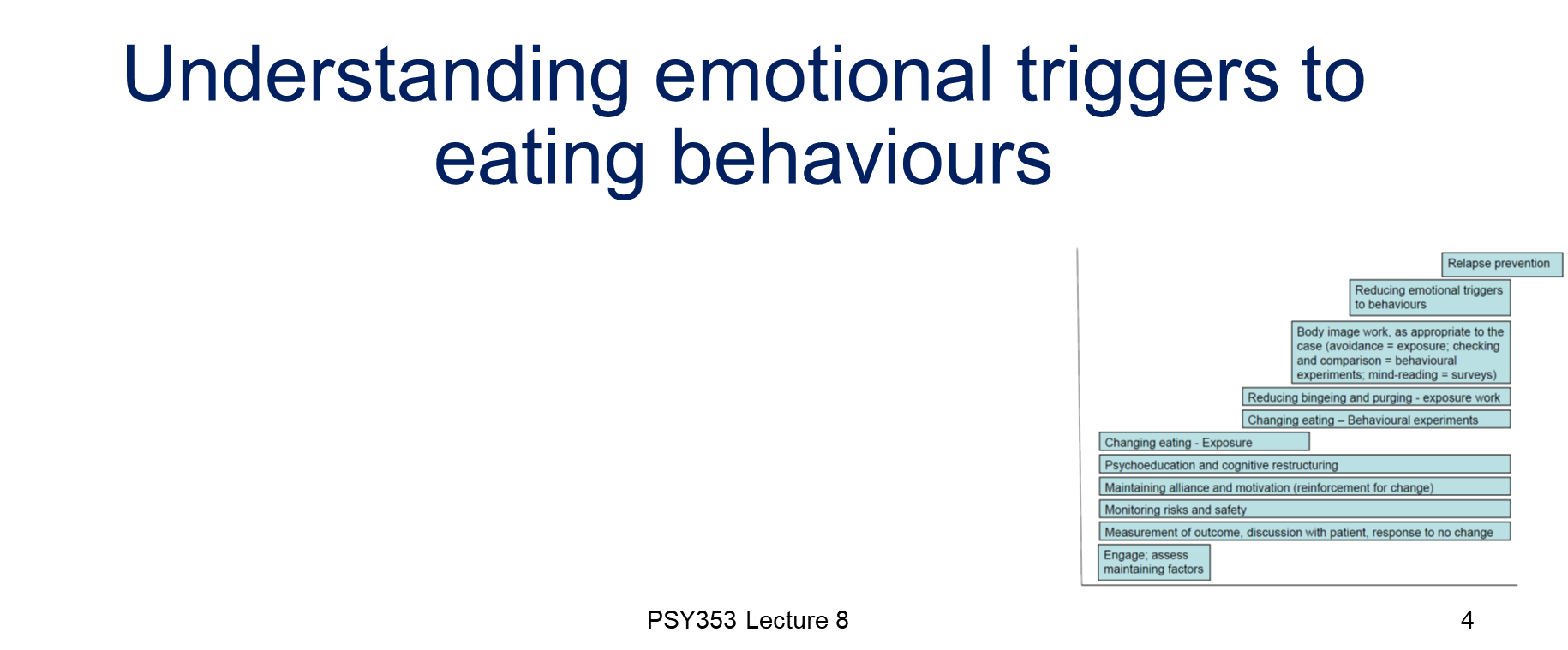
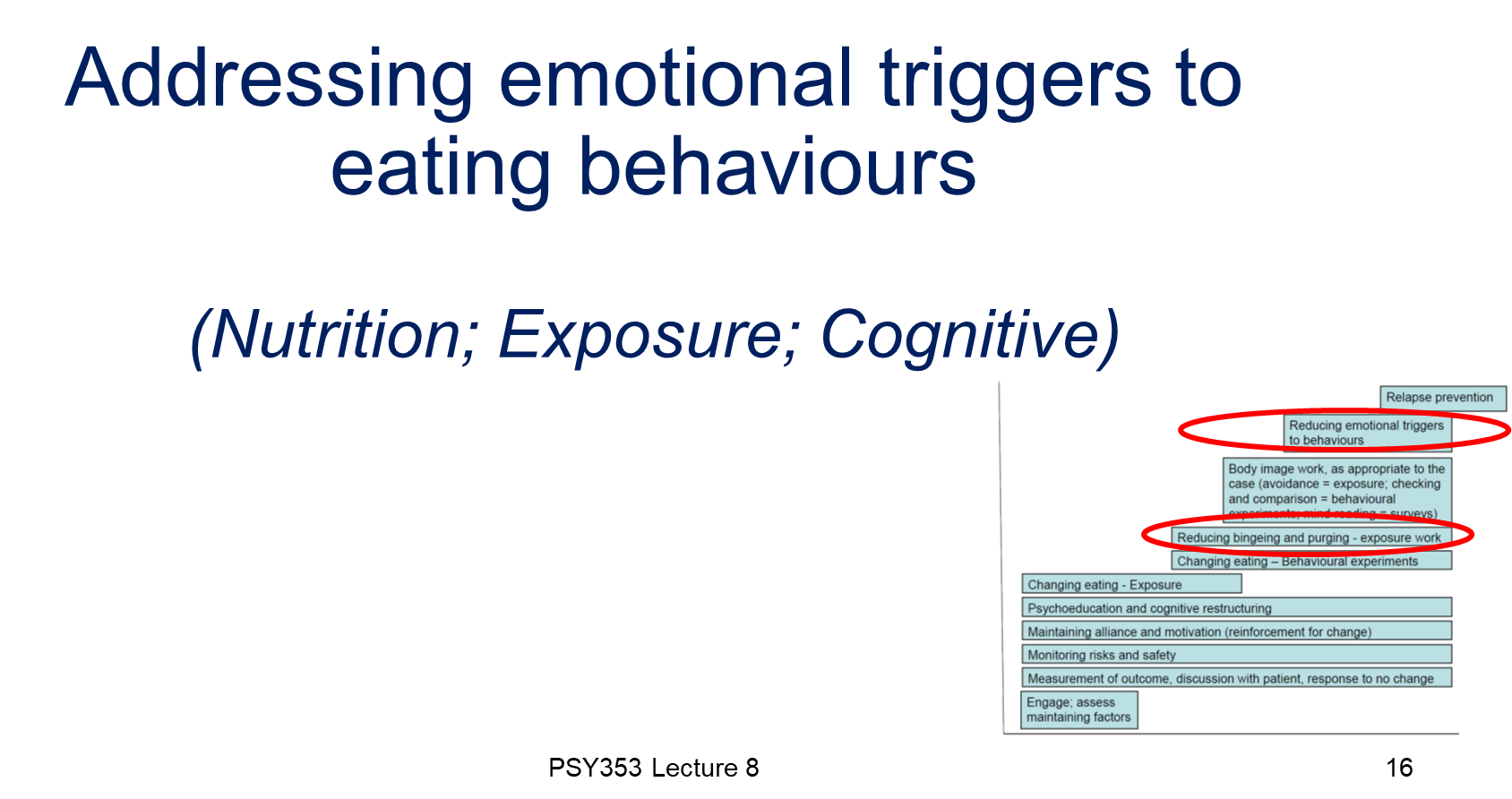
patients want to start with the emotional aspects, however, nutrition MUST come first because patients need to be well nourished to think rationally
anxiety, shame, anger, frustration etc
they find it hard to tolerate being happy, occasionally bingeing can happen because the person feels happy
often people self harm or drink as well as suffer with EDs, food is a controllable thing
avoidance could be restriction, exercise, just to not have to think and avoid the emotion
if I’ve grown up in an emotionally absent environment, do I feel safe with someone that is emotionally open? NO, they feel safer with an emotional pattern they understand, as they’re scared that the nice partner can turn nasty
alexithymia→ people are either incredibly sensitive to emotion or completely numb, you can develop a spectrum of it
Autistic spectrum problem → loads of different manifestations, they can be terrible or great with emotions, just discuss what the patient struggles with regarding emotions and others’ perceptions of their emotional capabilities
these are things we can do biologically
SSRIs prevent the patient’s serotonin levels from decreasing, that is caused due to a lack of carbohydrates
‘SSRO discontinuation syndrome’ described as having electric shocks for the brain, the flu and extreme hangovers all on one, don’t let SSRIs run out for patients, tell them to go straight to the GP
get the biology done way before therapy
have to sit with the emotion instead of the harmful behaviour (like cutting or bingeing), to watch the emotion disappear
relaxation methods like systematic desensitisation to get the patient to cut down their anxiety levels takes so much longer than other methods so isn’t as efficient
may make the therapist feel better but just not as practical