Vascular Disorders & Problems of peripheral Circulation pt.1
Cardiovascular Assessment
History & Physical
Health History
Family History
past medical history
past surgical history
medications
Activity
Exercise
Physical Assessment
BP & HR
Pulses
skin
Cap Refill time
Labs
medication levels
lipid panel
coagulation studies
CBC
CMP/BMP
HgbA1C
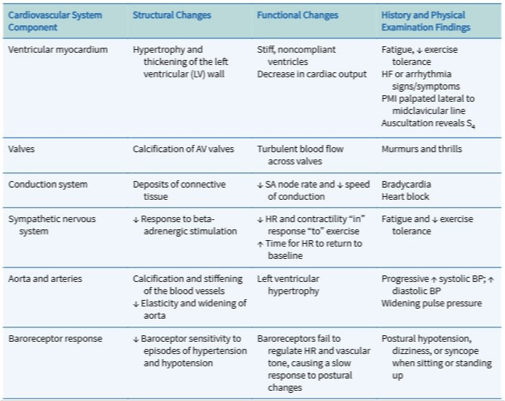
Gerontologic Considerations
Peripheral Arterial Disease (PAD)
= Difficulty getting perfusion to lower extremities
Caused by:
Atherosclerotic plaques
thrombemboli
Truma
Acute
Sudden ischemia
tissue death
Chronic (Gradual)
Collateral circulation
Compensatory
Slow ischemia & tissue death
Who is at risk?
Family history
Age (65 and older)
Smoking - causes sever vasoconstriction
Pre-existing health conditions:
Coronary artery disease (CAD)
Cerebral artery disease
Diabetes Mellitus
Hypertension
Dyslipidemia
Clotting disorders
Hyperthromocysteinemais
Clinical Manifestations
Structural changes
Hair loss distal to the occlusion
thick, opaque nails; shiny, dry skin
Skeletal muscle atrophy
Skin color changes:
Elevational pallor
dependent rubor (Red color when limb dependant from dilated damaged vessels)
Pulse changes:
Pulse diminidshed or absent belwo area of stenosis/obstruction-pedal, posterior tibial, popliteal, femoral
Cool extremity distal to occlusion
sensation changes:
Paresthesias
numbness
tingling of extremities
ulcer sor gangrene on tips of toes
edema
Critical limb ischemia
paint at rest
non-healing ulcers
Gangrene
Acute Limb ischemia
sudden decrease in perfusion
Intermittent Claudication = Carmp-like pain with exertion, relieved with rest, pain persists distally to problematic vessel, dependent position reduces pain.
Ankel-brachial index
Ankle SBP: brachail SBP
< 0.9 indicative of PAD
Diagnostic Studies
Doppler ultrasound
Invasive DIgital Angiography
asses allergies to iodine and contrast die
adequate renal function needed
Medical Management
Exercise - treats intermittent claudication
RIsk modification
Smoking cessation
weight loss
pharmacologic
Cilostazol: Vasodilator, interferes with platelet aggregation
ASA (Asprin) & Plavix: Antiplatelet agents
Statin (Anti-lipedema)
Anti-HTN
Thrombolysis
Injecting thrombolytic agent directly into thrombus]
Revascularization
Arterial bypass
angioplasty
Nursing Management
Post-operative care
Activity appropriate for pt Pain relief
Anticoagulant therapy
Monitor for complications
Report change in condition
Maintain tissue integrity
prevent amputation
Patient teaching
Avoid Trauma
Well fit shoes
wound care
risk modification
Upper Extremity Arterial Occlusive DIsease
Caused by:
Vasospasm
trauma
constrictive arterial disorders
Subclavian Steal syndrome = while arm is being used, preferential blood flow reverts to the extremity and away from the brain
Clinical Manifestations
Arm pain & fatigue with exertion
Dizziness
vertigo
Ataxia
Syncope
Bilateral visual disturbances
Nursing Assessment
coolness
pallor
decreased CRT
Decreased Amplitude in radial pulse
Arm BI difference of > = 15 mmHg
management
surgical bypass
percutaneous transluminal angioplasty (PTA)
Raynaud Disease & Phenomenon
DIsease Vs. Phenomenon
Primary
Idiopathic
vasospasm due to cold or stress
Secondary
disease processes that mimic s/s of Raynaud’s
EX. Scleroderma, SLE
Phenomenon - initial = white in fingertips - sustained = blue - resolved = red meaning blood flow returned
Management
typically benign and self-limiing
Avoid stimuli that provoke vasoconstriction
Dress warmly to prevent reflex vasoconstriction
tobacco is contraindicated
calcium-channel blockers
digital sympathectomy
Thromboangiitis Obliterans (Buerger’s Disease)
autoimmune vasculitis
recurrent inflammation in small arteries and veins causing occlusion
occurs most in males, between 25-45 yos
#1 cause = smoking
manifests as bilateral pain
can occur in feet
Treatment
Sympathetic block - dilates vessels & increases blood flow
Smoking cessation