Exam 1
Chapter 33
Blood cells types
Bone marrow:primary site for blood formation and maturation(hematopoiesis)
Stem cell can begin multi lineage differentiation into mature myeloid or lymphoid stem cells
Lymphoid stem cells produce Tor B lymphocytes
Myeloid stem cell differentiate into 3 cell types
Erythrocyte-(RBC)
Leucocytes-(WBC)
Platelets-(thrombocytes)
Erythrocyte(RBC)- They regress after birth until late adolescence. They are gradually replaced by yellow marrow. they are the most abundant of formed elements. Small and biconcave with no nucleus.
Erythrocytes have two principal functions:
(1) to pick up oxygen from the lungs and transport it to systemic tissues
(2) to pick up carbon dioxide from the tissues and deliver it in the lungs.
Erthrocyte that is formed in the bone marrow live 120 days in circulatory system.
Normal range
3.61-5.81 for female
4.21- 5.81 for male
For normal erythrocyte production, the bone marrow also requires iron, vitamin B12, folic acid, vitamin B6 (pyridoxine), protein, and other factors.
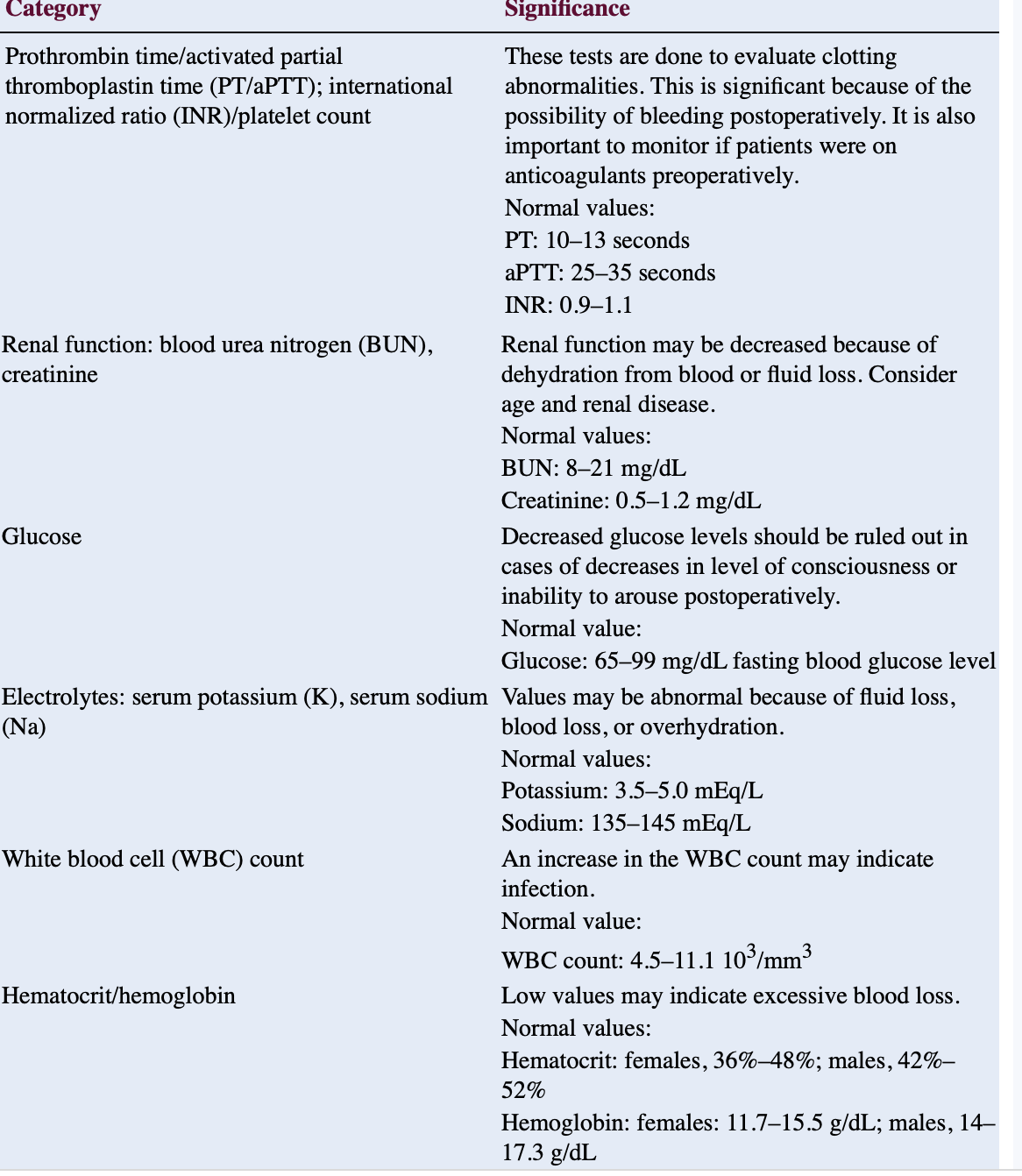
The volume of blood composed of erythrocytes is measured as haematocrit.
Hematocrit
Normal value
36-48 for females
42-52 for males
Hemoglobin
the oxygen-carrying component of an RBC, normal mature RBC contaons thousands of Hgb molecules
Hemoglobin is composed of a pigment (heme) that contains iron (Fe2+) and a protein (globin).
made up of four globins with a heme molecule attached to each globin
Normal value
Female- 11.7- 15.5
Male- 14-17.3
Leukocytes (WBC): components of the body’s defense system against infection and disease. least abundant.
Normal value
4500- 11000
Leukocytes are responsible for the immune responses that protect against harmful microorganisms, including identification and destruction of cancer cells and involvement in the inflammatory response and wound healing.
two types:
granulocytes: neutrophils, eosinophils, and basophils
agranular leukocytes: lymphocytes and monocytes
Clotting cascade: Hemostasis, or blood clotting, is a complex process that stops bleeding
factors and involves
Vasospasm: last more than 1 min, constrict the vessel and reduce blood flow.
Formation of a platelet plug: Von willebrand’s factor
Clot formation: instrisic and extrinsic clotting factor
Clot retraction: approx 30 min platelet trapped within clot begin to contract
fibrinolysis
Clot dissolution: fibronolysis removes clot after tissue has repaired
Hematological assessment
Nutrition: High vit K may increase blood coagulation
diet high in fat and carbohydrate and low in protein, iron and vitamins can decrease the function of all blood cells and ptentially lead to different type of anemia.
Chronic alcohol use is associated with nutritional deficiencies and liver impairment, both of which can decrease the ability of the blood to clot.
Vitamin C- facilitate calcium and nonheme
asparagus, broccoli, sweet and hot peppers, collards. Brussels, sprout, kale, potatoes, spinach, tomatoes, cirtruis fruit, strawberries .
Folacin (folic acid)- help with formation of RBC
Liver, legumes, green leafy vegetable
Vitamin B6- needed for synthesis of hemoglobin
(pyridoxine: meat, poultry, fish, shellfish, green and leafy vegetables, whole grain products, legumes
Vitamin B12-assist in division and maturity of RBCs
meat, poultry, fish, shellfish, eggs, and diary products
Vitamin K- necessary for the formation of prothrombin and other clotting factors in the liver
Cabbage, cauliflower, cereals, dark grean vegetables (broccoli, Brussels, sprouts, asparagus, dark leafy vegetables, fish, liver, beef, egg.
Calcium- bone formation and maintenance
Milk and milk products, fish with bones, green
Cobalt- aid in maturation of red blood cells
organ meat
Cooper- catalyst for H&H
Cereals, nuts, legumes, liver, shellfish, grapes, and meats.
Iron- cellular energy release cytochrome pathway
meats, heart, liver, clams, oysters, lima, bean, spinach, dates, dried nuts, enriched and whole grain cereals, apricots
Past Medical History
hepatitis, cirrhosis, and cancer that alter liver function may result in clotting factor deficiencies.
the synthesis of clotting factors II, VII, IX, and X requires vitamin K
Medication History
Ask pt for current medications, including anticoagulants, aspirin and other salicylates, herbs, nutritional supplements, and nutraceuticals.
Some dietary supplements may interact with prescribed medication therapy.
periodic assessment of periodic assessments of Hct, Hgb level, prothrombin time (PT), International Normalized Ratio (INR), and renal function are recommended when pt is on aspirin
Prolonged antibiotic therapy can lead to coagulopathies, bone marrow depression, or other undesired effects. For example, neutropenia may occur during therapy with penicillins, cephalosporins, or vancomycin.
Physical assessment- Head to toe approach. Be aware and respect patients feelings
Skin, neck assessment : observe for pallor or cyanosis or fissure at the mouth which may indicates nutritional deficiencies and or chronic anemia
A red, swollen, smooth, shiny, and tender tongue (glossitis) may indicate iron deficiency anemia or pernicious anemia.
Respiratory assesment: Four measures of respiration—rate, rhythm, depth, and sound—reflect the body’s metabolic state, diaphragm and chest muscle condition, and airway patency.
Respiratory rates of less than 12 or more than 20 breaths per minute usually are considered abnormal.
Cardiovascular assesment: When blood problems reduce oxygen delivery, the heart works harder to facilitate adequate tissue perfusion
Systolic BP tends to be lower than normal in patients with anemia.
Blood pressure may be higher than normal if the patient has too many RBCs.
Renal assesment: Hematuria is the abnormal presence of gross or microscopic blood in urine.
Musculoskeletal assessment: abdominal or bone pain may occur in pt with hyper or hypoproliferative disorders such as sickle cell anemia, leukemia or infection.
leukemia is a malignant proliferation of white blood cell precurssors or blasts in bone marrow or lymph tissue, which increases the pressure to the bone.
Sickle cell causes RBCs to be sickle shape. The abnormal cells accumulates in the capillaries and smaller blood vessels making the blood more viscous, impairing circulation and cause pain, tissue infarction and swelling.
Abdominal assessment: An enlarged spleen occurs with many hematological problems such as anemia, neutropenia, thrombocytopenia (low platelet count), or polycythemia vera (excessive RBC’s).
Splenomegaly may also occur in conditions such as cirrhosis, hepatitis, mononucleosis, and splenic rupture.
Diagnostic studies
CBC: total number of blood cells (leukocytes, erythrocytes, and platelets)
as well as the Hgb, Hct, and RBC indices (mean corpuscular volume [MCV], mean corpuscular hemoglobin [MCH], and mean corpuscular hemoglobin concentration [MCHC]).
Reticulocyte Count: Larger than RBCs. Reticulocytes are non-nucleated, immature RBCs that remain in the peripheral blood for 24 to 48 hours while maturing.
The reticulocyte count is useful for evaluating anemia, specifically to help distinguish between hypoproliferative and hyperproliferative anemias.
The reticulocyte count may also help assess blood loss, evaluate bone marrow response to anemia, and evaluate treatments for anemia.
Leukocytes Alkaline Phosphates: enzyme produced by normal mature neutrophils
Elevated LAP levels may result from infection, stress, inflammation, pregnancy, steroid use, and leukemia.
An elevated neutrophil count without an accompanying elevation in LAP level is associated with chronic myelogenous leukemia.
Serum Iron (Fe): blood levels should be drawn in the morning because of a diurnal variation in serum iron, with lower evening values. A pt on iron supplement should be asked to avoid the iron supplement for at least 24hr before the test is taken.
Ferritin; protein stored in the body.
Low ferritin levels may indicate iron deficiency, chronic GI bleeding, or heavy menstrual bleeding.
High levels may indicate alcoholic liver disease, hemochromatosis (excessive iron absorption), hemolytic anemia, Hodgkin’s lymphoma, or megaloblastic anemia. Illnesses such as infections, inflammations, and malignant diseases cause increased levels
Prothrombin time(PT): the purpose of this testevaluate the extrinsic coagulation system (factors V, VII, and X, and prothrombin and fibrinogen)
Used to monitor response to oral anticoagulant therapy.
A prolonged PT may indicate deficiencies in fibrinogen; prothrombin; factors V, VII, or Xl; or vitamin K.
It may also result as a therapeutic response from ongoing oral anticoagulant therapy (warfarin, Coumadin; tinzaparin sodium, Innohep).
A prolonged PT that exceeds two and one-half times the control value usually indicates abnormal bleeding.
International normalized ratio (INR): measure PT (prothrombin time) and to evaluate the effectiveness of oral anticoagulant therapy (warfarin sodium, Coumadin).
Pt on warfarin INR is 2-3
Pt on warfarin with prosthetic heart 2.5-3.5
increased INR indicates disseminated intravascular coagulation (DIC), cirrhosis, hepatitis, vitamin K deficiency, salicylate intoxication, uncontrolled oral anticoagulation, or massive blood transfusion.
Partial Thromboplastin Time: screen for deficiencies of the clotting factors in the intrinsic pathways and to monitor response to thrombin inhibitor therapy (heparin, argatroban).
range of the PTT is 60 to 70 seconds
aPTT is 30 to 40 seconds
Platelet Aggregation: performed in patients who are suspected of having abnormal platelet function, i.e., those who have a prolonged bleeding time and a normal or near-normal platelet count.
aggregation can be impaired with von Willebrand’s disease and use of certain medication such as aspirin, NSAIDs, antineoplastics, and psychotropic agents.
Bone marrow aspiration and biopsy: bone marrow aspiration and biopsy is to diagnose thrombocytopenia, leukemias, granulomas, anemias, and primary and metastatic tumors.
performed to determine causes of infection, to help stage diseases such as Hodgkin’s disease, to evaluate chemotherapy, and to monitor myelosuppression
involve the collection of a soft tissue specimen from the medullary canals of the long bone and interstices of cancellous bone for histological and hematological examination.
CHAPTER 34
Anemia: is a deficiency in the number of RBCs, occurs when there is a reduction in the oxygen-carrying capacity through either fewer RBCs or a reduction in hemoglobin.
Clinical manifestation:
mild can be asymptomatic; fatigue, pallor, dyspnea, heart palpitation, tachycardia, brittle nail, spon shaped nails(Koilonychias), glossitis, menstrual irregularities, delayed healing, syncope.
Causes of anemia
dietary
chronic blood loss hemorrhage, heavy menstruation, type of cancer esophageal, colon, stomach- peptic ulcer disease.
malabsorption of iron, b-12, celiac disease, Crohns disease
Use of H2 inhibitors, Proton pump inhibitor, and antacid
liver disease effecting iron absorption, and storage.
GI surgeries ; gastric bypass; partial and total gastrectomy
Commodities induced anemia: CHF, CKD for older adults
Classification
Morphologic: classified by RBC size and color
Etiologic: clinical condition caused the anemia
Iron Deficiency Anemia- in the world it’s high in non Caucasian American of lower socioeconomic esp. infants, children and pregnant women.
In the U.S its high in african american and mexican american women.
higher in female than male esp. premenopausal women due to blood loss through menses.
Iron-deficiency anemia can result in a condition known as pica, causing the iron-depleted individual to ingest nonnutritive substances such as paint, dirt, clay, ice, or laundry starch.
Iron-deficiency anemia often occurs as a result of hemorrhage and chronic blood loss, for example, heavy menstrual bleeding, certain types of cancer (esophageal, colon, stomach), and ulcerative gastrointestinal problems such as peptic ulcer disease.
Poor absorption of iron may be due to celiac disease, Crohn’s disease, and the chronic use of medications such as H2 inhibitors, proton-pump inhibitors, antacids, aspirin, and NSAIDs.
Gastrointestinal surgeries such as gastric bypass surgery and partial and total gastrectomy can lead to poor absorption of iron and iron deficiency anemia.
Older adults with multiple comorbidities, anemia is frequently a cause for hospitalization and exacerbates many chronic conditions, such as congestive heart failure (CHF) and chronic kidney disease
With an iron deficiency, the body has insufficient hemoglobin to carry adequate oxygen to meet body requirements.
The body is able to store iron in the liver as ferritin, and it is transferred to the rest of the body in times of increased demand via the protein transferrin, manufactured in the liver.
Iron deficiency anemia occurs when the body has exhaust the iron store so release of cytokine is released as a result of acute loss or inflammation in a diminished response from the kidneys for production of erythropoietin
stages of IDA as a result of negative iron balnce include: iron depletion, deficient erythropoiesis and finally IDA.
Anemia is the late stage of iron deficiency.
Signs and symptoms:-
Hypoxia
Fatigue and pallor
onset of tachycardia and tachypnea
SOB
fissure in the mouth or glossitis
painful swelling of the tongue- smooth and shiny.
Koilonychia
blood loss
decreased H&H
decreased serum ferritin
change in LOC
Diagnostic tests
CBC
decrease H&H
low serum ferritin. less than or equal to 100ug/L - 100% of IDA
serum iron
Total iron binding capacity(TIBC)
Serum transferrin receptors
mean corpuscular volume (MCV)
Treatments
Diet- red meat, dark green keafy vegetables(spinach, broccoli, peas), beats, dried beans, iron fortified breakfast cereals and breads, cream of wheat.
Vitamin C such as citrus fruits(orange, grapefruits) increases the absorption of iron.
Oral supplement is the first line of treatment if diet is not enough, but IV and IM is available.
monitor pt for abd discomfort, constipation, and or diahea, and
nausea.
parenteral means is indicated only in cases of severe gastrointestinal distress secondary to oral administration, malabsorption disorders, or in acute cases of IDA in which levels need to be increased more rapidly.
Nursing Management
IDA are related to the decreased oxygenation of body tissues.
Teach pt on diet and food that help maximize its absorption
pt on long life use of iron should be monitored for liver problem r/t to iron storage.
Monitor pt VS
Monitor labs for low ferritin and low H&H
minimize pt means of blood loss
Vitamin B-12 (Cobalamin) Anemia
Cellular metabolism is dependent on vitamin B12 because it is essential to the synthesis of fatty acids and energy production.
Vitamin B12 (also known as extrinsic factor) is introduced to the body through dietary sources of animal proteins, including meat, seafood, eggs, and dairy products.
The parietal cells of the stomach lining secrete a protein-binding substance known as intrinsic factor that binds with vitamin B12, leading to absorption in the ileum of the small intestine.
Pernicious anemia is caused by lack of intrisic factor
pernicious anemia is an autoimmune disease that leads to a vitamin B12 deficiency because of the inability to absorb vitamin B12 without intrinsic factor.
Vitamin B12 is also required for the conversion of methylmalonyl coenzyme A, part of the Krebs cycle.
Vitamin B12 and folate are cofactors essential in DNA synthesis and the methylation cycles of RBCs, part of cellular metabolism.
Supplementation of synthetic folic acid escapes this methylfolate trap, masking the vitamin B12 deficiency, and therefore resolves the anemia but has no effect on the neurological symptoms produced by the deficit of vitamin B12.
Nitrous oxide administered to a patient with a vitamin B12 deficiency interferes with the methylation cycle by destroying methylcobalamin, the form of vitamin B12 in human plasma.
This leads to impaired RBC production, and a profound postoperative anemia results and can be fatal if the vitamin B12 deficiency is not discovered.
Vitamin B12–deficiency anemia is reversible
Signs/ symptoms:
Can cause nerological and psychaiatric dysfunctions
Dymelination
spinal cord degeneration
peripheral neurophathy- paresthesia, numbness and tingling in the hands and feets.
altered mental status- depression
visual disturbance inability to distinguish blue from yellow, or blindness
tachycardia and tachypnea
SOB
dizziness and fatigue
Lhermitte sign-electric shock sensation produced by neck flexion- rare
Depression
mood swigs
impaired test and stinging sensation on the tongue
impaired sense of balance- dark
dementia resembling alzheimers
Constipation and diarrhea
anorexia
menstral irregularitied
weight loss
glossitis
low grade fever
tinnitus
Diagnosis
Delayed clinical manifestations, the results of a CBC may be the first indication that a problem exists.
The diagnosis of vitamin B12 deficiency is made based on a history and physical examination and a vitamin B12 serum assay blood test- as its limitations and has a wide normal range (200 to 1,000 pg/mL)- Patients with liver disease, lymphoma, and myeloproliferative disorders may have false-negative results.
A more sensitive test for vitamin B12 deficiency is to measure the level of methylmalonic acid (MMA), in the patient’s urine or blood. An excess of MMA indicates a lack of vitamin B12 in the tissues.-Patients with renal failure, dehydration, or hypovolemia can have falsely elevated serum MMA levels, a urinary MMA test is needed for accurate diagnosis in individuals with these disorders
In Vit B12 deficiency, the serum MMA level is more sensitive and is elevated, whereas the homocysteine level remains normal.
Gastrin levels, intrinsic factor levels, and in rare instances, the Schilling’s test, a radionuclide 24-hour urine test that indirectly measures intrinsic factor.
Treatment
Animal proteins provide the only source of vitamin B12 in the world.
Dietary sources of vitamin B12 include meat, seafood, eggs, and dairy products.
Long-term vegans/vegetarians or those of low socioeconomic status are at increased risk of deficiency and may need to take a daily supplement of vitamin B12.
vitamin B12 may not be sufficient once the deficiency is profound and the patient has developed clinical manifestations such as fatigue, weakness, and paresthesias. Once severe deficiency is determined, weekly vitamin B12 injections are required.
Nursing management
Educate patient that deficiency causes orthostatic hypotension so they should get up slowly.
Educate patient on clinical manifestation
Educate patient that pregnancy, hypothyroidism, advanced stages of cancer and intestinal tapeworm may increase the need for B12.
Educate chemo patient that radiation of certain cancer may cause inflammation of the intrstines that interferes with the b12 absorption, so there is a need for replacement therapy of B12.
Before starting a patient on folic acid, confirm that the patient does not have a vitamin B12 deficiency. Folic acid resolves the anemia by escaping the methylfolate trap, but neurological degeneration due to vitamin B12 deficiency continues.
Monitor use of nitrous oxide; Nitrous oxide inactivates vitamin B12 in the body. Prior to using for anesthesia, confirm that the patient is not vitamin B12 deficient.
Folic Acid Deficiency
Folic acid water-soluble vitamin (B9)- but folic acid is the synthetic form.
Folic acid, along with vitamin B12, is necessary for a complex pathway that aids in DNA synthesis and the formation of heme, the iron-containing portion of the hemoglobin molecule- essential for cell maturation and replication.
Folic acid deficiency is usually a result of inadequate dietary intake.
Frequently affects older adults, those with chronic illness, individuals who abuse alcohol, and individuals who go on extreme diets lacking folate.
Deficits in folic acid also develop secondary to malnutrition, specific malignancies, Crohn’s disease, celiac disease, and malabsorption due to gastrointestinal surgeries or medications.
Patients with rheumatoid arthritis who are treated with methotrexate may develop folic acid deficiency secondary to the antagonistic effects of this medication to folic acid.
Dietary sources of folate include green leafy vegetables, bran, yeast, legumes, and nuts. Fortified ceral and certain grain such as wheat flour.
Folic acid deficiency during pregnancy is also linked to fetal neural tube defects and some congenital orofacial abnormalities
It is recommended that pregnant women take folic acid supplementation of at least 400 mcg daily because this has led to decreased incidence and severity of spina bifida, cleft palate and lip, and other neural tube defects.
Folate enters the body through dietary sources or as folic acid supplementation and is absorbed in the jejunum portion of the small intestine
It is not unusual for deficits to occur in the presence of any problem affecting the jejunum, such as in gastric bypass surgery or the Whipple procedure (pancreatic duodenectomy); surgical procedure for specific gastrointestinal cancers.
Medications such as oral contraceptives, metformin for type 2 diabetes mellitus, and chemotherapeutic agents (fluorouracil) may interfere with folic acid absorption
Folic acid supplementation may increase the hepatic metabolism of the anticonvulsant phenytoin (Dilantin), which may increase the incidence of seizure activity.- correct the folic acid before initiating pheytoin to decrease seizure activity.
Chronic alcohol use contributes to folic acid deficiency secondary to malnutrition that is frequently present in these patients; alchohol affects the absorption of folic acid.
RBC of a pt with chronic alcohol use shows abnormal morphology and half life span of 120 days.
Signs and symptoms
Pallor
Tachycardia and tacypnea
dizziness
fatigue
pantocytopenia
decrease platelet and risk for bleeding
The neurological manifestations of vitamin B12 deficiency do not occur with folic acid deficiency but will persist if vitamin B12 is not replaced.
pt should avoid excessive cold and heat due to fatigue
Pt with B12 and folic acid can have
mood disorder
memory difficulty and weakness
vitiligo
premature graying of the hair
glossitis often seen with b12 deficiency
Because the folate/vitamin B12 codependency affects RBC maturation, folic acid replacement may reverse the anemia, but the neurological degeneration that occurs in vitamin B12 deficiencies continues and may become irreversible.
Diagnostic test
CBC- serum folate levels may or may not decrease
serum should be fassting blood test or level will be falsely elevated
RBC folate level-reflects the serum folate level over the past 3 months
Serum MMA and homocysteine levels are the best laboratory tests used to differentiate between anemia caused by a folic acid deficiency and those secondary to a vitamin B12 deficiency.
Since folate and B12 are cofactor of methylation cycle- Kreb cycle;
In folic acid deficiency the homocysteine levels are elevated and the MMA remain normal.
Renal insufficiency affects the result.
Treatment
Diet- fortified cereal and grain, dark greeny vegetable, dried beans and legumes, nuts bran and yeast
oral supplement is recommended for pregnant women(400mcg), children in their first life, pt with bypass surgey
Nursing management
diet management; food high in folic acid
encourage 400mcg for pregnant women to avoid tube defect
Encorage folic acid for pt with GI resection such as bypass and whipple procedure.
Sickle cell Anemia
is a genetic mutation that must be present in both parents in order for this form of the disease to manifest in offspring.
Affect predominately african descendant
In SCD, the RBC goes through a morphological change when it is exposed to decreased oxygen tension- elongated and stiff and lose flexibility
Sickle-shaped RBCs carry less oxygen and are fragile. Because of the decreased flexibility and fragility, RBCs break apart (hemolysis) as they pass through the capillary beds. The result is congestion and clumping in the capillary beds and the formation of thrombi
Individual with SCD RBC last 15-20 days
Destruction of RBCs also releases bilirubin, causing a rise in the serum bilirubin level.
Possible congestion in the spleen due to the increased RBC fragments that must be phagocytized leads to an enlarged spleen and possible pain.
Patient with SCD are increased risk of infection esp respiratory infection caused by pneumococcus, pertussis and Haemophilus influenzae.
When the sickling process is rapid and severe, the patient has a sickle cell crisis.
4 types of crisis
Vasooclussive or painful crisis- most common obstruction of vessels by hemolyzed cells
aplastic crisis- bone marrow ceases to produce RBCs due to decrease in blood reticulocyte count
sequentration crisis- massive pooling of RBCs in the spleen leads to hypovolemic shock and CAF.
hemolytic crisis results from increase rate of RBC hemolysis- decrease hemoglobin and increase jaundice.
Precipating factors- anything that causes hypoxemia
increase vasoconstriction and sicklinfg of RBCs
dehydration
cold temperation
infection
environment with low oxytgen tension- depressurized airplane cabins and high mountains
Crisis tend to lasts days to weeks
Repeated episodes of crises and infarctions of the bones can lead to uneven development of the fingers and toes, known as hand-foot syndrome- causing pain.
Pregnancy, with its increased demand on the body, can be a cause for the exacerbation of SCD.
Death is usually the result of CVA, infection, or long-term organ system damage.
Signs and symptoms
Fatigue
pallor
SOB
vaso-occlusion of blood vessel- pain and swelling
tissue ischemia causes cerebrovascular, pulmonary and splenic infarctions
Pain occurs in the joints, bone, chest and abdomen
Priapism in males
kidney and liver damage
delayed wound healing esp in the extremities due to impaired circulation and venous stasis
Treatment
no cure
treatment is aimed to prevent the crisis and symptom management
long term managementis to prevent organ failure
During a crisis, oxygen therapy is implemented to reverse the hypoxia caused by decreased hemoglobin and vaso-occlusion of vessels.
Aggressive hydration with oral and parenteral fluids increases blood volume and reduces renal vaso-occlusion caused by increased hemolysis of RBCs.
Analgesia, usually from opiates, is administered for severe pain
Abx is initiated for infection.
Hydroxyurea- chemotherapeutic agent
causes mylosupression- decrease ability of the bone marrow producing any type of blood type
teratogenic
Blood transfusions- not a singulair treatment. Its given with Iron-chelating agents such as desferrioxamine may need to be simultaneously administered parenterally with transfusions to bind to the iron and decrease the morbidity of iron overload.
Patients receiving repeated exchange transfusions have an increased risk of blood transfusion reactions and iron overload.
High levels of iron in the liver result in fibrosis and cirrhosis, leading to hepatomegaly and, ultimately, liver failure.
Peripheral stem cell transplantation is being attempted with a human leukocyte antigen (HLA)-matched sibling- one without the sickle cell trait us the preferred donor; otherwise the best match available
Transplantation has a high mortality rate with incidence of Graft vs host disease- occurs when donor bone marrow or stem cells attack the recipient’s tissues and occurs if the T cells in the graft.
Preventive measures such as prophylactic use of penicillin to prevent pneumococcal infection, vaccinations, and maintaining adequate hydration are first-line measures to decrease the incidence of crises.
Emotional support for the patient and his or her family is essential in order for the patient to be able to cope with SCD.
Nursing magement
Multiple episodes of crises and infarctions over a period of several years can result in the developmental problems seen in individuals with SCD:
Hand-foot syndrome
Delayed puberty with developmental delay of secondary sexual characteristics
Cognitive impairment, ranging from learning disabilities to mental retardation
Psychosocial issues
Monitor pt for tacycardia and tachypnea
monitor pt for jaundice since there is a decreased life span of RBCs in people with SCD and the increased destruction of those RBCs may cause an increase in serum bilirubin, leading to jaundice.
Administer 02 to assist decrease hypoxia
Encourage fluid to increase blood volume
Administer pain med
Administer antipyretic
provide support measure for pt and family and possible need for counseling.
update of immunization and annual flu with pneumococcal vaccine is essential with dental hygiene and checkup to avoid infection
avoid overexertion
avoid dehydration, increase fluid intake
risk for more sickle cell criciss during pregnancy - therapy and couseling recommended
Genetic counseling
Fetal complication- low birth weight, gestational HTN, preterm labor, spontaneous abortions, stillbirth.
Aplastic anemia(hypoplastic anemia)
is a rare disease process that develops due to bone marrow depression or damage
often acquired secondary to infections, including hepatitis and human immunodeficiency virus.
associated with treatments using high-dose radiation or chemotherapy for cancer, exposure to toxic chemicals, administration of specific medications (chloramphenicol and gold compounds), and autoimmune disorders.
Usually secondary to inherited marrow dysfunction; a second peak in people between the ages of 20 and 25; and an increased incidence in people older than 60 years of age
male to female ratio is 1:1.
The damage to the bone marrow, whether secondary to chemicals or medications or an autoimmune response, results in decreased production of red blood cells, white blood cells, and platelets- Pantocytopenia.
Signs and Symptoms- insidious and chronic
Decrease RBC
fatigue
pallor
SOB
tarcardia
pallor
dizziness and head.
Decresed WBCs
increase supceptibilty to infection
may lead to thrombocytopenia causing pt to have unexplained bruising, nosebleeding, gum bleeding and prolonged cut and other injuries
Diagnosis
CBC- pantocytopenia, decreased reticulocyte, WBC, and platelet counts
coagulation test- risk for thrombocytopenia
iron levels
hemoglobin electrophoresis- evaluates the anemia- identify different forms of hgb. increased Hgb F
bone marrow biopsy- lack of hematopoietic cells with predominate of fat cells
Treatment
During evaluation phase of aplastic anemia- treated with blood transfusions, and repeated transfusions may lead to increased iron levels.
The preferred treatment for aplastic anemia is bone marrow transplantation from an HLA-matched sibling donor.
Other treatments focus on stimulating bone marrow with medications such as filgrastim (Neupogen®) and epoetin-alfa (Epogen®), which stimulate the bone marrow production of cells and relieve symptoms.
In pt over 60 yr, immunosuppressive therapy is preferred.
patients who undergo bone marrow transplantation, there is an increased risk of GVHD.
Nursing management
Provide supplemental O2
Administer blood product
implement bleeding precaution
protect pt from injury
Avoid exposure to infection; croded places, and infection
monitor pt temp
its a medical emergeny intruct pt and family to contact PCP for signs of anemia, infection and bleeding.
Thrombocytopenia
Reduced number of platelets below the average range of 150,000 to 450,000/mm3.
complication of other disorders or a syndrome as a result of other events occurring in the body.
Antibodies that increase platelet destruction may be genetic, acquired, or medication induced.
medication- sulfa
autoimmune condition- lupus and DIC(acute or chronic)
viral infection in children and pregnant women(final trimester)
In approximately 70% of the cases of idiopathic thrombocytopenic purpura (ITP), there is an antecedent viral disease that precedes the eruption of petechiae or purpura by 1 to 3 week
Risk for hemorrhage in pt with HIT, DIC, ITP
it appears to be an immune system dysfunction in which antiplatelet antibodies are formed, which increases platelet destruction. Rather than the 7- to 10-day life span, the platelets may be destroyed in a matter of hours.
It typically occurs 5 to 14 days after the first administration of heparin.
Signs and symptoms
decrease number of platelets- easy bruising and petechiae.
Bleeding may occur from the nose, around the gums, or from the gastrointestinal tract.
In severe cases, bleeding in vital organs such as the brain may prove fatal.
Chapter 17
Post op phases
Phase I
This phase is generally in the PACU or intensive care unit (ICU)
There is intensive, close monitoring of all vital signs with continuous electrocardiogram monitoring.
There is a focus on cardiac, respiratory, and neurological functions, surgical-site monitoring, and pain and temperature control.
The goals of care in this phase are to stabilize the patient’s vital signs, allow the patient to awaken from anesthesia, and achieve adequate pain control.
Phase II
less intensive
The focus of nursing care is on preparing the patient to be discharged to an extended-care environment or home.
Phase III
focuses on providing ongoing care for those patients remaining in the postoperative care area after discharge criteria has been met.
Home D/c criteria
pt awake and alert
V/s stable
tolerating fluid no N/v
comfortable with oral pain meds & non pharmalogical methods
Pt is stable and able to walk
Pt is able to void, if pt cant void sign off to been no risk by provider
No sign of bleeding
skin intact; surgical wound clean and dry
no adverse reaction
pt understands teaching, and interpreter is available.
Post management
assess and monitor pt response to anesthesia
timely intervention to resolve problem
evaluate intervention; effects or adverse effects
reassess pt condition
evaluate achievement of D/c criteria
Post op assessment
Airway patency
• Respiratory status, including oxygen saturation (and capnography, if indicated) and auscultation of lung sounds
• Vital signs:
• Blood pressure
• Pulse: apical and peripheral
• Cardiac monitor rhythm
• Hemodynamic pressure readings if indicated
• Temperature
pain and comfort level
• Neurological function, including level of consciousness, motor function, and sensation
• Temperature and color of skin
• Condition of dressings; assessing for bleeding or drainage
• Condition of visible incisions
• Presence and patency of IV catheters, drains, and other catheters
• Hydration status and fluid therapy
Common labs in the PACU
patient-controlled analgesia (PCA)
A PCA pump is an infusion of a prescribed amount of analgesia through an IV route when the patient pushes a button.
only the patient can push Botton
Postoperative Nausea and Vomiting (PONV)
In the immediate postoperative period, PONV can cause dehydration, electrolyte imbalance, wound dehiscence, and aspiration.
Risk factor include
young, nonsmoking female
Have a history of PONV or motion sickness.
Certain types of surgeries; such as cholecystectomies and laparoscopic, intra-abdominal, gynecological, and neurological surgeries.
General anesthesia causes more PONV than regional anesthesia.
The longer the patient is under general anesthesia the more likely to experience POV
neuromuscular blocking agent such as neostigmine can cause PONV.
Treatment
minimize opiod usage
hydration should be minimized
Prophylactic treatment by using a combination of antiemetic medications in high-risk patients before surgery can help reduce PONV.
Dehiscence/evisceration
Dehiscence/evisceration requires immediate notification and intervention by the surgeon; maintain low Fowler’s position, minimize movement, and cover wound with sterile saline dressing.
Chap 5- Pallative care
Pallative care: is a specialized form of care that focuses on relief of pain and other symptoms and stress associated with a severe illness.
concurrently with curative treatment that meets the patient’s goal
Palliative care is provided in hospital, outpatient, and community settings.
It is also provided for patients under hospice care with a projected prognosis of 6 months or less.
Palliative care provides continuity of care across healthcare settings, including the outpatient clinic, hospital, rehabilitation or nursing facility, home, and hospice.
Hospice care:focuses on the care of a patient with a terminal illness who has less than 6 months to live
Domains of Pallative care
Domain 1: Structure and Process of Care- addresses the plan of care provided by nurses and providers with advanced PC training. The plan should incorporate the patient’s goals, preferences, and values while recognizing that they may change over time. The plan of care should travel with the patient across healthcare settings. Patients and families should be educated about hospice care when death may occur within the year
Domain 2:Physical Aspects of Care-assess, treat, and document symptoms such as pain, dyspnea, constipation, and nausea using standardized scales to evaluate the effectiveness of the interventions. Patient outcomes should be documented.
Domain 3: Psychological and Psychiatric Aspects of Care- state that the PC plan should assess and document the presence of anxiety, depression, and delirium using available standardized scales such as the Memorial Symptom Assessment Scale and the Edmonton Symptom Assessment Scale.
Domain 4: Social Aspects of Care, Including Advanced Care Planning-Nurses are important in advanced care planning (ACP), a process in which patients, with support from care providers, family, and important others, make decisions about future healthcare. The concept of ACP is based on the premise that persons with life-threatening chronic diseases or polymorbidity and their families need to be assisted by healthcare professionals to identify and determine preferences and wishes about end of life and respective decision making.
Domain 5: Spiritual, Religious, and Existential Aspects of Care- Spiritual care is based on the patient’s preferences.
Domain 6: Cultural Aspects of Care- Cultural humility may be an especially effective framework for navigating highly sensitive and emotionally charged discussions and interactions surrounding palliative care or end-of-life decisions. Awareness of power imbalances and an inclusive and open approach to incorporating a variety of perspectives and practices are important components of provider training, communication, and practice, promoting mutual empowerment, respect, partnership, and optimal care outcomes.
How healthcare decisions are made
• Preferences for how and to whom information is disclosed
• Dietary preferences
• Family communication
• Perspectives on death, suffering, and grieving
• Funeral/burial preferences
Domain 7: Care of the Imminently Dying- educate family about signs and symptoms of dying
Domain 8: -Ethical and Legal Aspects of Care:This domain also addresses the nurse’s role as patient advocate, assuring the patient or surrogate that preferences are known and will be honored and that ethical care will be provided. This includes the patient’s right to full disclosure of information and refusal of treatment. The ethical principle of beneficence is demonstrated by providing care that benefits the patient, such as good symptom management. Addressing the patient’s spiritual distress and respecting wishes for the use of life-sustaining treatment are examples of nonmaleficence, or not doing harm to the patient. Providing equitable access to hospice and PC for all patients is an example of the principle of justice.
Changes prior to death
Early stage(death approaching): Pt withdraw, loss of interest in soc contacts. Body slow; anorexia but no experience of hunger and thirst, begins to sleep more
Middle stage- weeks before death; decline in mental status; confusion, disoriented, sleep most of the time. Decrease Bp, and temp, irregular RR- labored and rapid, skin colr begins to change. Speaking slows or cease.
Late stage; days or hours before death- brief surge of energy, symptoms worsen as coma ensues, extremityies are cool and mottled, RR; rapid and labored (cheyne stokes), loss ability to manage secretion due to loss of swalllow reflex. Congestion in the airway causing RR to sound loud and wet. Death follows.
Hearing is the last ssense to lapse before death.
Symptom Management
Opiates, such as morphine, and adjuvant medications are often the treatment of choice for pain.
Anticholinergic medications help dry the secretions, lessening the gurgle.
Delirium can be managed by calm verbal reassurance. Surrounding the patient with familiar sights, sounds, and smells is also beneficial. Haloperidol or benzodiazepines (lorazepam, midazolam) can be used to manage hyperactive delirium in dying patient.
Family support
allow family the opportunity to participate in pt’s care such as mouth care, bathing, massaging the aching joint, reading to pt
use of reflective listening help family process their experience.
Asses family understanding of pt diagnosis and dying
infor them that pt is dying, and open dpace for them to grief.
bring in pt favourite music, quit, family pictures.
ask the young children who cannpt visit to write notes to share with the pt and alternate it with calls. Ask them to record stories about the past and share with pt
Principle of Double effect
The principle of double effect, often invoked concerning the effect of opiates at the end of life, implies that an intended good effect such as pain management is ethically permissible even if it produces an unintended secondary effect, hastening death
Postmortem care: involves preparing the body for eventual disposition to the funeral home. The body should be treated with respect, incorporating the family’s religious and cultural practices. Practices vary by state and/or local jurisdiction, but if there is to be an autopsy, tubes and catheters usually must remain in place. If no autopsy is planned, remove tubes and cleanse soiled areas of the body
Decisional Capacity
Pt is deemed to have decisional capacity if the
have the ability to understand the nature and consequence of the proposed treatment
have the ability to rationally evaluate the burdens, benefits, and risk for treatment
have the ability to communicate a decision
Well managed death
Appropriate pain and symptom management
Avoiding a prolonged dying process
Clear communication about decisions by patient, family, and provider
Adequate preparation for death for both the patient and loved ones
Feeling a sense of control
Finding a spiritual or emotional sense of completion
Affirming the patient as a unique and worthy person
Strengthening relationships with loved ones
Not being alone
Moral distress: involves the inability to do the morally correct thing because of situational factors
High stress in the work environment.
time and resource pressures
high-technology care situations
differences in values attitudes,
cultural or religious beliefs among patients, families, and staff.
Nurses cope with moral distress by talking with other nurses about the situation and sharing their feelings and values with their peers. They also share with and receive support from nurse managers and chaplains.
Nurses Self care
As individuals, nurses can build self-care activities into their daily schedules. Talking with trusted friends or nursing colleagues, journaling, engaging in aerobic exercise, gardening, practicing yoga, meditating, and praying can help recharge emotional batteries.
Performing postmortem care together
Pausing for a moment of silence during the monthly staff meeting to remember those who have died in care
Sending the family a bereavement card
Hospice Care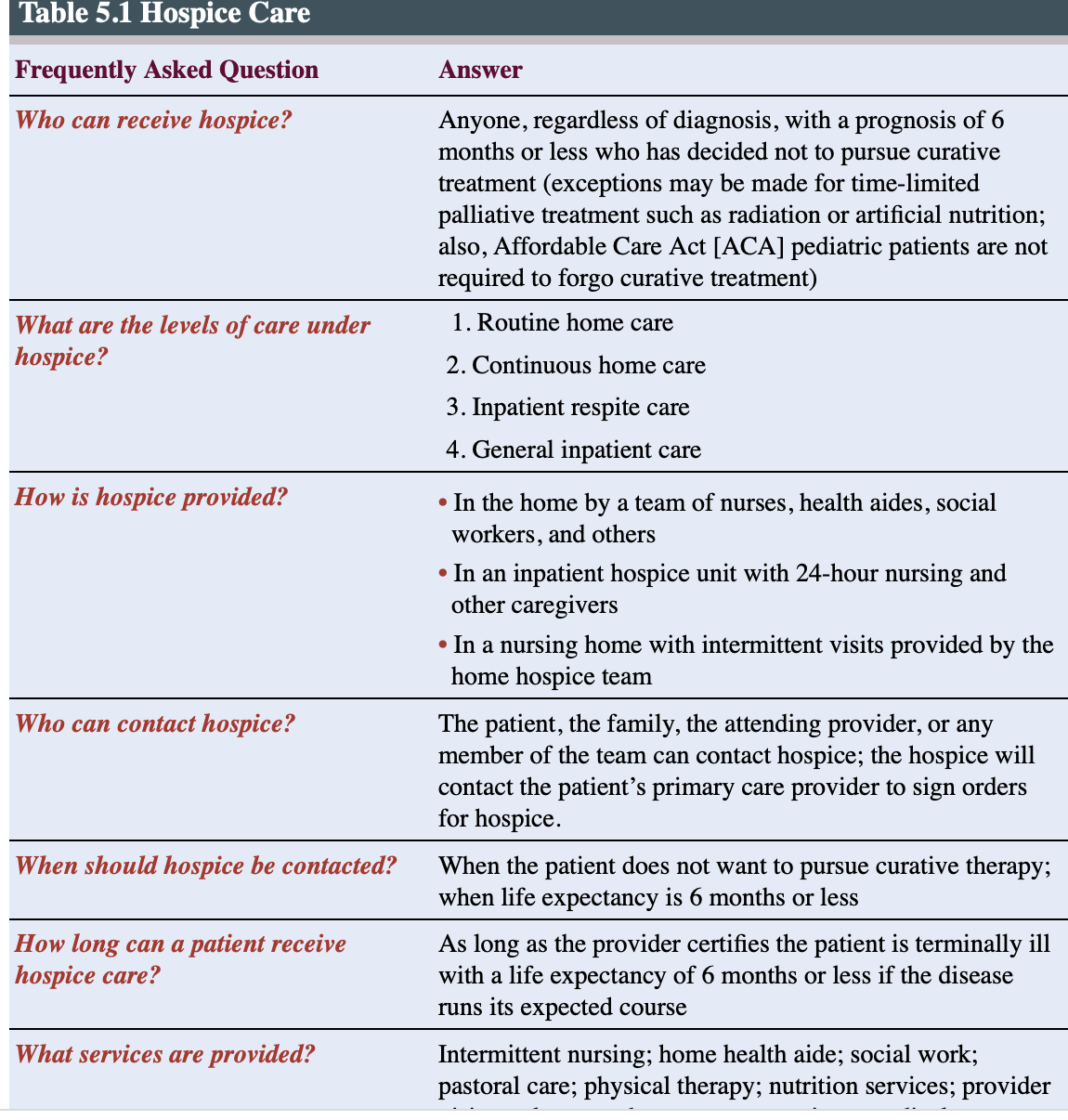
Chapter 10
TYPES OF INTRAVENOUS ACCESS DEVICES
IVAD, peripheral or central
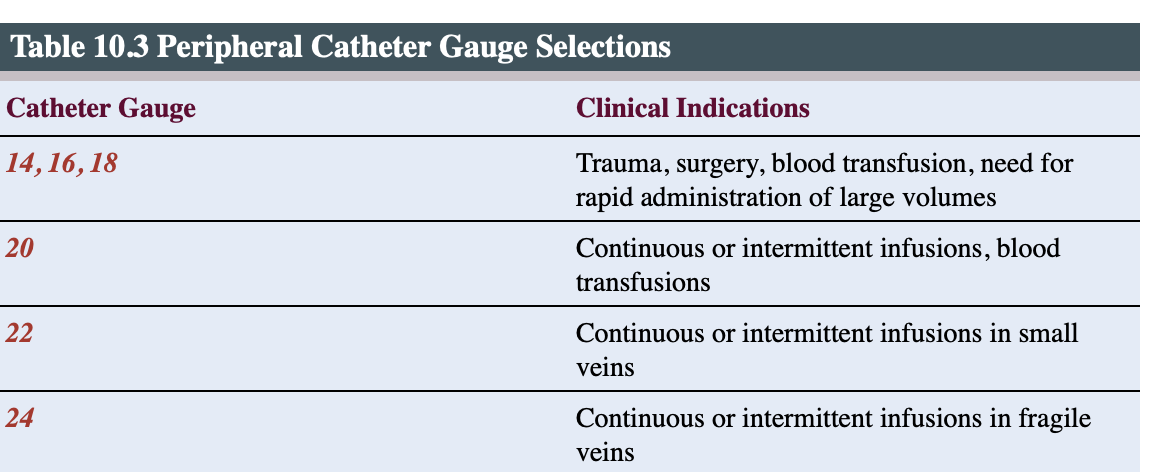
PVD- 14-27G: Therapies utilizing a short peripheral catheter should be expected to last less than a week, and indications include hydration and administration of pain medications and some antibiotics
established in the superficial veins of the upper extremity
Start from the distal and work upward.
Steel winged device: butterfly needle-short-term or single-dose therapy because the rigid steel needle is more likely to puncture the vein and lead to fluid or medication leaking out of the vein.
Midline catheter : inserted in a peripheral vein in the upper extremities with tips that terminate distal to the shoulder in either the basilic, cephalic, or brachial vein
used for therapy that last 1-4 wks
not used to administer vesicant or other vesicant solution e.g parentral solution oor solution less than 5pH or greater than 9 osmolarity.
Central Venous Access: When the tip of the IVAD terminates in the central vasculature at the level of the superior vena cava or the inferior vena cava.
These lumens are referred to as proximal, medial, or distal lumens depending on the location of the end of the fluid path on the catheter.
incompatible solutions can be infused using the different ports attached to each of the lumens
Each lumen requires initial flushing, which fills the catheter with the ordered IV solution, and flushing is also used to maintain the patency of the individual lumens if fluids are not being continuously administered.
Chapter 13-Cancer
2nd leading cause of death worldwide and in the US
Globally, the most common types of cancer are lung, breast, colorectal, prostate, skin, and stomach cancer.
Globally, women are more likely to develop breast, cervical, or colorectal cancer
men are more likely to develop lung, prostate, or colorectal cancer.
Cancer is more common in the US.
Cancer is generally regarded as a disease of advanced age and is linked to mutations that occur over time.
low in developing country where life expectancy is low.
Cancer-causing infections such as hepatitis and human papillomavirus (HPV) are the attributable etiology for cancer in 25% of cases in developing countries. carcinogen (cancer trigger) exposure varies across nations for different reasons, leading to different cancer disease patterns
The most common cancers in adults in the United States in order of greatest incidence are prostate, breast, and lung.
Risk factors- cumulative
Exposure to carcinogen
Modifiable risk factor
lifestyle- sedentary lifestyle; poor diet, smoking
Relationship between colon cancer and inflammatory bowel disease or hepatic cancer resulting from hepatitis C infection
Nonmodifiable risk
Age- Advance age
genetic- genetic syndrome
Cancer statistics
Males:Prostate
Lung and bronchus
Colon and rectum
Urinary bladder
Melanoma of the skin
Female: breast
Lungs and bronchus
Colon and rectum
Corpus and ureterus
Thyriod
Cancer characteristics
2 hallmark characteristics- uncontrolled cell growth and altered cell differentiation
Uncontrolled cell growth: Cancer cells lack contact inhibition.
cancer cells do not undergo apoptosis.
can grow and flourish in atypical patterns and environments.
This uncontrolled growth may result in dysplasia or deranged cell growth, in which cells vary in size, shape, and organization.
Cancer pattern is neoplasia- uncontrolled cell proliferation; malignant and grows and invase tissue and vessels.
Altered cell differentiation
When a cell loses expected structure and function, it is called anaplasia. As cancer proliferation progresses, the cancer cell loses similarity to the parent cell.
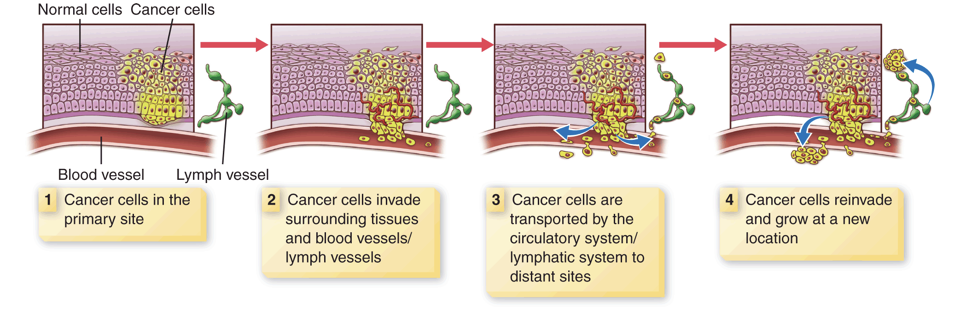
Metastasis:The propensity for tumors to spread is called metastasis.
Cancer cells spread by cell-to-cell transfer, through the lymphatic system, or through the blood (hematogenous).
Prostate cancer metasize to the rectum, pelvic floor, lower spine or hip
Colorectal cancer metasize hematogenously to the liver.
Types of Cancer
Solid tumor malignancies: arise from specific body organs and grow into masses that invade and erode normal body tissue as they expand in size. e.g lung cancer
Hematological malignancies: arise from cells of the hematopoietic cell line or from secondary immune organs such as the lymph nodes or spleen.
The three major subcategories of hematological malignancies are;
leukemia, cancers involving blood cells
lymphoma, cancers involving the lymphatic system
multiple myeloma, cancers involving plasma cells and immunoglobulins.
Staging of Cancer
The stage of disease is used to plan patient assessment, clinical management, and treatment strategies.
Sollid malignancy staging
T- tumor size
N-# of lymph node involved
M- presence of metastases
American Joint Communittee of cancer; define the staging
Cancer is generally staged along a continuum of one (I) through four (IV).
Stage I: A small tumor without obvious spread outside the organ.
Stage II: invasion of deeper tissues or involvement of local lymph nodes.
Stage III: large or locally invasive tumors, spread to the circulatory and lymphatic system
Stage IV: and cancers that have metastasized. They have moved to another location.
Clinical presentation
CAUTION symptoms- warning signs
constitutional symptoms- fatigue, unexplained weight loss, fever night sweat
Malignacy- specific S/s
Metastasis of cancer and Risk factor
Bladder cancer- tobacco and cigarettes
S/s: Hematuia
Abd discomfort
distended abd
low back pain
Metasises- Regional lymph nodes, bone, lung, skin, liver
Brain tumor- excessive Alcohol
S/s: headache
personality change
somnolence or hyperactivity
memory deficits
visual disturbance
facol motor deficit
Metastases: spinal cord
Brest cancer- Endocrine disrupter; early menses, late menarche, nulliparity, late 1st child, Genetic(BRCA1,BRCA2)
S/s: Breast mass
Axillary node enlargement
asynchrony of breast
nipple discharge
Metastases: bone, lungs, lymph nodes, liver and brain.