Cardiac muscle & Conducting system_241105
Certainly! Here’s a more detailed summary based on each section of the slides on the Cardiac Muscle and Conducting System:
In-depth Summary
Learning Objectives:
Identify excitable tissues in the heart.
Describe the cardiac muscle's electrical and mechanical properties.
Explain the ionic basis of automaticity in cardiac muscle cells.
Detail the origin and spread of cardiac excitation.
Illustrate the cardiac conduction system.
Differentiate normal and abnormal excitation patterns.
Identify factors affecting cardiac electrical activity.
The Medical Significance:
Understanding the cardiac muscle's electrical activity is crucial for interpreting normal heart function and managing heart disease.
Blood Flow Circuit:
The heart’s circulatory system comprises:
Pulmonary Circulation: Blood flows from the heart to the lungs for oxygenation.
Systemic Circulation: Oxygenated blood is distributed throughout the body.
These cycles are regulated by cardiac rhythmicity, the mechanism by which the heart generates and propagates action potentials, creating a regular heartbeat.
Electrical Activity of the Heart:
The heart has automaticity a property called auto-rythmicity, meaning it can initiate action potentials independently:
Contractile Cells: Make up 99% of the heart muscle and perform mechanical contractions . Do not initiate own action potentials.
Autorhythmic Cells(nodal cells): Specialized cells that generate and conduct electrical signals, forming the basis of heart rhythms. Unlike contractile cells, they do not contract but are key to initiating and regulating heartbeat.
Cardiac Muscle Structure:
Cardiac muscle shares some structural features with skeletal muscle:
Striated with actin and myosin filaments but operates involuntarily, like smooth muscle.
Branched Fibers: The muscle fibers interconnect at intercalated discs, which enable rapid ion diffusion across cells via gap junctions.
Functional Syncytium: The gap junctions allow the entire heart muscle to function as a unit, so an impulse can spread quickly across all fibers.
The heart is divided into two functional syncytia:
Atrial Syncytium: Comprises the two atrial walls.
Ventricular Syncytium: Comprises the two ventricular walls.
The division allows the atria to contract just before the ventricles, ensuring efficient blood flow and optimal cardiac output.
Spread of action potential through cardiac muscle
The cardiac muscle acts as a physiological syncytium due to the presence of gap junctions amongst the cardiac muscle fibres.
Because of this, the action potential spreads through the cardiac muscles very rapidly. ❑
There are two syncytia (the atrial and the ventricular) in the heart.
Action potential is transmitted from atria to ventricles only through the fibres of specialized conductive system.
Key Properties of Cardiac Muscle Cells:
Automaticity: Ability to self-initiate action potentials.
Rhythmicity: Generation of action potentials at regular intervals.
Conductivity: Transfer of action potentials from one cell to another.
Excitability: Response to electrical stimuli by generating action potentials.
Contractility: Force generation in response to electrical stimulus, enabling the heart muscle to contract and pump blood.
Cardiac Conduction System:
The heart’s conduction system consists of nodes and fibers that ensure proper spread of electrical impulses:
Sinoatrial (SA) Node: The heart’s primary pacemaker located in the right atrium. It initiates electrical impulses, setting the pace for the heart.
Atrioventricular (AV) Node: Located near the junction of the atria and ventricles. It receives impulses from the SA node and delays them to allow the atria to contract fully before ventricular contraction.
Bundle of His: Transmits impulses from the AV node to the ventricular muscles. It splits into the right and left bundle branches within the interventricular septum.
Purkinje Fibers: Branches from the Bundle of His that spread impulses through the ventricles, allowing for rapid, coordinated contraction.
This conduction system coordinates the heartbeat by ensuring a sequential contraction of the atria and ventricles.
Pacemaker Potential and Ionic Mechanisms:
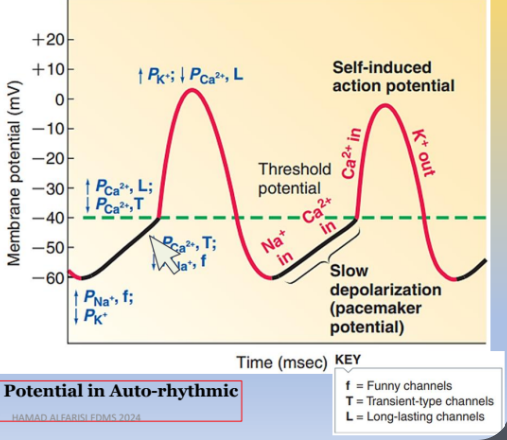
Autorhythmic cells have a unique pacemaker potential that gradually depolarizes the membrane until threshold is reached:
Sodium (Na+) Influx: Increased inward flow of Na+ ions through "funny" channels, unique to pacemaker cells.
Potassium (K+) Efflux Decrease: A progressive reduction in K+ outflow prolongs depolarization.
Calcium (Ca2+) Influx: Entry of Ca2+ ions also contributes to the depolarization, pushing the cell toward the threshold.
Once threshold is reached, the rising phase of action potential occurs due to Ca2+ entry through L-type Ca2+ channels, leading to cell depolarization.
Atrioventricular nodal (AV node) delay
The atrioventricular nodal delay is a very crucial mechanism for coordinated and synchronized cardiac function.
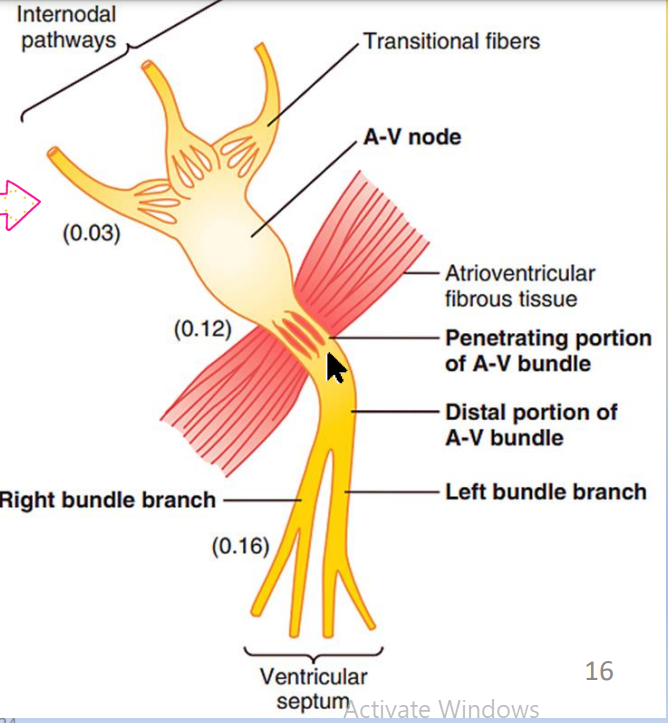
The impulse, after traveling through the internodal pathways, reaches the A-V node about 0.03 second after its origin in the sinus node
Then there is a delay of another 0.09 second in the A-V node itself.
A final delay of another 0.04 second occurs mainly in the penetrating A-V bundle.
The total delay in the A-V nodal and A-V bundle system is about 0.13 second.
Total delay of 0.16 second before the excitatory signal reaches the contracting muscle of the ventricles .
Action Potential in Contractile Cells:
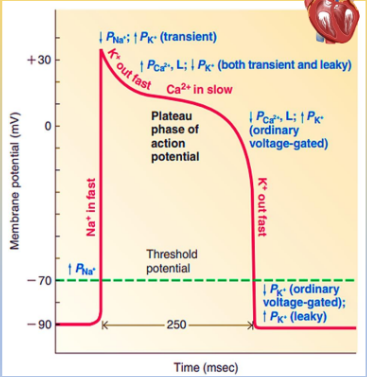
Contractile cells’ action potential is key to muscle contraction and is divided into distinct phases:
Depolarization (Phase 0): Rapid Na+ influx due to voltage-gated Na+ channels opening.
Initial Repolarization (Phase 1): Brief K+ efflux as Na+ channels close.
Plateau Phase (Phase 2): Sustained Ca2+ influx and reduced K+ efflux prolong depolarization, essential for continuous contraction.
Repolarization (Phase 3): Ca2+ channels close and K+ channels reopen, leading to a return to resting potential.
Resting Membrane Potential (Phase 4): The membrane returns to its stable resting potential, facilitated by the Na+-K+ pump.
The plateau phase of the action potential is critical, as it allows for prolonged contraction, ensuring efficient blood ejection from the ventricles.
Refractory Period in Cardiac Muscle:
The refractory period prevents immediate re-excitation, allowing the heart to fully contract and then relax before the next contraction. It lasts about 0.25-0.30 seconds in the ventricles and 0.15 seconds in the atria.
Autonomic Regulation:
Autonomic nervous system influences regulate heart rate:
Sympathetic Stimulation: Increases SA node discharge, heart rate, and force of contraction.
Parasympathetic Stimulation: Decreases SA node discharge, slowing the heart rate.