Section 1a: Anatomy & Physiology of Skin & Hair (pg. 3-119)
Anatomy of Skin and Hair (Pg. 3-23)
Structure of the Skin
Healthy skin has elasticity and, when pinched or pulled, quickly reverts to its normal shape. It’s color derives from a combination of melanin produced in the stratum germinativum; carotene, a yellowish pigment; and the concentration of blood vessels found in the dermis. It is approximately 1/5 of an inch thick at its thickest, on the soles of the feet to a 12th of an inch at its thinnest on the eyelids.
The skin is the body’s largest organ in surface area, covering up to 20 square ft. It is made up of epithelial tissue (no blood) and connective tissue (blood) and consists of three main layers: The Epidermis, The Dermis, and The Subcutaneous Layer or Subcutis
The Epidermis
The Epidermis (Scarf, Cuticle, Epithelial Tissue = No Blood ) | |
AKA: Scarf (Protective), Cuticle, No Blood Made up of 2 zones: Horny Zone & Germinal Zone As thick as a piece of paper. These 2 zones consist of 5 layers that can be memorized with the acronym Come, Let’s Get Sun Burned / Girls | The Horny Zone: The outer portion of the epidermis, is divided into three layers - Stratum Corneum, Stratum Lucidum, Stratus Granulosum. Acts as a barrier against bacterial invasion and water absorption. The Germinal Zone: Two main layers (Stratum Spinosum/ Stratum Basale/Germinativum) of differing cells make up the germinal or, as it is also known, the living or basal zone |
Stratum Corneum Outermost layer | The outermost layer of the epidermis, consists of dead skin cells which are constantly shed. These cells are predominately bound by sebum, the skin’s natural lubricant. |
Stratum Lucidum Clear Protein Eleidin; transparent; found in palms and soles | This layer gets its name from the transparent nature of the cells that contain eleidin; a clear substance derived from keratohyalin granules. Found only in the palms of the hands and soles of the feet where the epidermis is thickest. Not found in thin skin (i.e. eyelids). |
Stratum Granulosum Calluses form here | The cells here have nuclei and are still living. As these cells are pushed upward by new cells, they lose their nuclei and die. This layer varies in thickness. It is thickest in the palms and soles and thinnest on the eyelids. Persistent friction and pressure cause areas to thicken for protection and form calluses. |
Stratum Spinosum Prickle cell layer | Also known as the prickle cell layer because of the cells’ prickly shape. Living cells, each cell is attached to the cells around it by prickly shaped fibers. |
Stratum Basale/Germinativum Lowest layer of Epidermis Mitosis (cell division) Melanocytes (Melanin production) Where Skin Cancer Begins | The lowest layer of the epidermis, also known as the innermost layer of the epidermis, or basal layer. Mitosis (cell division) takes place here as new epidermal tissue is formed and begins migrating to the surface of the skin, replacing the dead skin cells that have been shed. This is known as desquamation (act of exfoliation) and takes approx. 28 days (shorter when younger, longer when older). Melanocytes exist in this layer. |
The Dermis
The Dermis (Living Layer/Tissue, Connective Tissue = Blood, “True Skin”) | |
AKA: The Living Layer/Tissue, True Skin, Corium, Cutis Vera, Derma, Connective Tissue = Has Blood | The dermis is made of dense connective tissue and divided into two layers called the Papillary Layer and the Reticular Layer. Nerves and blood vessels course though this layer. 1-4mm thick |
The Papillary Layer Strongest Portion of the Dermis Made of Papillae Meissner’s Corpuscles (Touch) Collagen | Lies directly below the epidermis and is made of papillae - elastic collagen and reticular cone-shaped fibers with finger like projections that protrude upward into the epidermis, locking the two layers together. Meissner’s corpuscles, which are tactile nerve ending sensitive to touch, are in this layer. |
The Reticular Layer Thickest layer of the skin Dense Bundle of Collagen Many appendages | In the reticular layer there are numerous appendages: arrector pili muscles (goosebumps), blood vessels, fat cells, hair follicles, lymph vessels, nerve endings, sebaceous glands (oil), and sudoriferous glands (sweat). Collagen fibers are thick and densely packed here, elastic fibers are thinner and more loosely arranged here. |
The Subcutaneous Layer
The Subcutaneous Layer (Subcutis, Hypodermis, Adipose Tissue/Fat) |
At the base of the dermis is a layer of fatty tissue called the hypodermis, subcutaneous layer, subcutis, or adipose tissue. |
This layer varies in thickness depending on the individuals age, sex, and overall health. Many of the arteries, veins and lymphatics circulate through this area, as do nerve endings and an abundance of fat cells. This layer protects against injury/impact, i.e. hits and falls. |
The Structure and Function of the Skin
As the body’s largest sensory organ the skin has multiple functions, including protection, heat regulation, excretion, secretion, absorption, sensation, and the synthesis of Vitamin D. Healthy skin should have hair, as hair plays an important role in many of these functions.
Protection
Secretion and Excretion
| Heat Regulation
Absorption and Penetration
Sensation
|
Degrees of Skin Burns (Layers of Skin):
1st Degree: Epidermis (superficial burn)
2nd Degree: Epidermis and Dermis (severe sunburn; hot water burn)
3rd Degree: Epidermis, dermis, and subcutaneous → can be fatal, skin graft may be needed, permanent scarring and possible infection
4th Degree: Rarely see; down to the muscles and bones, normally fatal
Cellular Components of Skin
Melanocytes: Dendritic pigment-producing cells located in the basal (germinativum) layer of the skin. The protect the skin from UV radiation. People of all races have a similar number of melanocytes. The difference in skin pigmentation depends on (1) the number of the melanosomes and (2) their dispersion in the skin. Sunlight stimulates melanocytes to increase pigment production and more widely disperse melanosomes.
Langerhans Cells (found in epidermis): Dendritic cells in the epidermis that have an immunologic function. They fight infection in the skin and digest impurities on the skin like pacman.
Basement Membrane Zone (BMZ): The BMZ serves as the “glue” between the epidermis and dermis and is the site of blister formation in a number of diseases
Skin Appendages
Sudoriferous Glands: The sweat glands controlled by the sympathetic nervous system. They are found deep in the dermis and have tubular ducts extending all the way up to the pores of the epidermis. There are two types of sweat glands, (1) eccrine and (2) apocrine.
Eccrine Sweat Glands (Sweet Sweat): They help to regulate body temperature by excreting sweat onto the surface of the skin, from which the cooling process of evaporation takes place. Located all over the body, but in increased numbers on the forehead, palms of hands, and soles of feet. They excrete mainly water with a little salt, urea and other water-soluble substances.
Apocrine Sweat Glands: In humans, they serve no useful function, but they are responsible for body odor. Located mainly in the axillae (armpit) and genital areas and usually open into hair follicles. The substances emitted from these glands mixed with bacteria on the skin surface create body odor. They are believed to excrete pheromones which are thought to play a role in sexual attraction.
Hair Follicle: In humans, hair is mainly decorative. Hair follicles are distributed over the entire body surface except the palms and soles. Hair comes in two sizes: (1) Vellus hair; which are short, fine, light colored, and barely noticed. (2) Terminal Hairs; which are thicker, longer, and darker then the vellus type. In some locations they are hormonally influences and don’t appear until puberty (beards, pubic, underarms)
A hair follicle can be viewed as a specialized invagination (indentation, depression) of the epidermis with a population of cells at the bottom (hair bulb) that are even more actively replicating than are normal epidermal basal cells.
Melanocytes in the matrix contribute pigment, the amount of which determines the color of the hair.
As the matrix cells continue to divide, hair is pushed outward and exits through the epidermis at the rate of about 1cm per month. Hair growth in an individual follicle is cyclical, with a growth (anagen) phase and a resting (telogen) phase. Lengths of phases vary depending on area of the body. On the scalp anagen phase lasts about 6 years and telogen phase about 4 months.
Sebaceous Glands: Produce an oily substance called sebum, which lubricates skin and hair. Found wherever hair follicles are located as they are part of the pilosebaceuos unit. Found in greater numbers on the scalp, the T-Zone, and the cheeks. Vary in size and shape, influenced by endocrine system.
Blood and Lymph Supply: Lymph glands produce lymph, which is made of white blood corpuscles and plasma. HIV stores in blood & body fluid, i.e. lymph fluid
Anatomy of Hair and the Pilosebaceous Unit
The hair and its follicle are major appendages to the structure of the skin. Hair is found all over the body, with the exception of the soles of the feet and the palms of the hand. A great deal of hair on the body is invisible to the naked eye. Hormones and genetics influence hair growth at different ages in males and females.
What is the meaning of pilosebaceous unit?
[Pilo] → Hair
[Sebaceous] → Oily Gland
Sebaceous glands are a source of new hair; oil lubricates hair
The Structure of the Hair
Healthy hair is continually growing, shedding, and being replaced. The hair sits in a pocket in the skin (indentation or depression in the epidermal tissue) - imagine a finger poking into a balloon, so that balloon indents. In similar fashion, parts of the epidermis go down around the base of the hair and back upward, to the surface.
Straight Hair → Round Shaped Follicle
Kinky Hair → Flat Shaped Follicle
Wavy Hair → Oval Shaped Follicle
The Follicular Canal and Sheaths
The space the hair occupies is called the follicular canal. The outer sheath of the canal is formed from the basal cell layer. The inner sheath of the follicular canal, which is made of horny epidermal tissue, is called the external root sheath.
The Hair Shaft
The hair shaft is lined with epidermal tissue and in full-grown, active-hair stage extends downward, through the dermis to the subcutaneous tissue.
The epidermal cells are responsible for producing the hair follicle and the hair matrix. The base of the follicular canal widens (enlarges) to the hair follicle bulb.
The bulb, the area where the hair grows, contains the dividing cells of the hair matrix that produce the hair and the protective external and internal root sheath.
The Dermal Papilla and Papillae
The dermal papilla at the base of the hair bulb is an indentation which is the layer of dermal tissue that attaches itself to the epidermis with protrusions called papillae.
These papillae contain the blood supply needed for providing nutrients for growth as well as the hormones that stimulate hair growth.
Blood and hormones nourish hair
The root or papilla of the mature terminal hair is found in the lower part of the dermis (can reach to subcutaneous), and the hair shaft reaches up to its follicular opening in the epidermis.
The Arrector Pili Muscle (NOT a nerve)
The arrector pili muscle is an appendage to the hair follicle that is attached to the underside of the follicle midway between the bulb and the sebaceous gland.
The arrector pili muscle is partially responsible for heat regulation. Both fear and cold stimuli cause the arrector pili muscle fiber to contract, lifting the hair straight upward. Giving us “goose bumps” or “goose flesh”.
The Sebaceous Gland
Is attached to the hair follicle and opens into the follicular shaft. It secretes sebum, a protective fatty, oily substance that lubricates the hair (and skin), preventing it from becoming dry and brittle, thus breaking.
The sebaceous gland also prevents the epidermis from drying and cracking, preventing bacteria and germs from entering the skin.
Additional Notes
Hair growing longer on the head is due to distribution flow of the hormone androgen throughout the body
The hair bulge is the area where stem cells exist
Layers of the Hair
Three layers compose the hair (1) cuticle, (2) cortex, (3) medulla.
The Cuticle: Outermost Layer Ridges Protection | The outermost layer of the hair. It is composed of transparent cells that overlap like scales (you can feel the ridges when sliding upward on the hair shaft). The purpose of the cuticle is to protect the inner layers of the hair. |
The Cortex: Middle Layer Melanin Strength & Elasticity | Below the cuticle lies the cortex. This middle layer is made of elongated cells of fibrous tissue and the pigment that gives hair is color (melanin found here). Its also the layer that gives hair its strength and elasticity. |
The Medulla: Innermost Layer Fine Hair = No Medulla Curly Hair = Strong Medulla | The innermost layer of the hair. Made of round cells, the medulla is also called the pith or marrow. Fine hair lacks the medulla. Can be found in all wavy hair. In general, the curlier the hair, the stronger the medulla. |
Types of Hair (Lanugo, Vellus, Terminal)
Hair follicles can produce vellus or terminal hair, which can be affected by age, genetics, health, and the hormonal changes of puberty, pregnancy and menopause.
Lanugo: Fetal Hair Develops 3m prior to birth Sheds a few weeks post birth | Lanugo, soft, downy hair, is also called fetal hair because it is on fetuses in utero (develops about 3 months prior to birth) and on infants at birth, covering their bodies and scalps. It may contain pigment and be light or dark. It often sheds a few weeks after birth. |
Vellus: Peach fuzz Present in adulthood Woman have more | Present through adulthood. Fine and short, often called peach fuzz. Often has no pigment or medulla. Women are believed to have 55% more vellus hair than men, and it can be found on women’s faces where men produce beards and mustache hair at puberty onward. |
Intermediate Vellus Hair: | Vellus hair that starts to acquire pigment and become coarser |
Terminal: Medullated and Pigmented | Longer, coarser, pigmented hair that covers the scalp and is found on the arms and legs. At puberty, it is also found in groin area and axillae, as well as on the face of men and occasionally the chest and back. |
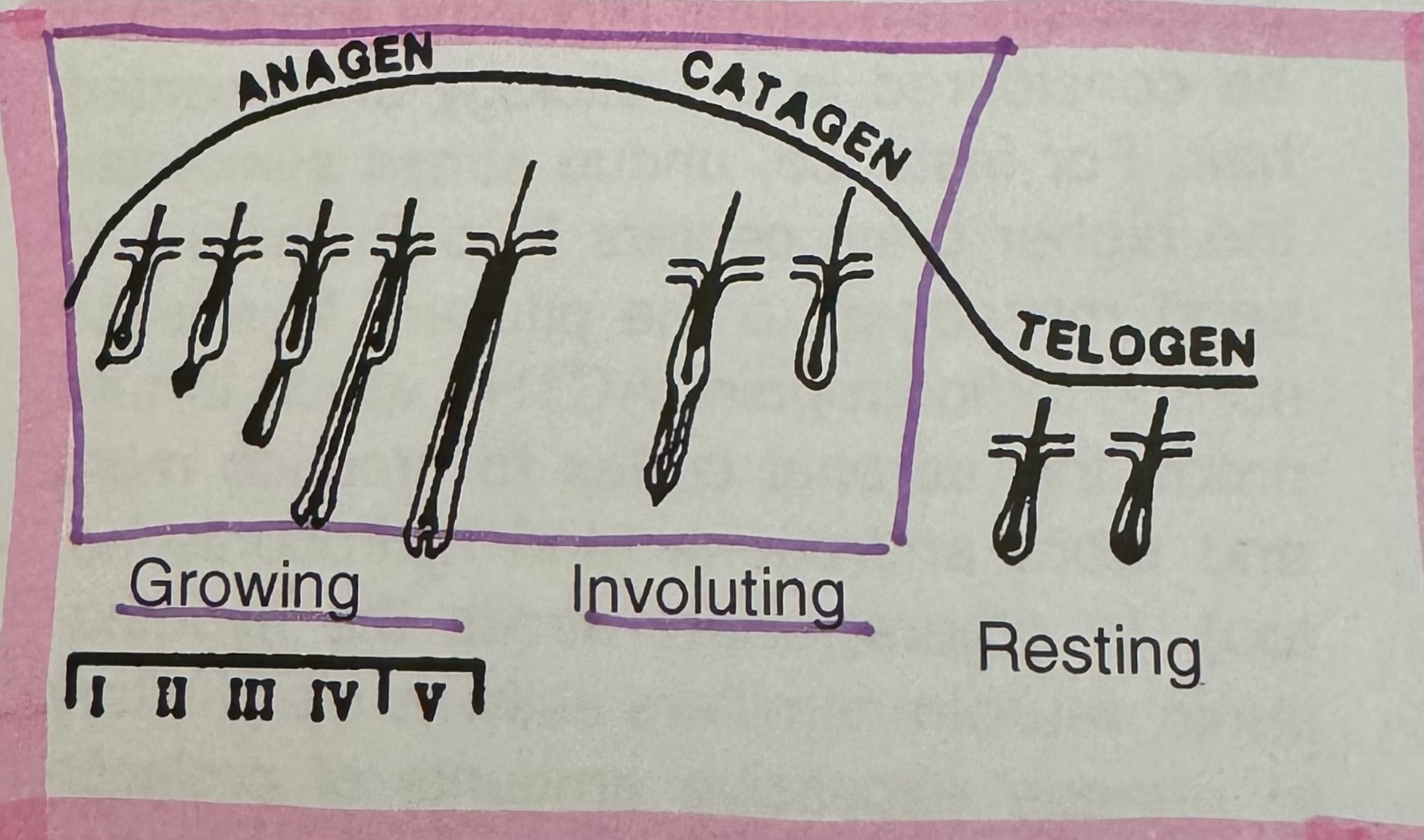
Hair Growth Cycle (Anagen, Catagen, Telogen - ACT)
Anagen: The Growing Phase Ideal phase for hair removal/ treatment of hair | The hair’s active growing phase, when the hair follicle is at its deepest. At this stage the hair matrix is active, encapsulating the dermal papilla, and the bulb of the hair is visibly darker. Once a growing anagen has reached its full length, it can remain for varying amounts of time (depending on location) for a few weeks on the finger to 8 years on the scalp.
Gray hair is deepest rooted hair, tough to treat. |
Catagen: The Transitional Phase (Involution) Shortest Hair-Growth Phase Club hair starts here | The shortest hair-growth phase, lasting for only a few days to a few weeks. Occurs when the hair follicle separates from the dermal papilla. Follicle shrinks and cord attaching follicle retracts upward. |
Telogen: The Resting Phase Shedding | The base of the hair looks like a club, getting the name club hair. Club hair starts in catagen and finishes in telogen. The bulb is usually white. The hair is released by the end of the telogen phase. |
Extra Notes/Hair Growth
Hair grows faster in the summer which tells us that heat stimulates growth
Telogen hair increases (more hair loss) during illness, after childbirth, and when an individual experiences stress
Excess androgens (male hormones) may certainly stimulate terminal hair to regrow faster meaning a shorter telogen phase.
Soft and Hair Keratin
Hair → Hard Keratin
Nails → Hard Keratin
Skin → Soft Keratin
Retin-A, Herpes, Warts, Skin Cancer (Pg. 24-28)
Photo aging (light + aging) of the skin refers to the fact that sunlight (as well as your heredity), not just age, is responsible for most features of “old looking” skin. “Today’s suntan is tomorrow’s wrinkles“ refers to the fact that the sun disintegrates the skins elastic fibers.
CANCER
Do not perform services without a doctors clearance on patients who have or have had skin cancer. Malignant melanoma is deadly.
Most skin cancers begin as small bumps or red scaly patches which don’t completely heal. They may grow large, bleed or form ulcerated sores. Any sores that do not heal or a mole that changes or gets flaky or darker should be seen by a doctor.
Malignant melanoma, a relatively uncommon cancer of the skin, occurs as a dark brown, small mole like growth. This becomes larger and may bleed or become an ulcerated sore.
WARTS
Warts are growths caused by a virus that affects the skin. They are contagious.
HERPES
Herpes is a virus that causes cold sores (herpes 1), fever blisters (Blistering rashes around the mouth or groin areas - herpes 2).
No one knows why herpes emerges from the nerve tissue under the skin. Through observation, we know that there are numbers of things that bring it on. Emotional stress, fatigue, high fevers, colds, menstrual cycle, and gastrointestinal upset are but a few. Even sunburn and windburn have been known to bring on herpes attacks, and this can be for the most part prevented by using a sunscreen.
Exam Q: Herpes infections are usually recognizable by their typical group of water blisters or pus pimples in a single area.
Herpes is extremely contagious, especially type 2.
Guidelines ‘97-’98 For Permanent Hair Removal: Using Electrolysis Modalities (Pg. 29-33)
Accutane = Isotretinoin; part of the retinoid family. Because it can change the function and structure of normal skin, it can have an effect of electrolysis treatment.
With regard to tissue/skin injury from chemical, peels and dermabrasion, there is some concern over the possibility of increased scarring when these procedures are performed during the use of Accutane and for up to six months after.
How does Accutane affect electrolysis?
The client skin will usually be more red and appear thinner/more transparent.
There is no definite contraindication for the use of any electrolysis modality, but expect even more redness and sensitivity as compared to Retin A.
Postponing electrolysis on the face until one month after the client stops Accutane is advised.
How does low concentration, alpha hydroxy acids affect electrolysis?
Slight increased redness, may be noted during and after treatment
Examples of AHA’s include glycolic acid (sugar cane), lactic acid (sour milk), citric acid (fruits), malic acid (apples), tartaric acid (grapes), and mandelic acid (bitter almonds)
How does dermabrasion affect electrolysis?
The removal of the superficial portion of the skin (epidermis and outer dermis) by means of an abrasive device.
Small milia are common after dermabrasion; electrolysis can be performed around these lesions.
It is recommended that a period of three months elapse before electrolysis is performed on previously dermabraded skin. If the skin is still red, electrolysis should be postponed until all redness has disappeared.
VERY IMPORTANT SECTION: Tetracycline Antibiotics
Frequently used tetracyclines include:
Tetracycline hydrochloride
Doxycycline
Minocycline - acne treatment
Diseases frequently treated with tetracycline:
Acne
Lyme disease
Rosacea (acne rosacea)
Noteworthy side effects:
Pigmentation of the skin can occasionally occur with minocycline in areas of injury; Minocycline can cause brownish gray pigmentation in areas of injury.
Skin grafts
With electrolysis skin grafts can affect the treatment because distorted follicles in scars are likely to be present.
How do laser procedures affect electrolysis?
For laser resurfacing of selected facial units, such as the upper lip or chin, wait at least two months or until the skin is no longer red or tender before attempting electrolysis.
If in doubt check with the physician who performed the procedure.
Diabetes (Diabetes Mellitus)
Diabetes is a disorder of carbohydrate, metabolism that involves insulin deficiency and or insulin resistance. All causes of diabetes lead to hyperglycemia or high blood pressure, which is the hallmark of this disease. There are three main types:
Type 1 diabetes: Juvenile diabetes; insulin dependent, this form usually develops prior to early childhood
Type 2 diabetes: Non-insulin-dependent. This form usually develops later on in life, and the patient may or may not be on insulin.
Gestational diabetes: diabetes that develop during pregnancy.
Peripheral vascular disease is quite common in diabetic patients and is usually manifested by poor circulation, especially in the lower legs
Guidelines for performing electrolysis on diabetic clients:
The main area you need to be concerned with is the lower legs from the knee down. If there are open sores on the legs or feet do not work on the area.
Also do not work on any skin that does not appear healthy.
Pregnancy
Guidelines for performing electrolysis on pregnant clients:
Do not perform electrolysis on the abdomen or breast during the last trimester (last 3m) of the pregnancy using any modality.
Pacemakers/defibrillators
Always have the client check, or you check, with the clients cardiologist regarding the safety of electrolysis and the specific device.
Cellular Activity of the Bulge Region and Ramifications for Electrologists (Pg. 34-35)
The hair follicle bulge is situated close to the sebaceous glands, at the boundary between the permanent hair (I.e. upper portion) and transient hair (I.e. lower portion) and close to the insertion of the arrector pili muscle to the hair follicle.
The bulge is likely to control the hair follicle cycle. It appears that there are two areas to target, the bulge and the bulb. The stem cells of the bulge will be more resistant to heat because of their poor ability to multiply.
Outer Root Sheath (ORS)
Inner Root Sheath (IRS)
It seems that the optimum results in permanent hair removal, would be achieved by destruction of cells beginning at the bulge region and following on down along the hair shaft to the bulb.
*Reference image on page 34 to know how to identify the bulge for exam
The Growth Cycle (Pg. 36-38)
The Anagen Phase (Active Growth)
This phase can be divided into two sections; (1) the reconstruction of the hair bulb and (2) the growth of the hair. The early phase is signaled by mitotic activity of the hair germ. Mitotic activity is the continuous process of cell division: one cell divides into two cells, two into four, and so on. Through this activity, the hair germ grows and builds a solid cord that extends deeper into the dermis to surround the papilla and form a new onion shaped bulb. The bulb is the thickest or widest part of the follicle and consist of the lower third of the follicle, which is short when the bulb is formed.
The duration of the anagen phase varies based on the location of the body: from a few weeks on the fingers, 4-6 months on the thigh, to 3-8 years on the scalp.
The Catagen Phase (Transitional)
When the growing hair has reached its full length, the anagen phase ends, and the catagen phase begins with the cessation or stopping of melanin production of the melanocytes in the upper part of the bulb. The last step of the catagen follicle is the building of the club. The lower end of the catagen hair becomes keratinized and builds the hair club, which is anchored into the germ-sac.
The Telogen Phase (Resting)
Some of the club hairs formed during catagen may fall out in telogen; but mostly, they are shed in the early part of the anagen phase as the new hair shaft approaches the surface of the skin.
Hair Growth Table (Pg. 39-41)
Hair grows faster during the summer, with good health, and in the young.
If your clients have waxed, plucked or received electrolysis within the last four months, those hairs will take 2-4 months to regrow depending on the body site.
The total number of hair follicles in each individual does not increase after birth, but the number does gradually reduce with increasing age.
Factors involved in Hair Growth and Regrowth
Visible hairs may be vice, intermediate, or terminal. Anagen hair is only visible once it has emerged through the surface of the skin.
On the scalp 13% of resting hairs are in telogen phase. 85% of growing hairs are in anagen phase.
Hirsutism (Pg. 43-48)
Hirsutism is excess body hair. It is a frequent complaint among women.
Normal hair growth and its control
The number of hair follicles/skin area is greater in Caucasians than in Orientals and greater in Mediterranean than in Nordic individuals. Hair grows from hair follicles within the skin. Only the souls and palms are free of hair follicles.
There are two types of hair in the adult; vellus hair and terminal hair. Vellus hair are soft, fine, and usually short. They may be colorless, giving the impression of “hairless skin“. Examples of vellus hair in women are found on the face, chest, back, etc. Terminal hairs are longer, coarser, and thicker, such as those found in the scalp, pubic area and axilla of both men and women. In men, they are also found on the face and body.
Various hormones control hair growth. Thyroid hormone and growth hormone affect hair growth. The most important hormone controlling growth are “androgens” commonly known as “male” hormones. The most important one is testosterone. A good example is puberty in which, in both sexes, androgens induce the appearance of pubic and axillary hair. “Estrogen” or female hormones have the opposite effect.
Exam Q: Once vellus hair has been transformed into terminal hair it cannot change back even if androgens disappear.
What constitutes hirsutism in women?
All women have terminal hair in some parts of the body, specifically the scalp, pubic and axillary area. A few hairs around the nipple or over the thighs may be normal.
Hirsutism: Excess body hair in women, presence of thick, usually dark, hair over the face, chest, abdomen, upper thighs or upper arms.
Hirsutism must be distinguished from “hypertrichosis“. This condition is characterized by excessive growth of vellus type hair, which may be darker than usual. This is very common of women of Mediterranean descent, and usually runs in families.
What causes hirsutism?
Exam Q: Hirsutism is almost always the result of excess effect of androgens on the hair follicles. The excess androgens can be:
Exogenous: The use of male hormones and medications with androgen effects will stimulate hair growth. An example is Danazol used in endometriosis.
Ovarian
Androgen producing ovarian tumors: hirsutism progresses rapidly and left untreated leads to masculinization (loss of scalp, voice changes, male body habitus).
Mixed gonadal dysgenesis (hermaphrodite): This is a rare condition of genetic origin in which either remnants of testicular tissue are found in an ovary. Most affected individuals present marked hirsutism upon initiation of puberty.
PCOS: AKA - Chronic Anovulation or Stein-Leventhal Syndrome
Familial Hirsutism = Idiopathic
Iatric Hirsutism = Medication Induced
Adrenal: Cushing’s syndrome: the condition is the consequence of excess production of corticosteroids in the adrenal gland. Corticosteroids are a family of hormones produced by the adrenal gland. Some pituitary tumors produce excess ACTH, a hormone that stimulates the adrenal gland to produce corticosteroids. Some of the corticosteroids in the adrenal are androgens, and therefore stimulate hair growth.
Local/intra-follicular or idiopathic: there are some patients who present with hirsutism, but ovulate regularly. Their hormonal levels are normal, and no apparent explanation is found for their hirsutism. This category of patients have been labeled “idiopathic“ or “familial hirsutism“. The only satisfactory explanation for this distressing problem is hypersensitivity of the skins hair apparatus to normal levels of androgens.
Treatment of Hirsutism
Tweezing causes an increased blood supply to the tweezed hairs and adjacent hairs, causing an increase in the follicle structure.
Although many women find the thought unpleasant, close shaving is the best method for temporarily removing unsightly hair. The only permanent way of removing excess hair is by electrolysis. The electrologist uses a very fine current needle, placing it down the hair shaft and into the hair follicle. Electrolysis should not be performed until hormonal therapy has been used for at least six months.
Hormonal therapy will stop new hair from developing. Terminal hairs that are already present. Do not fall out or disappear with hormonal therapy and must be removed by electrolysis.
Birth control pills:
Birth control pills stop the excessive hair growth by decreasing the Pituitary hormones LH and FSH. Birth control pills can also be combined with spironolactone or a corticosteroid (prednisone or dexamethasone).
Spironolactone: also used to treat high blood pressure and heart failure. Spironolactone or Aldactone is a drug which was initially intended as a diuretic “water pill”. Andocur is banned in the US.
Corticosteroids (Prednisone, dexamethasone): Corticosteroids are used when the adrenal is thought to be overactive or to treat autoimmune diseases, for example lupus. They can stimulate excess hair growth, prednisone, and dexamethasone (decadeon) are synthetic man-made corticosteroids.
Idiopathic Hirsutism (Pg. 49-52)
Idiopathic hirsutism may be defined as unwanted hair for which no positive factor is apparent. It is by far the most common of all the disorders associated with inappropriate hairiness and often is referred to as genetic or familial hirsutism.
PATHOPHYSIOLOGY
The skin of both males and females contains similar numbers of hair, follicles or pilot sebaceous units.
Normal masculine and feminine patterns of hair distribution are dependent on levels of androgens, or so-called male hormones, in both men and women. For instance, pubic and axillary hair in a woman will not appear if she is suffering from sexual infantilism due to loss of pituitary gland function.
Sexual hair, i.e., facial, ear, chest, abdominal, pubic and axillary, lower limbs, and abdomen is hormone dependent.
All hair follicles undergo a cyclical pattern of growth. What actually determines the rate of change from growth (anagen) to regression or involution (catagen), or from resting (telogen) to growth are not known.
During the growing phase, the follicle consists of three major structures: follicular sheath (upper and lower), follicular bulb, and hair shaft. Seasons influence, the rate of human hair growth: hair growth faster in the summer than in the winter months.
The Role of Androgens
The ovaries produce androgens in excess; menstruation occurs quite irregularly, and patients are, as a rule, anovulatory (can’t ovulate). The hirsutism may be so marked as to defeminize the patient, despite the presence of good breast development.
Signs of virilism are amenorrhea, marked hirsutism, enlargement of the clitoris, lowering of the voice, and increased muscle mass. There are, however, expectations. Occasionally one may encounter of viralized woman who menstruates regularly, or a feminized, but hairy one, who may be amenorrheic. When hirsutism is not attended by menstrual disturbances or fertility problems, it is sad to be idiopathic.
Treatment
Access hair growth in females (hirsutism) can be caused by increased sensitivity to her own androgens.
Polycystic Ovarian Syndrome and Understanding PCOS (Pg. 78-88)
What is PCOS?
PCOS is a health problem that can affect a woman’s menstrual cycle.
What causes PCOS?
The cause of PCOS is unknown. A main underlying problem with PCOS is a hormonal imbalance. In women with PCOS, the ovaries make more androgens than normal. Androgens are male hormones that females also make. High levels of these hormones affect the development and release of eggs during ovulation.
Many women with PCOS have too much insulin in their bodies because they have problems using it. Excess insulin appears to increase production of androgen. High androgen levels can lead to: Acne, excessive hair, growth, weight gain, and problems with ovulation.
Symptoms of PCOS
Symptoms of PCOS can vary from women to woman. Some of the symptoms of PCOS include:
Infertility
In frequent, absent, and or irregular menstrual period
Hirsutism - Increased hair growth on the face, chest, stomach, back, thumbs, or toes
Cysts on the ovaries
Acne, oily skin, or dandruff
Weight gain or obesity
Male pattern, baldness, or thinning hair
Acanthodis Nigracans (exclusively related to diabetes): Patches of skin on the neck, arms, breasts, or thighs that are thick and dark, brown or black.
Skin tags, excess flaps of skin in the armpits or neck area (Arochordan)
Medicine for increased hair growth through extra male hormones
Medicines called anti-androgens or androgen suppressants may reduce hair growth and clear acne. Spironolactone, (Aldactone) first used to treat high blood pressure, has been shown to reduce the impact of male hormones on hair, growth and women. Finasteride, taken by men for hair loss, has the same effect. Anti-androgens are often combined with birth control pills.
Who should have a work up for PCOS?
Any woman who has some of the following symptoms should consider having an evaluation work up for PCOS. (This is intended as general information. Only medical diagnosis must be done through consultation with the physician):
Very only skin
Persistent acne
Facial or body hair that requires more than occasional removal
Loss of scalp pair. This is common with PCOS, but many women have hair loss without any other changes. This is known as alopecia (female alopecia = alopecia areata) or androgenic alopecia.
Darkening of the skin on the back of the neck or under arms - acanthosis nigracans
Irregular periods, periods usually more than five weeks apart, or prolonged, or heavy bleeding
Difficulty controlling weight, especially if the extra weight is on the upper part of the body or the abdomen
Skin and hair changes
The skin and hair changes are due to the effect of testosterone on the oil glands and hair follicles. There are two parts to the treatment: lowering the testosterone, and blocking the effects of testosterone.
If testosterone levels are elevated, treatment usually includes lowering them. The best way to do this depends on where the extra testosterone is coming from. When it comes from the ovary, oral contraceptives usually lower it by as much as half. In rare situations, other medications can be used to suppress the ovary more completely.
When the testosterone comes from the adrenal, a cortison- like medication called dexamethasone can be used in low doses to partially suppress the adrenal so that it makes less testosterone. This medication is used only in special circumstances and in very low doses.
Hirsutism, Diabetes and Heart Disease (Pg. 89-92)
The improvement of hirsutism occurs slowly, often requiring 6 to 8 months of therapy prior to observing a difference.
Obesity
Obesity has been associated with PCOS since Stein and Leventhal describe the syndrome. The presence of obesity is associated with increased metabolism of androgens, reflected in both and elevated production and clearance rate.
Insulin resistance/type 2 diabetes mellitus
Approximately 1/2 of patients with PCOS demonstrate insulin resistance.
Malignancy
Chronic anovulation is well known risk factor for the development of endometrial carcinoma. More specifically untreated PCOS is a significant risk factor for endometrial carcinoma.
Conclusions
In conclusion, patients with PCOS are at higher risk for developing obesity, type two diabetes, colitis, hypertension, lipid abnormalities, CAD or coronary artery disease, and endometrial carcinoma. The following periodic and preventative care in patients with androgen excess is recommended:
Stress, weight loss, smoking cessation, regular exercise, and a reduction in high fat dietary intake. If hypertriglyceridemia is evident, the patient should be encouraged to discontinue alcohol consumption and the negative impact of estrogenic preparations, i.e. oral contraceptive pills, should be monitored.
Hair Growth: The role of Heredity, Genetics, and Androgenic Metabolism (Pg. 93-96)
Hair growth is cyclical: anagen or growing phase; catagen or transitional phase of involution; and telogen or the resting phase.
The duration of each phase in the human depends on many factors. Each follicle is nurtured by one or more sebaceous glands which produce an oil lubrication film, which protects the hair. Usually, although not always, increased hairness is signaled by increased oiliness. In addition, each terminal hair, not vellus hair, follicle has a special attachment, called the arrector pili.
Excessive hair growth, especially on the face on a woman, known as hirsutism, is often regarded as a lack of femininity, but it need not be a deterrent to essential womanhood. Only when we have clitoral hypertrophy (Including male pattern, baldness, deepening of the voice, increase muscle mass, and amenorrhea), can we speak of virilism.
Hair is a derivative of the epidermis, and the hair follicle is part of the Pylos sebaceous system. All of these elements are present at least three months prior to birth, and it is rare that any new hair follicles will develop in the human adult. Incidentally, there is no difference whatsoever between the male and female distribution of hair follicles. The difference between males and females in regard to sexual hair patterns is due mainly to the concentration of circulating androgens.
Androgen, derived from adrenal, testes and ovaries.
Simply put excessive hair growth may be caused by an increased sensitivity of the hair follicle to endogenous (Originating within an organ) androgens. Usually, this is a hereditary trait. On the other hand, in the greater number of hirsute women displaying what is called “idiopathic hirsutism” there may be enzymatic defects in the production of certain steroids by the ovary or adrenal. There may even be disturbances in the liver or kidney metabolism, which may alter the nature or rate of steroid excretion.
However, “sexual hair”, i.e. facial, ancillary, chest, pubic hair, Is directly related to the production by the glands of internal secretion.
It should be noted in passing that certain stresses of life can greatly alter hair, growth patterns, at least temporarily in some cases.
The electrolysis practitioner would do well to steel herself to these possibilities in order to avoid chaos during treatment or anger when promises made we’re not able to be kept.
Oral Contraceptives (Pg. 97-103)
Androgens: a male hormone. Maybe be strong or weak.
Estrogen: a female hormone.
Familial or idiopathic: occurring in families without a parent hormonal cause.
Progesterone: a natural hormone produced in the ovary after ovulation, and then the placenta during pregnancy; opposes the effect of androgens.
Testosterone: a potent male hormone present and serum.
Iatric: linked to drugs or medication
Sex Hormones, Drugs and Superfluous Hair (Pg.105-119)
Minoxidil, which is used for kidney failure, patience, and the treatment of severe high blood pressure, and finasteride for the treatment of alopecia, are also known to be hair growth stimulators.
The sex hormones fall, mainly into three classes: androgens, the male hormones, i.e. testosterone, and two groups of female hormones, the estrogen, and the progesterone.
Androgens
Androgens, the so-called “male hormones“ stimulate the hair follicles, and the sebaceous glands and are responsible for changing fine, vellus hairs into thick terminal hairs.
Corticosteroids and hair growth
Prednisone is a synthetic steroid derived from Cortisone. Its effects are much the same, except that it causes less sodium and water retention. It is linked to excess hair and hyperpigmentation.
Hair growth as a side effect of medication
Excessive hair growth that can be directly attributed to medical drug therapy is called iatric hirsutism. Iatric being a Greek word pertaining to medicine or to a physician.
Drugs and hormones
The pattern of hair growth for a young male is the same as that of the female, until puberty, when higher concentrations of the so-called “male sex hormones“ which are present in both men and women, and hereditary conspire to expand the sexual hair of the man to include the upper lip, beard area, neck, and escutcheon (scrotum in Latin).
The hair of the scalp, eyebrows and eyelashes is mostly androgen independent, meaning that it is not totally reliant on the male hormones For its growth. The opposite is true for the sexual hair that appears at puberty. It is very dependent on androgens, especially testosterone, the major hormone affecting the growth of hair.
Conclusion
However, course, thick, and pigmented hair on the face are generally a sign of androgen excess. Obviously, the fact that the patient has observed hirsutism in female family members does not mean the cause of the hirsutism in their family is not related to androgens.
The androgen receptors in the skin of some hirsute women are more sensitive to normal amounts of androgens. These women may have normal hormonal test, but will be helped by taking anti-androgens.
Skin and Hair Anatomy Test Questions
Multiple Choice Questions
What is the largest organ of the body?
a) Liver
b) Heart
c) Skin
d) Lungs
What are the main layers of skin?
a) Epidermis, Dermis, Subcutaneous
b) Epidermis, Dermis, Muscle
c) Dermis, Fat, Muscle
d) Epidermis, Fat, Bone
The outermost layer of the epidermis is called:
a) Stratum Germinativum
b) Stratum Lucidum
c) Stratum Corneum
d) Stratum Granulosum
Which layer of the skin contains live cells and is responsible for cell division?
a) Stratum Corneum
b) Stratum Granulosum
c) Stratum Spinosum
d) Stratum Basale
What pigment gives skin its color?
a) Carotene
b) Hemoglobin
c) Melanin
d) Chlorophyll
The dermis is primarily composed of:
a) Epithelial tissue
b) Connective tissue
c) Muscle tissue
d) Nervous tissue
Which layer of skin is responsible for thermoregulation?
a) Epidermis
b) Dermis
c) Subcutaneous layer
d) Hypodermis
What type of hair is predominantly found on the body before puberty?
a) Terminal hair
b) Vellus hair
c) Lanugo
d) All of the above
Which cells in the epidermis protect against UV radiation?
a) Keratinocytes
b) Melanocytes
c) Langerhans cells
d) Adipocytes
The main function of sebaceous glands is to:
a) Sweat production
b) Lubricate skin and hair
c) Produce melanin
d) Form hair follicles
The hair follicles are primarily found in which layer of the skin?
a) Epidermis
b) Dermis
c) Subcutaneous layer
d) All layers
What type of sweat gland is primarily involved in temperature regulation?
a) Apocrine
b) Eccrine
c) Sebaceous
d) Holocrine
Which of the following is a characteristic of the stratum lucidum?
a) Found only on thick skin
b) Contains living cells
c) Thickest on eyelids
d) Darkly pigmented
What is responsible for the 'goosebumps' effect?
a) Sebum
b) Hair follicles
c) Arrector pili muscle
d) Sweat
The main component of the hair shaft is:
a) Keratin
b) Collagen
c) Elastin
d) Melanin
Which layer provides cushioning against injury?
a) Epidermis
b) Dermis
c) Subcutaneous layer
d) Stratum Granulosum
Hirsutism is defined as:
a) Excessive hair growth in women
b) Absence of hair
c) Inflammation of hair follicles
d) Normal hair growth
The process of shedding dead skin cells is known as:
a) Excretion
b) Desquamation
c) Secretion
d) Absorption
Which of the following is NOT a function of the skin?
a) Protection
b) Absorption
c) Respiration
d) Sensation
What determines the color of hair?
a) Melanin in the cortex
b) Sebum in the follicle
c) Blood flow in the dermis
d) Piloerector muscle
How long does it typically take for the epidermal tissue to be replaced?
a) 14 days
b) 28 days
c) 42 days
d) 56 days
What is the primary role of Langerhans cells?
a) Produce melanin
b) Maintain skin hydration
c) Provide immune response
d) Sense touch
Which type of hair develops during puberty?
a) Vellus hair
b) Terminal hair
c) Lanugo
d) None of the above
The hypodermis is also known as:
a) Epidermis
b) Adipose layer
c) Dermis
d) Basal layer
Which type of sweat gland is associated with body odor?
a) Eccrine
b) Apocrine
c) Sebaceous
d) Merocrine
The dermal papillae play a significant role in:
a) Sensation
b) Blood circulation
c) Hair growth
d) All of the above
The acid mantle of the skin is made up of:
a) Lipids and sebum
b) Sweat and oils
c) Melanin
d) Both a and b
Which microscope is suitable for viewing skin layers?
a) Light microscope
b) Scanning electron microscope
c) Transmission electron microscope
d) Fluorescent microscope
The phase of hair growth that lasts for the shortest duration is:
a) Anagen
b) Catagen
c) Telogen
d) all phases last the same
What forms the base of the hair bulb?
a) Arrector pili
b) Papillae
c) Stratum lucidum
d) Follicular canal
Melanocytes are primarily located in which layer?
a) Stratum corneum
b) Stratum granulosum
c) Stratum basale
d) Dermis
Which of the following best describes apocrine glands?
a) Present in high numbers everywhere
b) Open into hair follicles
c) Secretes a thin, clear fluid
d) Prevents skin drying
What layer of skin is absent on the eyelids?
a) Stratum corneum
b) Stratum lucidum
c) Stratum granulosum
d) Stratum spinosum
What is the primary function of adipose tissue in the hypodermis?
a) Allow skin to breathe
b) Insulate the body
c) Produce hormones
d) Protect against UV light
Which skin condition is caused by a virus?
a) Acne
b) Herpes
c) Psoriasis
d) Eczema
What is the main ingredient in hair?
a) Soft keratin
b) Hard keratin
c) Collagen
d) Elastin
Which skin cell type is primarily responsible for moisture retention?
a) Keratinocytes
b) Fibroblasts
c) Adipocytes
d) Melanocytes
Sebum is used to:
a) Dry the skin
b) Lubricate the skin
c) Produce sweat
d) Block UV rays
Which condition is characterized by excessive pigmentation?
a) Albinism
b) Melasma
c) Vitiligo
d) Eczema
What is the cycle through which hair grows called?
a) Follicle cycle
b) Hair cycle
c) Anagen cycle
d) Hair growth cycle
What is the primary purpose of the dermis?
a) Sensation
b) Protection
c) Hair growth
d) Temperature regulation
What connects the epidermis and dermis?
a) Follicular canal
b) Basement membrane zone (BMZ)
c) Collagen fibers
d) Sebaceous glands
Which hair type is fine and light-colored?
a) Terminal hair
b) Vellus hair
c) Lanugo
d) All of the above
The thickest skin on the body is found on:
a) Palms of hands
b) Eyelids
c) Back of the neck
d) Underarms
The function of the stratum corneum is to:
a) Absorb nutrients
b) Protect against water loss
c) Regulate temperature
d) Provide blood supply
What type of hair is typically hormonally influenced?
a) Vellus hair
b) Terminal hair
c) Lanugo
d) All hair
Which type of hair is known as 'peach fuzz'?
a) Terminal hair
b) Lanugo
c) Vellus hair
d) All of the above
Which gland is NOT part of the pilosebaceous unit?
a) Sebaceous glands
b) Hair follicles
c) Sudoriferous glands
d) Adipocytes
Skin cancer can develop from which layer?
a) Dermis
b) Subcutaneous
c) Epidermis
d) All layers
Which layer is predominantly made of elastic fibers?
a) Papillary layer
b) Reticular layer
c) Epidermis
d) Air layer
The thinning of hair is known as:
a) Alopecia
b) Hirsutism
c) Hypertrichosis
d) Seborrhea
Which of the following isn’t a characteristic of eccrine glands?
a) They regulate body temperature
b) They are found everywhere on the body
c) They produce thick, yellowish fluid
d) They help with moisture
The basic structure of hair includes:
a) Cuticle, cortex, medulla
b) Dermis, epidermis, subcutis
c) Papilla, shaft, root
d) None of the above
The primary component of the hair cuticle is:
a) Soft keratin
b) Hard keratin
c) Collagen
d) Melanin
Skin disorders may begin as small bumps or irritated patches typically associated with:
a) Bacteria
b) Viruses
c) Fungus
d) All of the above
How does the skin help in Vitamin D synthesis?
a) Absorbing sunlight
b) Producing melanin
c) Regulating skin pH
d) Protecting from UV rays
Hypertrichosis is characterized by:
a) Increased hair growth
b) Hair loss
c) Irregular hair patterns
d) Puberty-related hair changes
The bulge region of hair follicles is associated with:
a) Stem cell activity
b) Melanocyte activity
c) Dermal papilla growth
d) Sebaceous secretion
In which hair phase does hair shed?
a) Anagen
b) Catagen
c) Telogen
d) All phases
What is the term for the loss of hair growth capability?
a) Alopecia
b) Hypertrichosis
c) Hirsutism
d) None of the above
Eccrine glands are most active:
a) During cold weather
b) Under stress
c) When the body is hot
d) While sleeping
Most of the body's cutaneous sensory receptors are found in which layer?
a) Epidermis
b) Dermis
c) Subcutaneous layer
d) Stratum lucidum
Which phase is also referred to as the involution phase?
a) Anagen
b) Catagen
c) Telogen
d) Follicular
What is the primary role of the arrector pili muscle?
a) Lubricate hair
b) Control skin temperature
c) Cause hair to stand up
d) Promote hair growth
The acid mantle of the skin is primarily due to:
a) Sweat and sebum
b) Melanin production
c) Blood flow
d) Keratin
What skin layer is critical for holding blood vessels?
a) Epidermis
b) Dermis
c) Subdermal
d) Subcutaneous
Melanocytes are predominantly located in:
a) Stratum corneum
b) Stratum germinativum
c) Dermis
d) Hypodermis
What type of hair is typically found on the scalp?
a) Lanugo
b) Terminal hair
c) Vellus hair
d) All of the above
Which skin function protects against pathogens?
a) Absorption
b) Protection
c) Secretion
d) Thermoregulation
What is the role of the dermal papilla?
a) Producing sebum
b) Nourishing hair follicles
c) Acting as a barrier
d) Sensation
The process of keratinization is primarily observed in which skin layer?
a) Epidermis
b) Dermis
c) Reticular layer
d) Papillary layer
What type of glands are sebaceous glands?
a) Eccrine
b) Apocrine
c) Holocrine
d) Exocrine
What does the hair matrix produce?
a) Skin
b) Nails
c) Hair
d) Sebum
The specifics of hair texture are primarily determined by:
a) Genetics
b) Health
c) Environmental factors
d) All of the above
The skin's ability to regulate temperature is achieved through:
a) Blood flow
b) Sweat production
c) Both a and b
d) None of the above
Cellular activity in the bulge region of hair follicles is crucial for:
a) Inducing telogen phase
b) Hair regeneration
c) Producing oils
d) Skin healing
Which of the following substances prevents the skin from drying out?
a) Water
b) Sebum
c) Keratin
d) Sweat
The main function of the papillary layer is to:
a) Protect UV radiation
b) Provide strength
c) Nourish the epidermis
d) Store fat
Excessive hair growth in women is known as:
a) Hypertrichosis
b) Hirsutism
c) Alopecia
d) Epidermis
The primary reason for hair to change color is:
a) Lack of nutrients
b) Aging process
c) Hormonal changes
d) All of the above
Skin's protective barrier is mainly maintained by:
a) Melanin
b) Keratin
c) Both a and b
d) Adipose tissue
Which layer of skin is primarily avascular (lacks blood vessels)?
a) Epidermis
b) Dermis
c) Subcutaneous layer
d) Both b and c
Which hair phase is considered the resting phase?
a) Telogen
b) Anagen
c) Catagen
d) Growing phase
The primary role of keratin in the skin is to:
a) Provide strength
b) Help with sensation
c) Control moisture
d) Maintain blood flow
Sebaceous glands are primarily found in association with:
a) Sweat glands
b) Hair follicles
c) Adipocytes
d) All the above
Which hair type is mostly affected by hormonal changes?
a) Vellus
b) Terminal
c) Lanugo
d) All types
The majority of skin cancers arise from the:
a) Dermis
b) Subcutaneous layer
c) Epidermis
d) Hypodermis
Hair is said to be a derivative of which layer of skin?
a) Dermis
b) Epidermis
c) Subcutaneous layer
d) All layers
The term for skin inflammation is:
a) Dermatitis
b) Eczema
c) Psoriasis
d) Fungal infection
In terms of hair growth, which phase is when the follicle remains active?
a) Anagen
b) Catagen
c) Telogen
d) Resting
Excessive oil production in the skin can lead to:
a) Dry skin
b) Oily skin
c) Eczema
d) All of the above
Which structure performs a significant role in temperature regulation?
a) Sweat glands
b) Sebaceous glands
c) Dermis
d) Epidermis
What determines whether hair is straight, wavy, or curly?
a) Hair color
b) Hair texture
c) Follicle shape
d) Hair length
Skin cancer should be monitored especially when moles appear:
a) Black and large
b) Unchanged
c) Brown and small
d) Lighter than skin
What is the role of the reticular layer of the dermis?
a) Provides nutrients
b) Offers strength and elasticity
c) Contains sweat glands
d) All of the above
The impact of hormones primarily associates with:
a) Skin elasticity
b) Hair growth and texture
c) Immune functions
d) None of the above
A decrease in vellus hair usually happens:
a) Due to aging
b) Post-puberty
c) After menopause
d) All of the above
Which condition can occur due to reduced blood circulation?
a) Acne
b) Psoriasis
c) Dermatitis
d) Folliculitis
The phase of the hair cycle known for the most active hair growth is:
a) Anagen
b) Telogen
c) Catagen
d) Quiescent
The primary component responsible for skin hydration is:
a) Water
b) Lipids
c) Collagen
d) Keratin
Answer Guide with Explanations
c) Skin The skin is the largest organ of the body, covering an area of about 20 square feet.
a) Epidermis, Dermis, Subcutaneous These are the three main layers of skin.
c) Stratum Corneum This is the outermost layer of the epidermis, consisting of dead skin cells.
d) Stratum Basale This is the deepest layer where live cells and cell division occurs.
c) Melanin Melanin is the pigment produced by melanocytes that gives skin its color.
b) Connective tissue The dermis is primarily made of dense connective tissue, providing strength and elasticity.
b) Dermis The dermis contains sweat glands and blood vessels that help regulate body temperature.
b) Vellus hair Vellus hair is fine hair that covers much of the human body before puberty.
b) Melanocytes Melanocytes in the epidermis produce melanin, which protects against UV radiation.
b) Lubricate skin and hair Sebaceous glands secrete sebum, an oily substance that lubricates the skin and hair.
b) Dermis Hair follicles are embedded in the dermal layer of skin.
b) Eccrine Eccrine sweat glands are responsible for regulating body temperature through sweat.
a) Found only on thick skin The stratum lucidum is a clear layer found on the palms and soles, not present on thin skin.
c) Arrector pili muscle This muscle contracts in response to cold or fear, causing hair to stand upright and producing 'goosebumps.'
a) Keratin The hair shaft is mainly composed of hard keratin, a fibrous protein.
c) Subcutaneous layer This layer contains fat that acts as cushioning and insulation for the body.
a) Excessive hair growth in women Hirsutism is characterized by thick, dark hair growth in areas typical for males.
b) Desquamation The shedding of dead skin cells is termed desquamation.
c) Digestion The skin protects against external factors, absorbs specific substances, but does not aid in digestion.
c) Melanin in the cortex The color of hair is primarily determined by the amount and type of melanin present in the cortex.
b) 28 days Typically, it takes about 28 days for the epidermis to completely renew itself.
c) Provide immune response Langerhans cells are immune cells in the skin that help recognize and fight infections.
b) Terminal hair Terminal hair begins to develop during puberty under the influence of androgens.
b) Adipose layer The hypodermis is also known as the adipose layer due to its fat content.
b) Apocrine Apocrine glands secrete a thicker fluid that can lead to body odor when mixed with bacteria.
d) All of the above Dermal papillae are involved in sensation, maintaining blood supply, and supporting hair growth.
d) Both a and b The acid mantle consists of sweat and sebum, which help protect the skin from bacteria.
a) Light microscope Light microscopes are commonly used to observe cellular structures in skin layers.
b) Catagen Catagen is the transitional phase that lasts for a short duration (days to weeks).
b) Papillae The base of the hair bulb is formed by the dermal papillae, which nourish the hair.
c) Stratum basale Melanocytes are primarily found in the stratum basale, the deepest layer of the epidermis.
b) Open into hair follicles Apocrine glands open into hair follicles, while eccrine glands open directly to the skin surface.
b) Stratum lucidum The stratum lucidum is absent in thin skin like on the eyelids.
b) Insulate the body Adipose tissue in the hypodermis helps insulate and protect the body.
b) Herpes Herpes is caused by a virus, leading to blisters and sores.
b) Hard keratin Hair is made of hard keratin, which provides strength.
a) Keratinocytes Keratinocytes are responsible for moisture retention in the skin.
b) Lubricate the skin Sebum helps keep the skin and hair lubricated, preventing dryness.
b) Melasma Melasma involves excess pigmentation associated commonly with hormonal changes.
d) Hair growth cycle The hair growth cycle consists of anagen, catagen, and telogen phases.
b) Protection The dermis provides structure and strength to the skin, including protections against physical forces.
b) Basement membrane zone The basement membrane connects the epidermis and dermis, providing structural support.
b) Vellus hair Vellus hair is fine and light-colored, often referred to as “peach fuzz.”
a) Palms of hands The thickest skin is found on the palms of the hands and soles of the feet.
b) Protect against water loss The stratum corneum acts as a barrier to prevent water loss from the body.
b) Terminal hair Terminal hair is significantly affected by androgens and hormonal changes.
c) Vellus hair Vellus hair is often described as soft, light, and barely noticeable hair on the body.
d) Adipocytes Adipocytes are fat cells and are not part of the pilosebaceous unit, which consists of hair follicles, sebaceous glands, and sometimes sweat glands.
c) Epidermis Many skin cancers, such as basal cell carcinoma, arise from epidermal cells.
b) Reticular layer The reticular layer is comprised of dense connective tissue, which provides elasticity and strength to the skin.
a) Alopecia Alopecia is the medical term for hair loss.
c) They produce thick, yellowish fluid Eccrine glands secrete a thin, clear fluid, not thick or yellowish; that characteristic pertains to apocrine glands.
a) Cuticle, cortex, medulla These are the three basic layers of hair.
b) Hard keratin The cuticle is primarily made of hard keratin, which protects the inner layers of the hair.
d) All of the above Skin disorders can stem from bacterial, viral, or fungal infections.
a) Absorbing sunlight The skin synthesizes vitamin D when exposed to sunlight.
a) Increased hair growth Hypertrichosis refers to abnormal hair growth, while hirsutism specifically refers to excess male-pattern hair growth in women.
a) Stem cell activity The bulge region of hair follicles contains stem cells that can regenerate hair.
c) Telogen Hair sheds during the telogen phase, which is the resting phase before new growth.
a) Alopecia Alopecia refers to the loss of hair growth capability or balding.
c) When the body is hot Eccrine glands are most active to help cool the body down through perspiration.
b) Dermis Most sensory receptors are located in the dermis, including touch and pressure receptors.
b) Catagen The catagen phase is the transitional phase during which hair stops growing and prepares for shedding.
c) Cause hair to stand up The arrector pili muscle contracts, making hair stand up (goosebumps). It assists in temperature regulation.
d) Sweat and sebum The acid mantle forms from the combination of sweat (a weak acid) and sebum (from sebaceous glands).
b) DermisThe dermis contains blood vessels that supply nutrients to the skin.
b) Stratum germinativum Melanocytes, which produce melanin, are primarily located in the basal layer of the epidermis.
b) Terminal hair Terminal hair, which is thick and pigmented, covers the scalp and is typically found on other areas influenced by hormones.
b) Protection Skin protects against pathogens by acting as a barrier and utilizing immune cells within the dermis and epidermis.
b) Nourishing hair follicles The dermal papilla provides blood supply, essential for hair growth and nourishment.
a) Epidermis Keratinization occurs primarily in the epidermis, particularly in the stratum corneum.
d) Exocrine Sebaceous glands are exocrine glands, which release their secretions onto the surface of the skin through ducts.
c) Hair The hair matrix consists of rapidly dividing cells that produce hair.
a) Genetics Hair texture is largely determined by genetic factors, as well as hormonal influences and environmental factors.
c) Both a and b The skin regulates temperature through blood flow and sweat production, maintaining homeostasis.
b) Hair regeneration Cellular activity in the bulge region is important for the regeneration of hair follicles during hair cycling.
b) Sebum Sebum prevents the skin from drying out by providing lubrication and moisture retention.
c) Nourish the epidermis The papillary layer of the dermis provides nutrients to the epidermis through capillaries.
b) Hirsutism Hirsutism is characterized by excessive hair growth in areas typical for males, like the face and chest.
b) Aging process Changes in hair color, including graying, are commonly associated with aging and hormonal changes.
c) Both a and b The skin's protective barrier is maintained by keratin (providing strength) and melanin (protecting from UV radiation).
a) Epidermis The epidermis is primarily avascular; it does not contain blood vessels, relying on the dermis for nutrients.
a) Telogen Telogen is the resting phase in which the hair follicle is inactive, before hair shedding starts.
a) Provide strength Keratin's primary role in skin and hair is to provide structural strength and integrity.
b) Hair follicles Sebaceous glands are closely associated with hair follicles, where they secrete sebum.
b) Terminal Terminal hair is the type most influenced by hormonal fluctuations during puberty, pregnancy, and other life stages.
c) Epidermis Most skin cancers arise from cells in the epidermis, particularly from the basal or squamous cells.
b) Epidermis Hair is a derivative of the epidermis, growing from hair follicles that are extensions of this layer.
a) Dermatitis Dermatitis refers to any inflammation of the skin, which can result from multiple causes, including irritants or allergens.
a) Anagen Anagen is the active growth phase during which hair follicles actively produce hair.
b) Oily skin Excessive oil production commonly leads to oily skin, which can contribute to acne and other skin issues.
a) Sweat glands Sweat glands, particularly eccrine glands, play a significant role in temperature regulation through sweat production.
c) Follicle shape The shape of the hair follicle determines whether the hair is straight (round), wavy (oval), or curly (flat).
a) Black and large Moles that are black, large, asymmetrical, or change in size or color should be monitored as potential indicators of skin cancer.
b) Offers strength and elasticity The reticular layer of the dermis contains dense connective tissue that provides strength and elasticity to the skin.
b) Hair growth and texture Hormonal changes can significantly affect hair growth rates and textures, particularly during puberty or menopause.
d) All of the above A decrease in vellus hair is common due to aging, post-puberty changes, or after menopause.
c) Dermatitis Reduced blood circulation can lead to various skin conditions, including dermatitis due to poor nutrient delivery.
a) Anagen The anagen phase is known for the most active hair growth, during which the hair follicle is firmly attached.
a) Water Water is the primary component responsible for skin hydration; maintaining skin moisture is crucial for health.