Immunotherapy
LEARNING OBJECTIVES
Define immunotherapy.
Describe how immunotherapy works.
Identify different types of immunotherapy.
Immunotherapy: Treatment that uses certain parts of the immune system to fight disease such as caner. a.k.a biotherapy.
How?
By boosting the body’s immune system in a very general way.
Increase strength of immune system.
Counteract signals produced by cell that suppress the immune response.
Non-Specific immunotherapy
Utilize materials that have modulatory effects on the immune system. Modulatory molecules are usually involved in stimulating macrophages, lymphocytes, and natural killer cells.
e.g ILs, Tumor necrosis facter, erythropoietin.
cytokines → activate immune system → fight cancer.
They can either be used as single agents or in combination therapies to improve the effectiveness of the primary treatment.
Cytokines
Chemicals made by some immune system cells.
Crucial in controlling the growth and activity of other immune system cells and blood cells in the body.
Cytokine inhibitors:
Production can be blocked e.g etanercept for rheumatoid arthritis
Cytokines can be neutralized in circulation e.g infliximab for ulcerative colitis
Specific receptor can be blocked e.g kineret for sepsis and RA
Interleukins
Group of cytokines that act as chemical signals between white blood cells.
IL-2 helps immune system cells grown and divide quickly.
Used in treating kidney cancer.
Interferons
Cytokines that help the body resist viruses and infections.
IFN-alfa, beta and gamma
Alfa stimulates T cells and other immune system cells to attack the cancer. It can also encourage cancer cells to send out chemicals that attract immune system cells to them.
Hep B treatment.
How tumors evade the immune system
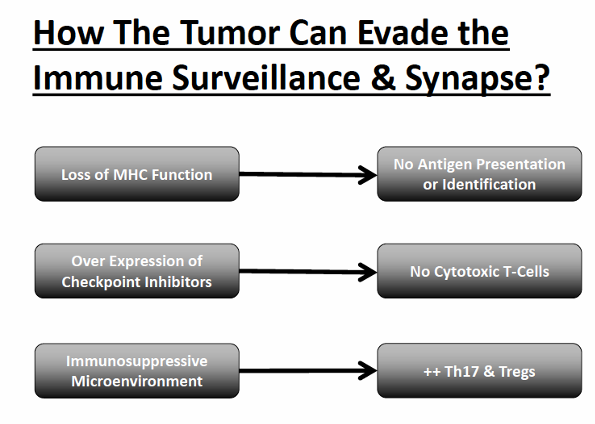
MULTILAYERD IMMUNE SUPPRESION
Tumors insulate themselves with dense layers of immunosuppressive stroma.
Overcoming the many layers of interconnected and often functionally redundant immune suppressive mechanisms represents a challenge for tumor specific T cells.
Immunotherapy can ‘peel back’ the layers of local immune suppression, thereby restoring the capacity of T cells to eradicate the tumor.
PROGRAMMED DEATH-1 IMMUNE CHECKPOINT (PD-1)
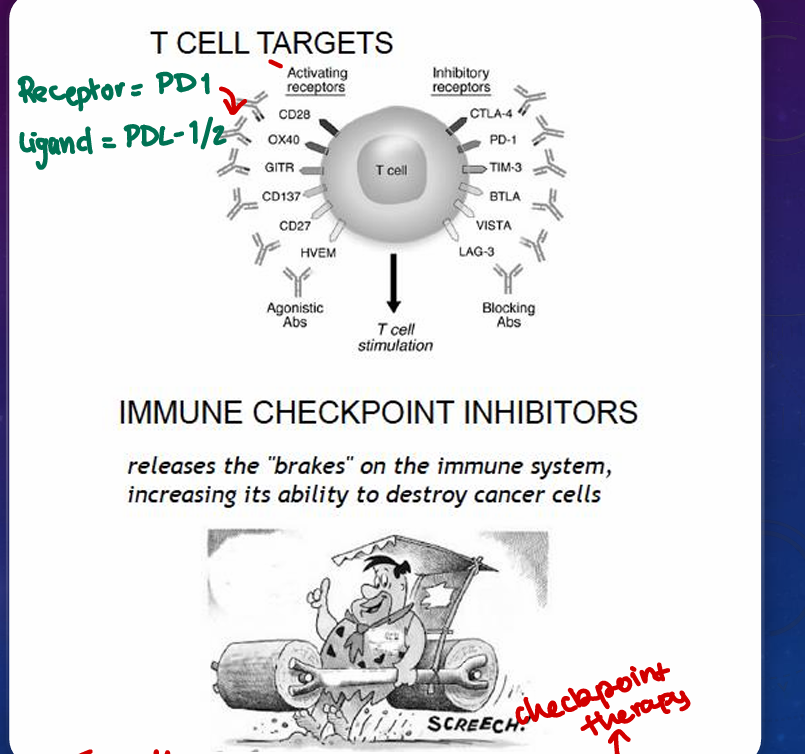
PD-1 (cell receptor) is overexpressed on T cells and these are functionally exhausted cells.
Ligands: PDL1 and PDL2 (tumor cell/APC)
Higher tumoral PDL-1 expression correlates with decreased overall survival.
RATIONALE: Blocking the PD-1 or PDL1 pathway would restore/promote the function of chronically exhausted tumor specific T cells and decrease tumor-induced immune suppression.
Cancer cells have PDL1 (overexpressed) which binds to PD1 on T cells.
This inhibits the T-cell so cancer cells evade the immune system.
Nivolumab and pembrolizumab target PD-1 on activated T cells.
Atezolizumab disrupts the interaction of PD-1 and proteins on the surface of tumor cells (PDL-1 AND 2).
Antibody Based therapies
TYPES OF ANTIBODY BASED THERAPY
NAKED mAbs
Naked mAbs are most widely used e.g Trastuzumab (Herceptin) for breast cancer.
They can have direct and indirect effects.
DIRECT
Producing apoptosis.
Block growth factor receptors and arrest proliferation of tumor cells.
INDIRECT
Recruit cytotoxic cells such as monocytes and macrophages.
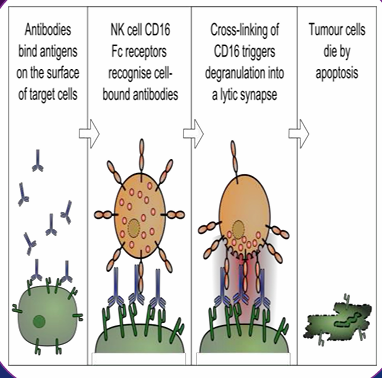
ANTIBODY-DEPENDENT CELL MEDIATED CYTOXICITY (ADCC)
Recruiting non-specific cytotoxic cells such as natural killer cells, macrophages, monocytes and eosinophils.
The Fc gamme receptors (FcyR) on the surface of the immune effector cells bind the Fc region of an antibody, which itself specifically bound to a target cell.
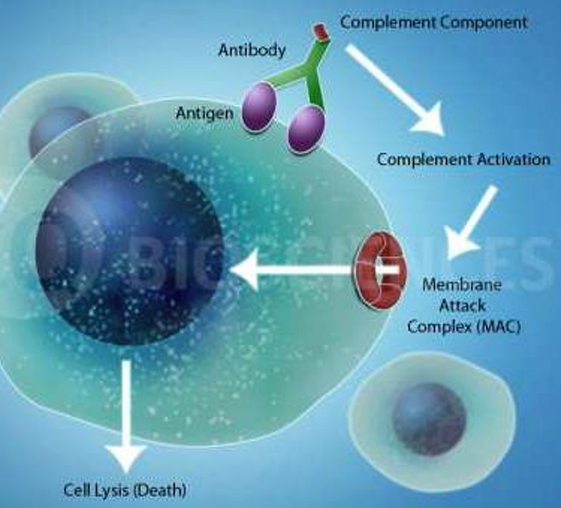
COMPLEMENT DEPENDENT CYTOTOXICITY (CDC)
Monoclonal antibodies also bind to complement, leading to direct cellular toxicity.
In CDC, the C1a binds the antibody and this binding trigger the complement cascade which leads to the formation of the membrane attack complex (MAC).
ANTIBODY CONJUGATES
Antibodies conjugated with traditional therapeutic agents are more potent than naked monoclonal antibodies.
They can be divided into groups depending on what they are linked to:
mAbs with radioactive particles attached are referred to as radiolabeled → radioimmunotherapy (RIT).
They deliver radioactivity directly to cancerous cells and can be used to treat some types of non-Hodgkin lymphoma.
mAbs with chemotherapy drugs attached are referred to as chemo-labeled.
Have powerful chemo attached to them.
Brentuximab for lymphoma and Ado-trastuzumab emtansine for HER2+ Breast cancer.
mAbs attached to cell toxins are called immunotoxins.
Have cell poisons.
ANTIBODY-DIRECTED ENZYME PRO-DRUG THERAPY (ADEPT)
The objective of antibody directed enzyme prodrug therapy is to selectively deliver chemotherapy to cancer sited.
The basic principle is target an enzyme to tumors by attaching it to an antibody directed to a tumor associated antigen.
After clearance of an enzyme from blood, a non-toxic prodrug is given. The targeted enzyme converts a non-toxic prodrug into a potent cell killing agent within tumors to achieve effective therapy without normal tissue toxicity.
IMMUNOGLOBULIN (IVIG)
Contains the pooled IgG extracted from the plasma of over one thousand blood donors.
IVIG’s effects las between 2 weeks and 3 months.
It is mainly used as treatment in 3 major categories:
Immune deficiencies
Autoimmune disease e.g immune thrombocytopenia
Acute infections
SIDE EFFECTS OF MABS
Allergic reaction
Flu like symptoms
Nausea and diarrhoea
skin rashes
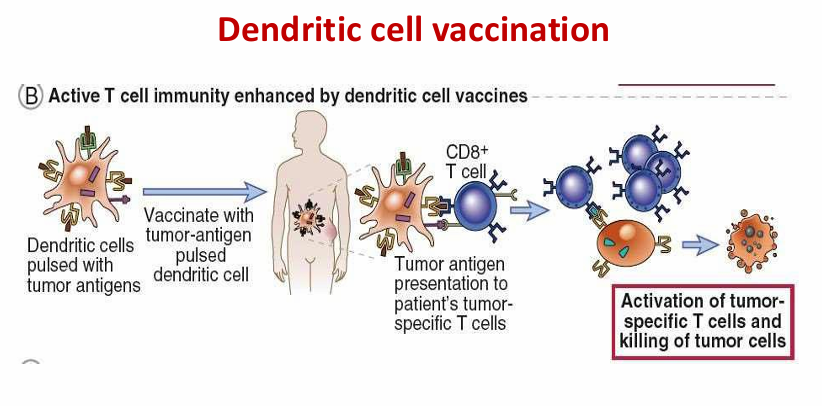
Cancer treatment vaccines
Made from a patient’s own tumor cells to educate T cells to better recognize and kill the pre-existing tumor.
Very expensive.
Dendritic cell vaccination
Adoptive cell transfer (ACT)
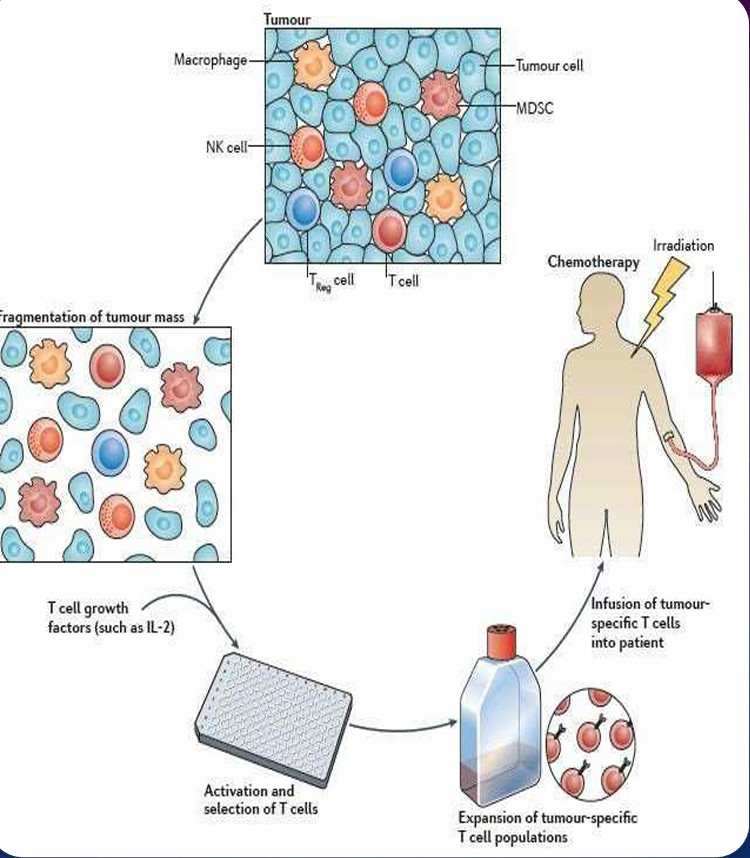
Tumor infiltrating lymphocytes (TILs) with greatest recognition of tumor cells are collected.
These cells are grown in the lab.
Cells are activated by treatment with immune system signaling proteins called cytokines.
Infused into patient.